145 Cushing syndrome
Salient features
Examination
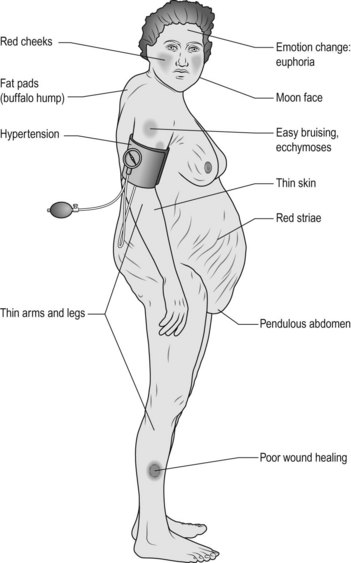
• Moon-like facies (Fig. 145.1), acne, hirsutism and plethora (from telangiectasia).
• Ask the patient whether he or she has back pain and then examine the spine, looking for evidence of osteoporosis and collapse of vertebra, kyphoscoliosis.
• Tell the examiner you would like to:
• Comment on signs of asthma, rheumatoid arthritis, SLE, fibrosing alveolitis (as these are conditions that are treated with long-term steroids).
Questions
How would you investigate such a patient?
Tests to confirm the diagnosis of hypercortisolism:
• Urinary free cortisol as 24-h collection: this is the most direct and reliable practical index of cortisol secretion. The reason is that plasma concentrations of ACTH and cortisol fall and rise episodically, in normal subjects, in Cushing syndrome and in ectopic ACTH syndrome
• Measurement of midnight salivary cortisol levels
Tests to determine the site of hormone production:
• Low-and high-dose dexamethasone test: low-dose dexamethasone fails to suppress urinary steroid secretion in Cushing’s disease whereas high-dose dexamethasone (2 mg every 6 h for 2 days) suppresses at least 50% of urinary steroid secretion
• Chest radiography for carcinoma of the bronchus
• Plain radiograph of the abdomen for adrenal calcification
• Ultrasonography of the abdomen for adrenal tumours
• If Cushing’s disease is suspected:






