Cranial Nerves
Nystagmus
BACKGROUND
Nystagmus is an oscillation of the eyes. This can be a symmetrical oscillation—pendular nystagmus—or faster in one direction—jerk nystagmus. In jerk nystagmus there is a slow drift in one direction with a fast correction in the opposite direction. It is conventional to describe the nystagmus in the direction of the fast phase. If the oscillation is a twisting movement, this is torsional or rotatory nystagmus.
Nystagmus can be:
WHAT TO DO
Ask the patient to follow your finger with both eyes. Move the finger in turn up, down and to each side. Hold the finger briefly in each position at a point where the finger can easily be seen by both eyes.
Watch for nystagmus. Note:
• the direction of the fast phase—is it in the horizontal plane, in the vertical plane or rotatory?
• the position of the eye when nystagmus occurs and when it is most marked
• whether it affects the abducting eye more than the adducting eye
To decide whether it is central or peripheral, note:
Special test: optokinetic nystagmus (OKN)
This can be tested when a striped drum is spun in front of the eyes; this normally evokes nystagmus in the opposite direction to the direction of spin. This is a useful test for patients with hysterical blindness.
Tests for benign positional vertigo are described in Chapter 12.
WHAT YOU FIND
See Figure 10.1.
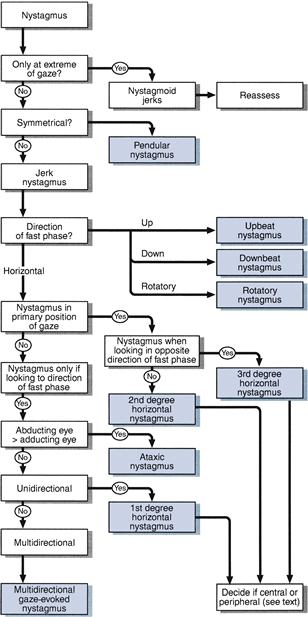
Figure 10.1 Flow chart: nystagmus
Decide whether central or peripheral.
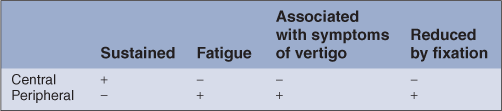
Peripheral nystagmus is not associated with other eye movement abnormalities and usually has a rotatory component.
WHAT IT MEANS
• Rotatory (or rotary) nystagmus:
– Pure rotatory nystagmus = central; peripheral horizontal nystagmus usually has a rotatory component.
• Vertical nystagmus (rare): indicates brainstem disease.
– Upbeat: indicates upper brainstem. Common causes: demyelination, stroke, Wernicke’s encephalopathy.
• Horizontal nystagmus (common):
– Ataxic nystagmus: nystagmus of abducting eye > > adducting eye, associated with internuclear ophthalmoplegia (see Chapter 9). Common causes: multiple sclerosis, cerebrovascular disease.
– unilateral central vestibular syndrome. Common causes: as central vestibular syndromes.
• Unusual and rare eye movement abnormalities:
– Ocular bobbing: eyes drifting up and down in the vertical plane—associated with pontine lesions.