Chapter 9 Contact dermatitis
1. Name the two pathogenic types of contact dermatitis.
Contact dermatitis refers to cutaneous inflammation resulting from the interaction of an external agent and the skin. These reactions occur through one of two mechanisms: a nonimmunologic irritant contact dermatitis (ICD) or an immunologic allergic contact dermatitis (ACD). ICD accounts for 80% of all reactions, while ACD is responsible for approximately 20%. Although over 3700 substances have been identified as contact allergens, almost any substance, under the right circumstances, can act as an irritant. It is important to note that irritating compounds can be allergenic, and allergenic compounds can be irritating.
Marks JG, Elsner P, DeLeo VA: Contact and occupational dermatology, ed 3, St Louis, 2002, Mosby.
2. Name the two subtypes of irritant contact dermatitis, and describe them.
ICD can be divided into acute toxic and cumulative insult subtypes. Acute toxic eruptions occur from a single exposure to a strong toxic chemical, such as an acid or alkali, inducing erythema, vesicles, bullae, or skin sloughing. Reactions occur within minutes to hours after exposure, localize to the areas of maximal contact, and have sharp borders. In most cases, healing occurs soon after exposure. Chronic cumulative insult reactions are the more common type of ICD. These are due to multiple exposures of many low-level irritants, such as soaps and shampoos, over time. This dermatitis may take weeks, months, or even years to appear. It is characterized by erythema, scaling, fissuring, pruritus, lichenification, and poor demarcation from the surrounding skin.
3. Explain the pathogenesis of allergic contact dermatitis (ACD).
ACD is a type IV, delayed, cell-mediated, hypersensitivity reaction. Initially, a low-molecular-weight antigen hapten (<500 Daltons) contacts the skin and forms a hapten–carrier protein complex. This complex then associates itself with an epidermal Langerhans’ cell, which presents the complete antigen to a T-helper cell, causing the release of various mediators. Subsequently, T-cell expansion occurs in regional lymph nodes, producing specific memory and T-effector lymphocytes, which circulate in the general bloodstream. This whole process of sensitization occurs in approximately 5 to 21 days. Upon reexposure to the specific antigen, there is proliferation of activated T cells, mediator release, and migration of cytotoxic T cells, resulting in cutaneous eczematous inflammation at the site of contact. This phase occurs within 48 to 72 hours after exposure. Because many allergens are irritants, preceding irritation is common and may enhance allergen absorption. In contrast to irritant reactions, relatively small concentrations of an allergen can be enough to elicit an inflammatory reaction. Acute ACD may have erythema, edema, and vesicle formation. Chronic ACD reactions are scaly, erythematous, possibly lichenified, and can mimic chronic ICD. Table 9-1 compares ACD and ICD.
Table 9-1. Comparison of Irritant and Allergic Contact Dermatitis
| IRRITANT | ALLERGIC | |
|---|---|---|
| Examples | Water, soap | Nickel, fragrance, hair dye |
| Number of compounds | Many | Fewer |
| Distribution of reaction | Localized | May spread beyond area of maximal contact and become generalized |
| Concentration of agent needed to elicit reaction | High | Can be minute |
| Time course | Immediate to late | Sensitization in 2 weeks; elicitation takes 24–72 hrs |
| Immunology | Nonspecific | Specific type IV delayed hypersensitivity reaction |
| Diagnostic test | None | Patch test |
Li L, Cruz P: Allergic contact dermatitis: pathophysiology applied to future therapy, Dermatol Thera 17:219–223, 2004.
4. Can urticarial reactions occur from contact with a substance?
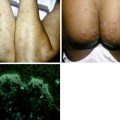
Occasionally, urticarial reactions may occur with certain exposures, instead of the eczematous changes seen with ACD and ICD (Fig. 9-1). Allergic contact urticaria involves a specific IgE–mast cell interaction, resulting in the release of vasoactive compounds. While urticaria occurs at the site of contact, more generalized symptoms can appear, including angioedema, anaphylaxis, rhinoconjunctivitis, and widespread urticaria. A good example is the latex glove immediate reaction reported in health care professionals. Nonimmunologic contact urticaria occurs secondary to a non–antibody-mediated release of vasoactive mediators or due to a direct effect on the cutaneous vasculature. Many agents found in cosmetic products can cause a nonimmunologic contact urticaria. These include sorbic acid, benzoic acid, and cinnamic acid. This may explain the facial burning and stinging that some patients experience using cosmetics. To diagnose contact urticaria, a prick test is usually performed. In this test, a small amount of the allergen is placed on the skin, and a needle is used to prick the skin. An urticarial wheal of appropriate size constitutes a positive test, usually developing within 15 to 20 minutes after allergen administration (Fig. 9-2).

5. Why is the distribution of a contact dermatitis rash important?
The location and distribution of the dermatitis are vital clues to the underlying culprit (Table 9-2). For example, an eczematous dermatitis on the dorsal feet should alert the clinician to the possibility of shoe dermatitis.
6. List three common misperceptions regarding the location of a contact dermatitis.
1. Dermatitis has to be bilateral if the exposure is bilateral, that is, with a shoe or glove allergy. In most cases, contact reactions tend to be patchy and do not have the same intensity at all sites of exposure.
2. The rash of contact dermatitis occurs only at the site of maximal contact. Allergens can frequently be spread to distant sites of contact (Fig. 9-3), as when nail polish is transferred to the eyelid, inducing dermatitis when a sensitized patient rubs her eyelids with her fingernails.
3. Contact dermatitis does not affect the palms and soles because of their thick stratum corneum. Although it is true that other more sensitive areas such as the eyelids, face, and genitalia are more likely to be reactive, contact dermatitis definitely should be considered when dealing with an eczematous dermatitis of the palms or soles.
7. How is patch testing done?
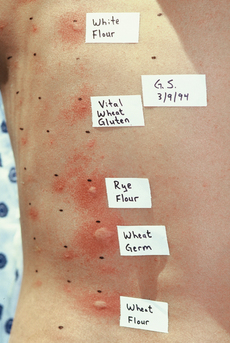
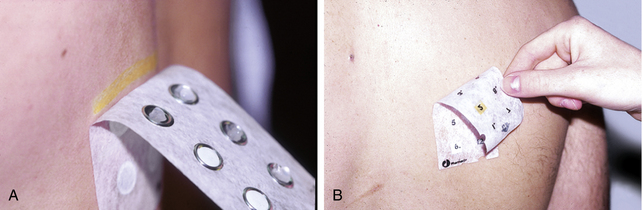
Because ICD and ACD can be indistinguishable both clinically and histologically, patch testing is the only method available to diagnose ACD and differentiate it from ICD. Two patch test methods are currently in widespread use: the Finn chamber (Fig. 9-4A) and True Test systems (Fig. 9-4B). With the Finn chamber method, a small amount of the allergen, usually in a petrolatum vehicle, is placed into individual aluminum wells affixed to a strip of paper tape. With the True Test method, no advance preparation is necessary, as the allergens have already been commercially incorporated into the back of the paper tape strips. Only 28 “screening” allergens are currently available with the True Test, while hundreds are available with the Finn chamber method. These strips are applied to the patient’s upper back, which is the preferred testing site. After 48 hours, the patches are removed and the initial reading is recorded. Because these allergic reactions are delayed, a second interpretation must be performed at 72 hours, 96 hours, or even at 1 week after the initial test application. Additional readings beyond 48 hours increase the positive patch test yield by 34%. The classic positive allergic patch test reaction shows spreading erythema, edema, and closely set vesicles that persist after removal of the patch or that appear after 2 to 7 days. Irritant reactions may have a glazed, scalded, follicular, or pustular appearance that usually fades after the patch is removed.
Table 9-2. Location of Contact Dermatitis and Suspicious Agents
| LOCATION | SUSPICIOUS AGENT |
|---|---|
| Eyelids | Nail polish, eye makeup, airborne allergens |
| Earlobes or neck | Metal jewelry |
| Forehead, scalp margins | Hair dyes |
| Face | Cosmetic fragrances and preservatives, airborne allergens |
| Axilla | Deodorants |
| Hands | Gloves, occupational contacts |
| Waistband | Elastic |
| Dorsal feet | Shoes |

8. What substances are tested in the standard “screening” patch test?
Because of its convenience, most patients with a suspected allergic contact dermatitis are patch tested with the True Test “standard” panel of 28 allergens, which can detect many common sensitivities (Table 9-3). However, this panel only detects 62% to 75% of the most common allergens. The North American Contact Dermatitis Group’s Standard 65-allergen tray, which utilizes the Finn Chamber method, is a more efficacious screening series than more limited patch test series. Additional testing with more specialized allergen panels is frequently warranted to enhance allergen detection. Testing should only be done with known materials in accepted concentrations.
Table 9-3. Allergens Evaluated by the True Test and the Finn Chamber Test
| ALLERGEN | SOURCES |
|---|---|
| Benzocaine 5% | Topical anesthetic |
| Caine mix | Topical anesthetic |
| Nickel sulfate 2.5% | Metal jewelry |
| Potassium dichromate 0.25% | Leather, cement |
| Cobalt | Metal jewelry, paint |
| Neomycin sulfate 20% | Topical antibiotics |
| p-Phenylenediamine 1% | Hair dye |
| Ethylenediamine 1% | Topical medications |
| Cinnamaldehyde 1% | Perfume, flavors |
| Balsam of Peru 25% | Perfume, medications |
| Fragrance mix | Perfume, flavors |
| Formaldehyde 1% | Preservative, fabric finishes |
| Quaternium-15 2% | Cosmetic and industrial preservative |
| Imidazolidinyl urea 2% | Cosmetic preservative |
| Paraben mix | Cosmetic preservative |
| Thimerosal | Cosmetic and medicament preservative |
| Cl+Me− Isothiazoline (MCI/MI) | Cosmetic and industrial preservative |
| Lanolin alcohol 30% | Topical skin care products |
| Epoxy resin 1% | Glues, plastics |
| p-tert-butylphenol formaldehyde resin 1% | Glues |
| Colophony (resin) 2% | Adhesives, solder flux |
| Mercaptobenzothiazole 1% | Rubber, fungicide |
| Carba mix 3% | Rubber, fungicide |
| Thiuram mix 1% | Rubber, fungicide |
| Mercapto mix 1% | Rubber, fungicide |
| Black rubber mix 0.6% | Black rubber |
| Budesonide | Topical corticosteroid |
| Tixocortol 21-pivalate | Topical corticosteroid |
9. An astute physician should not need to patch test. Right?
Many clinicians believe that a thorough history and physical exam are sufficient for an accurate diagnosis of ACD. They believe that patch testing is unnecessary because they can tell whether a reaction is ICD or ACD simply by evaluating the dermatitis. Results of several studies, however, show that clinicians are often wrong when guessing whether contact dermatitis is irritant or allergic. In fact, experienced dermatologists may only suspect the true allergen in 50% of cases. Patch testing is the only way to differentiate between the two conditions because clinically and histologically ICD and ACD cannot be reliably differentiated.
10. What is a repeated open application test (ROAT)?
The ROAT, or usage test, is used when patch testing is negative, and yet there remains a strong clinical suspicion for ACD. Remember, patch testing is a one-time occlusive test that does not always duplicate low-level chronic daily exposure. With the ROAT, patients apply the suspected product to a quarter-sized area on the forearm twice a day for 1 week. If the patient is allergic, a localized dermatitis will occur, confirming the suspected allergy (Fig. 9-5).
11. What is the differential diagnosis of contact dermatitis?
Contact dermatitis, with its scaling, erythema, lichenification, and/or vesicles, belongs in the group of eczematous disorders. Other such conditions—atopic dermatitis, nummular eczema, neurodermatitis, stasis dermatitis, seborrheic dermatitis, photodermatoses, dermatophyte infections, drug eruptions, and dyshidrotic eczema (pompholyx)—should always be considered when evaluating a prospective patient for contact dermatitis. A complete history including previous skin diseases, drug and exposure histories, location and course of the eruption, patch testing, and potassium hydroxide tests should help point to the diagnosis of contact dermatitis.

12. Which is the most common allergen on the standard tray?
The metal nickel, found commonly in costume jewelry, is the most common allergen on the standard tray. Approximately 5.8% of the general population in the United States is sensitized, while patch test clinics around the country note a prevalence rate of 19% in their dermatitis populations (Fig. 9-6). The high rate of sensitization is felt to be secondary to ear piercing, which is why this allergy is more common in females. In men, nickel dermatitis is predominantly of occupational origin.

14. If a change in a skin care product does not lead to clearing of a patient’s rash, does this mean that the original product was not the culprit?
Not necessarily. Many consumer cosmetic and toiletry products contain the same allergens (usually fragrances and preservatives). Moreover, many products contain cross-reacting agents that can exacerbate the original problem. For example, patients who are allergic to the hair dye allergen paraphenylenediamine will need to avoid the over-the-counter topical anesthetic benzocaine. Both compounds belong to the para-amino group and can cross-react with one another.
15. How is contact dermatitis managed?
If the patient has ACD, the allergen should be detected by patch testing, and subsequently it should be thoroughly avoided. Sources of the allergen as well as cross-reacting agents should be explained to the patient. An acceptable nonsensitizing substitute should be offered. For ICD, avoidance of as many irritants as possible is crucial. Frequent water exposure, which desiccates and chaps the skin, should be kept to a minimum. Frequent moisturization and hand protection with gloves, if indicated, are important. With contact dermatitis, systemic steroids should be used only in acute situations. Compresses may be helpful if vesicles are present. When the condition is chronic, topical steroids of appropriate strength and moisturizers are the mainstay of therapy. Recently, the newer nonsteroidal macrolide immunosuppressive agents, tacrolimus and pimecrolimus, have been used increasingly with good results. Lastly, phototherapy and Grenz ray therapy has also been used in difficult cases.
Rietschel RL, Fowler JF: Treatment of contact dermatitis. In Rietschel RL, Fowler JF, editors: Fisher’s contact dermatitis, ed 6, Hamilton, Ontario, BC Decker, 2008, pp 722–729.