[level-membership-for-internal-medicine-category]
Cough
Cough is a reflex explosive expiration that prevents aspiration and promotes the removal of secretions and foreign particles from the lung.
Causes
Chronic
Productive
• TB (bloodstained) • (common where TB is endemic)
• Pulmonary oedema (pink, frothy)
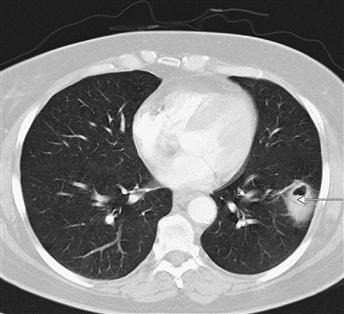
Figure 12 CT thorax showing a left lower lobe non-small-cell lung cancer revealed as a peripheral cavitating mass (arrow).
The patient presented with cough and haemoptysis.
Non-Productive
History
Onset and duration
The onset of a cough may be acute or chronic (usually defined as a cough that has persisted for more than three weeks). Sudden onset of an unrelenting bout of violent coughing may be due to an inhaled foreign body. If this is large enough to occlude the airway, coughing abruptly ceases and is supervened by cyanosis and eventually unconsciousness.
Sputum
The frequency, quantity and appearance of expectorated sputum can be very helpful in the differential diagnosis. Cough continuously productive of purulent sputum is suggestive of chronic bronchitis and bronchiectasis. Expectorated bloodstained sputum tends to be a complaint of patients with bronchogenic carcinoma, pulmonary embolism and TB.
Smoking history
Smoking alone may cause a chronic cough; however, a long smoking history predisposes to bronchogenic carcinoma and chronic bronchitis.
Associated symptoms
Episodic (or even seasonal) wheezing with shortness of breath is common with asthma. This should be differentiated from the monophonic wheeze, which is suggestive of intraluminal obstruction from foreign bodies or tumour.
Most of the respiratory causes of coughing tend to be accompanied by shortness of breath, but sudden onset of dyspnoea may result from aspiration or pulmonary embolism. Shortness of breath that is worse on recumbency is suggestive of pulmonary oedema; however, asthma may also be worse at night. Weight loss can be a prominent feature with lung tumours and TB.
Pleuritic chest pain may be experienced with pulmonary emboli and pneumonia; unrelenting chest pain is more suggestive of bony metastasis from lung cancer. Retrosternal burning chest pain precipitated by posture suggests gastro-oesophageal reflux disease, and the associated cough is due to aspiration of refluxed material. Frequent clearing of the throat due to nasal discharge or a history of allergy with rhinitis may result in post-nasal drip and precipitate coughing.
Examination
Temperature
The presence of pyrexia usually indicates an infective aetiology; the temperature may also be raised with pulmonary embolism.
Inspection and palpation
With COPD, the chest may be barrel-shaped. Patients suffering with lung cancer or TB may appear cachectic. Cyanosis is a feature of pulmonary embolism and COPD. The fingers should be inspected for clubbing (p. 64), which is associated with bronchial carcinoma and bronchiectasis. The JVP is raised in congestive cardiac failure. The supraclavicular nodes may be palpable with respiratory tract infections, TB and lung cancer.
Auscultation
On auscultation, coarse crepitations are a feature of bronchiectasis and pulmonary oedema. Auscultatory features of bronchial carcinoma are non-specific and may manifest as a pleural effusion (dull to percussion, absent breath sounds, decreased vocal resonance) or segmental collapse of the lung. Widespread wheezing is suggestive of asthma, and a fixed inspiratory wheeze may be heard with bronchial luminal obstruction.
General Investigations
■ Sputum cultures
If a productive cough is present, sputum should be sent for cultures. This will include TB-specific cultures and Ziehl–Neelsen staining.
■ Peak flow
Bedside determination of peak expiratory flow rate is useful in the diagnosis of asthma (low peak flow).
■ WCC
A raised WCC is a non-specific indicator of infection, as it may also be raised with pulmonary embolism.
■ CXR
Very useful and may reveal areas of consolidation with infection. Dilated bronchi with persistent areas of infection are suggestive of bronchiectasis. Apical pulmonary consolidation with calcification and hilar lymphadenopathy is characteristic of TB. The presence of pulmonary oedema is appreciated by bilateral patchy shadowing; this may be accompanied by other radiological features of cardiac failure, including cardiomegaly, upper lobe diversion of the pulmonary veins, bilateral pleural effusions and Kerley B lines (1–2 cm horizontal lines in the periphery of the lung fields). Bronchial carcinoma may present as a hilar mass, peripheral mass or with collapse and consolidation of the lung due to airway obstruction. Bilateral hilar lymphadenopathy is suggestive of sarcoidosis.
■ Respiratory function tests
Formal respiratory function tests can be used to diagnose airway obstruction (asthma, chronic bronchitis and bronchiectasis) and flow volume loops may reveal fixed airway obstruction.
Specific Investigations
■ V/Q scan
Indicated when the diagnosis of pulmonary embolism is suspected (especially where CXR is normal).
■ Pulmonary angiography
May be indicated in severely ill patients with suspected pulmonary embolism when surgery or thrombolysis is being considered.
■ CT thorax
Useful for the diagnosis and staging of lung cancer; it is also specific for the diagnosis of bronchiectasis.
■ pH studies
24-hour pH monitoring may be required when a diagnosis of gastro-oesophageal reflux disease cannot be made on the history alone.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
Cough
Cough is a reflex explosive expiration that prevents aspiration and promotes the removal of secretions and foreign particles from the lung.
Causes
Chronic
Productive
• TB (bloodstained) • (common where TB is endemic)
• Pulmonary oedema (pink, frothy)
Figure 12 CT thorax showing a left lower lobe non-small-cell lung cancer revealed as a peripheral cavitating mass (arrow).
The patient presented with cough and haemoptysis.
Non-Productive
History
Onset and duration
The onset of a cough may be acute or chronic (usually defined as a cough that has persisted for more than three weeks). Sudden onset of an unrelenting bout of violent coughing may be due to an inhaled foreign body. If this is large enough to occlude the airway, coughing abruptly ceases and is supervened by cyanosis and eventually unconsciousness.
Sputum
The frequency, quantity and appearance of expectorated sputum can be very helpful in the differential diagnosis. Cough continuously productive of purulent sputum is suggestive of chronic bronchitis and bronchiectasis. Expectorated bloodstained sputum tends to be a complaint of patients with bronchogenic carcinoma, pulmonary embolism and TB.
Smoking history
[/not-level-membership-for-internal-medicine-category]
