7 Conotruncal Lesions
Tetralogy of Fallot
Background
Overview of Echocardiographic Approach
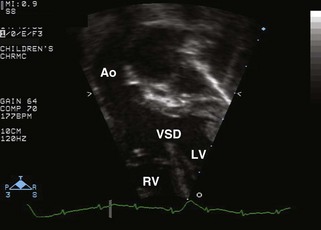
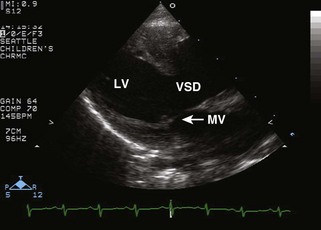
Anatomic Imaging
Acquisition


Physiologic Data
Alternate Approaches
Key Points
TOF Repaired
Background
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition
Analysis
Physiologic Data
Acquisition
Alternate Approaches
Key Points
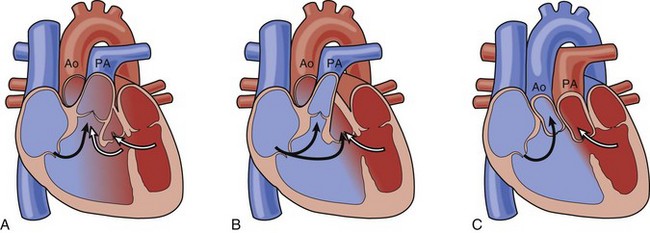
Double-Outlet Right Ventricle
Background
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition
Analysis
Pitfalls
Physiologic Data
Alternate Approaches
Key Points
Double-Outlet Right Ventricle: Post-Repair
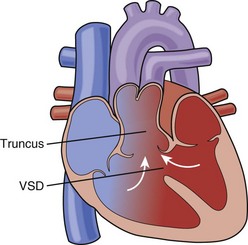
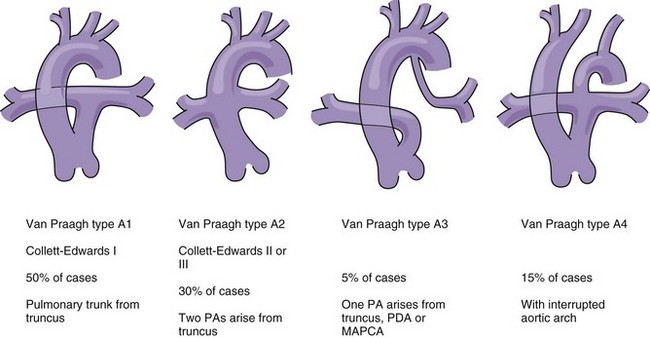
Truncus Arteriosus
Background
Anatomy
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition

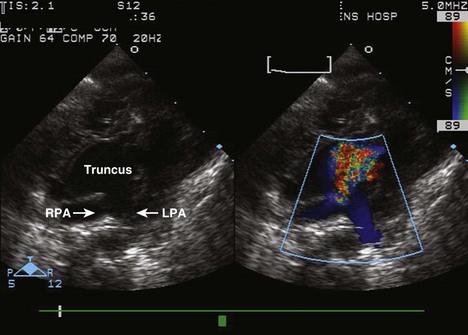
Pitfalls
Physiologic Data
Key Points
Truncus Arteriosus: Status Post Repair
Background
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition
Analysis
Physiologic Data
Acquisition
Alternate Approaches
Key Points
1 Anderson RH, Weinberg PM. The clinical anatomy of tetralogy of Fallot. Cardiol Young. 2005;15(Suppl 1):38-47.
2 Hagler DJ. Double-outlet right and left ventricles. In: Eidem BW, Cetta F, O’Leary PW, editors. Echocardiography in Pediatric and Adult Congenital Heart Disease. Philadelphia: Lippincott Williams & Wilkins, 2010.
3 Jones FD, Fenstermaker B, Kovalchin JP. Truncus arteriosus. In: Eidem BW, Cetta F, O’Leary PW, editors. Echocardiography in Pediatric and Adult Congenital Heart Disease. Philadelphia: Lippincott Williams & Wilkins, 2010.
4 Lewin MB, Salerno JC. Truncus arteriosus. In: Lai WW, Mertens LL, Cohen MS, Geva T, editors. Echocardiography in Pediatric and Congenital Heart Disease. Hoboken, NJ: Wiley-Blackwell, 2009.
5 Lopez L. Double-outlet ventricle. In: Lai WW, Mertens LL, Cohen MS, Geva T, editors. Echocardiography in Pediatric and Congenital Heart Disease. Hoboken, NJ: Wiley-Blackwell, 2009.
6 Miller-Hance WC, Silverman NH. Transesophageal echocardiography in congenital heart disease with focus on the adult. Cardiol Clin. 2000;18(4):861-892.
7 Srivastava S, Parness IA. Tetralogy of Fallot. In: Lai WW, Mertens LL, Cohen MS, Geva T, editors. Echocardiography in Pediatric and Congenital Heart Disease. Hoboken, NJ: Wiley-Blackwell, 2009.
8 Mahle WT, Martinez R, Silverman N, Cohen MS, Anderson RH. Anatomy, echocardiography, and surgical approach to double outlet right ventricle. Cardiol Young. 2008;18(Suppl 3):39-51.
9 Vyas H, Eidem BW. Tetralogy of Fallot. In: Eidem BW, Cetta F, O’Leary PW, editors. Echocardiography in Pediatric and Adult Congenital Heart Disease. Lippincott Williams & Wilkins, 2010.