• Rarely requires cricopharyngeal myotomy or botulinim toxin injection
DIAGNOSTIC CHECKLIST
• Persistent narrowing or just intermittent indentation
• Smoothly outlined lip-like projection posteriorly at C5-6 level with jet effect seen via narrowed lumen
(Left) Graphic shows hypertrophied contracted cricopharyngeus muscle at the pharyngoesophageal junction (usually near the C5-6 cervical level).
(Right) Lateral view from an esophagram shows a typical appearance of cricopharyngeal achalasia, with a large filling defect along the posterior wall of the pharyngoesophageal junction, at the C5-6 level. Note the distension of the pharynx proximal to this process.
(Left) Lateral film from an esophagram shows a prominent cricopharyngeal “bar” at the C5-6 level in a woman with symptoms of reflux and pills “sticking” in her throat.
(Right) Spot film of the lower esophagus in the same woman shows a hiatal hernia and marked gastroesophageal reflux. Cricopharyngeal achalasia is most often seen in patients with other esophageal disorders, such as reflux esophagitis or motility disorders.
Lateral esophagram shows rounded, hypertrophied cricopharyngeus muscle impinging on the posterior lumen at the pharyngoesophageal junction .
Lateral esophagram shows prominent cricopharyngeus , pharyngeal distention, and an esophageal web .





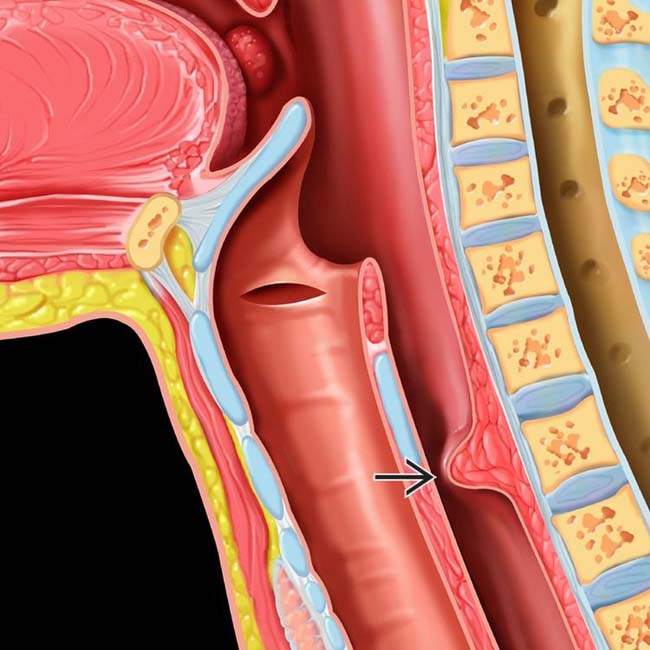
 at the pharyngoesophageal junction (usually near the C5-6 cervical level).
at the pharyngoesophageal junction (usually near the C5-6 cervical level).
 along the posterior wall of the pharyngoesophageal junction, at the C5-6 level. Note the distension of the pharynx
along the posterior wall of the pharyngoesophageal junction, at the C5-6 level. Note the distension of the pharynx  proximal to this process.
proximal to this process.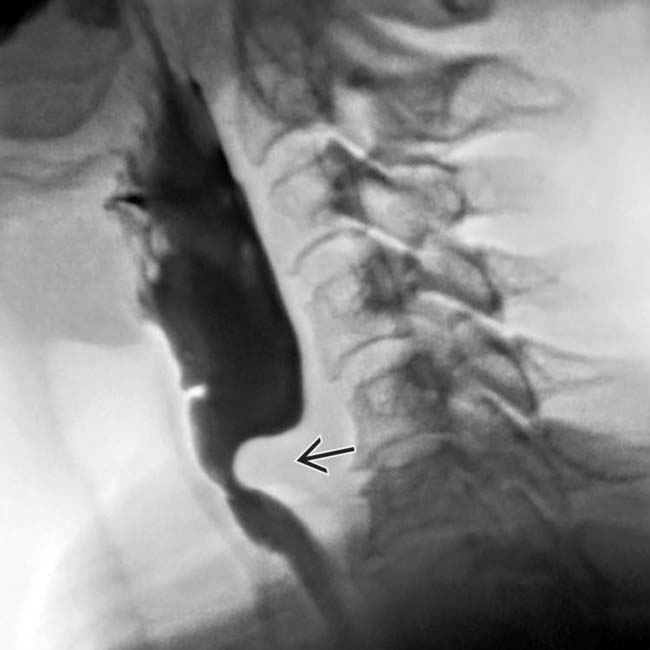
 at the C5-6 level in a woman with symptoms of reflux and pills “sticking” in her throat.
at the C5-6 level in a woman with symptoms of reflux and pills “sticking” in her throat.
 and marked gastroesophageal reflux. Cricopharyngeal achalasia is most often seen in patients with other esophageal disorders, such as reflux esophagitis or motility disorders.
and marked gastroesophageal reflux. Cricopharyngeal achalasia is most often seen in patients with other esophageal disorders, such as reflux esophagitis or motility disorders.
 .
.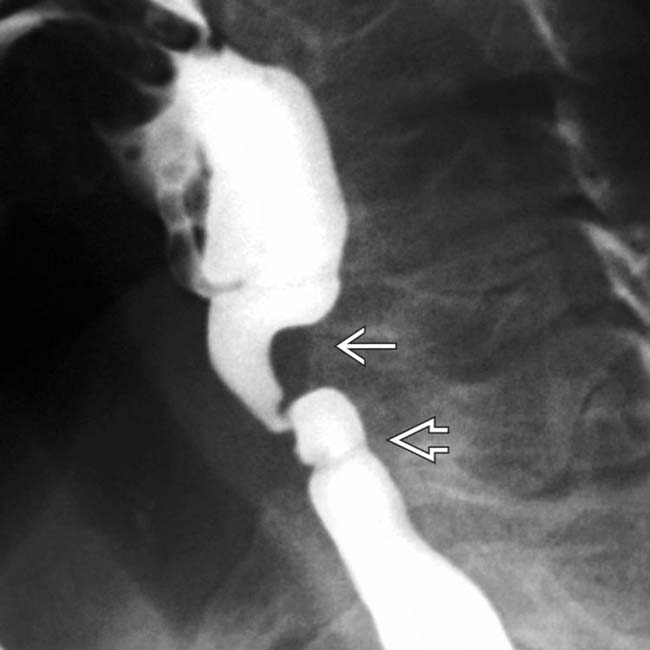
 , pharyngeal distention, and an esophageal web
, pharyngeal distention, and an esophageal web  .
.


