[level-membership-for-obstetrics-gynecology-category]
Pelvic Congestion Syndrome
Synonyms/Description
Varicose veins of the pelvis
Etiology
Although the etiology of pelvic congestion syndrome is unclear, it appears that gross dilatation, valve incompetence, and reflux of the ovarian veins may be causal. Anatomic and/or hormonal factors may lead to insufficiency of the ovarian and/or internal iliac veins, resulting in peri-ovarian pelvic varicosities. Such tubo-ovarian varicoceles may be the female equivalent of testicular varicoceles.
Ultrasound Findings
The ultrasound diagnosis is based on a subjective impression of excessive venous channels in a patient with dull and chronic pelvic pain made worse when standing. CT scans have also been used to detect these varicosities, but an ultrasound diagnosis is usually sufficient. The objective criteria include dilated ovarian veins greater than 4 mm in diameter, dilated and tortuous arcuate veins communicating with pelvic varicose veins, and retrograde venous flow, particularly in the left ovarian vein.
Differential Diagnosis
The diagnosis of pelvic venous congestion is suggested after all other causes of pelvic pain have been excluded. Endometriosis is a common cause of chronic pelvic pain that should be investigated before implicating venous congestion as a final diagnosis. Furthermore, there are patients with large pelvic veins who have no pain at all and others who barely make the subjective criteria for this disorder but who complain of debilitating pain. Certainly once a patient has been investigated for other causes of pelvic pain, large, dilated, tortuous pelvic varicosities with sluggish and occasional retrograde flow do suggest the diagnosis of pelvic venous congestion syndrome.
Clinical Aspects and Recommendations
Clinically, pelvic congestion syndrome is characterized by pelvic pain of at least 6 months duration. It often manifests during or after a pregnancy and worsens with subsequent pregnancies. Such pain can be variable in its severity, but it is usually described as a dull ache or heaviness. It increases premenstrually and is worsened with prolonged standing, postural changes, walking, or activities that can increase intra-abdominal pressure. Occasionally it is worsened after intercourse. Classically it is unilateral and greater on the left side in most patients. It is virtually unheard of in menopausal women, thus implicating the hormone estrogen in part of the pathogenesis.
There is no standard approach to treatment of pelvic congestion syndrome. Ovarian cycle suppression with combination contraceptives, GnRH agonists, or high-dose progestational agents has been employed. In the most severe cases refractory to medical management, embolization of ovarian veins can be performed. Rarely, hysterectomy and bilateral salpingo-oophorectomy can be viewed as a last resort.
Figure
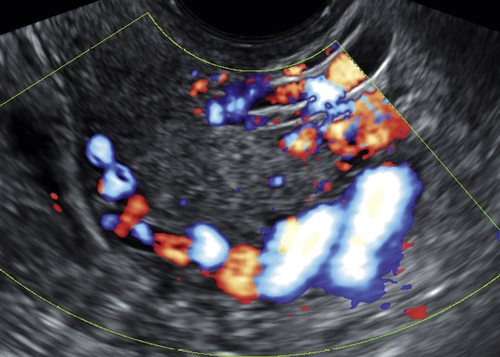
Figure P2-1 Color flow Doppler image showing excessive and large veins around the uterus in a patient with characteristic dull but chronic pelvic pain.
Suggested Reading
Beard R.W., Reginald P.W., Wadsworth J. Clinical features of women with chronic lower abdominal pain and pelvic congestion. Br J Obstet Gynecol. 1988;95:153.
Hobbs J.T. The pelvic congestion syndrome. Br J Hosp Med. 1990;43:200.
Ignacio E.A., Dua R., Sarin S., Harper A.S., Yim D., Mathur V., Venbrux A.C. Pelvic congestion syndrome: diagnosis and treatment. Semin Intervent Radiol. 2008;25:361–368.
Tu F.F., Hahn D., Steege J.F. Pelvic congestion syndrome-associated pelvic pain: a systematic review of diagnosis and management. Obstet Gynecol Surv. 2010;65:332–340.
[/level-membership-for-obstetrics-gynecology-category][not-level-membership-for-obstetrics-gynecology-category]
Pelvic Congestion Syndrome
Synonyms/Description
Varicose veins of the pelvis
Etiology
Although the etiology of pelvic congestion syndrome is unclear, it appears that gross dilatation, valve incompetence, and reflux of the ovarian veins may be causal. Anatomic and/or hormonal factors may lead to insufficiency of the ovarian and/or internal iliac veins, resulting in peri-ovarian pelvic varicosities. Such tubo-ovarian varicoceles may be the female equivalent of testicular varicoceles.
Ultrasound Findings
The ultrasound diagnosis is based on a subjective impression of excessive venous channels in a patient with dull and chronic pelvic pain made worse when standing. CT scans have also been used to detect these varicosities, but an ultrasound diagnosis is usually sufficient. The objective criteria include dilated ovarian veins greater than 4 mm in diameter, dilated and tortuous arcuate veins communicating with pelvic varicose veins, and retrograde venous flow, particularly in the left ovarian vein.
Differential Diagnosis
Buy Membership for Obstetrics & Gynecology Category to continue reading.
Learn more here
[/not-level-membership-for-obstetrics-gynecology-category]
Gynecologic Ultrasound A Problem-Based Approach Expert Consult