Can you imagine a world without conflict? Why, it would be a world without change! Conflict is inevitable wherever there are people with differing backgrounds, needs, values, and priorities.
A stereotypical perspective of conflict related to nursing is that “nice” nurses avoid conflict. According to Beauregard and colleagues (2003), although caricatured images of the nurse may encompass the “old” battle-ax, the control freak, the naughty nurse, or the doctor’s handmaiden, the primary perception of the nurse by the public is one of the caring angel who is gentle and kind. Conflict within the nursing profession has traditionally generated negative feelings to the extent that many nurses use avoidance as a coping mechanism because of their feeling that the “public’s stereotypical image of them demanded that they be ‘nice,’ self-sacrificing, and submissive nurses and that if they engaged in conflict they would be branded emotional or unfeminine women” (Kelly, 2006, p. 27).
The presence of conflict in a situation is not necessarily negative but may, in fact, have some positive results. As a process, conflict is neutral. Following are some possible outcomes of conflict:
Disturbing issues are brought out into the open, which may avert a more serious conflict.
Group cohesiveness may increase as individuals resolve issues.
New leadership may develop as a consequence of resolution.
The results of conflict can be constructive, occurring when productive outcomes are achieved, or destructive, leading to poor communication and creating dissatisfaction.
Conflict
What Causes Conflict?
Let us look at some common factors of conflict as they relate to nursing.
Role Conflict
When two people have the same or related responsibilities with ambiguous boundaries, the potential for conflict exists. For example, a nurse on the 11 PM to 7 AM shift may be uncertain whether he or the nurse on the 7 AM to 3 PM shift is responsible for weighing a patient.
Communication Conflict
Failing to discuss differences with one another can lead to problems with communication. Communication is a two-way process; when one person is unclear in a communication, the process falls apart. A recent graduate may find that with a busy schedule, numerous patient demands, and a shortage of time, it is easy to forget to notify a patient’s family of a change in visiting hours—a great annoyance to the family members who cannot visit when they arrive.
Goal Conflict
We all have unique goals and objectives for what we hope to achieve in our places of employment. When one nurse places his or her personal achievement and advancement above everyone else’s, conflict can occur. An example of this can be seen in the newly graduated nurse who pursues an advanced nursing degree immediately following undergraduate education; the experienced nurse in the unit may feel that the new graduate nurse requires a minimum length of time at the bedside before advancing his or her education.
Personality Conflict
Wouldn’t it be great if we got along with everyone? Of course, we all know that there are just some people with whom we have a difficult time. The situation is all too familiar, and many times we may find ourselves with such thoughts as “I’ll try to overlook her negative, lousy behavior; after all, she doesn’t have much of a family life.” Trying to change another person’s personality is like guaranteeing an unhappy ending to a story.
Ethical or Values Conflict
During a cardiac arrest, a graduate nurse has a conflict with the physician’s order of “No Code,” on a young adolescent patient. She has difficulty taking care of the adolescent, because he reminds her of her younger brother who died tragically in an automobile accident.
Conflicts in nursing may fit into one or more of the aforementioned categories. Consider some common areas of conflict among nursing staff, including scheduling days off, determining vacation leave, assigning committees, patient care assignments, and performance appraisals, to name just a few.
What Are Common Areas of Conflict Between Nurses and Patients—and Between Nurses and Patients’ Families?
Guttenberg (1983) identifies five common areas of conflict among nurses and their patients and families.
1. Quality of care. This is by far the most common area of conflict and the easiest to remedy. Families typically are concerned with how well their loved one is being attended to, how friendly the nurses are, how well the hospital or home health services are provided and coordinated, and how flexible the hospital is with visiting hours and meeting their special needs.
2. Treatment decisions. This area of conflict often arises between the family of an older adult and the nurse. A physician may order a treatment with which the family does not agree. In this situation it is very important that the nurse not defend the physician’s orders or attempt to persuade or convince the family that the physician or nurse knows what’s best for the patient. In these situations, the issue is rarely the treatment itself but rather the family’s desire to decide what is right for the loved one. Be sure to clarify the orders and explain to the family that you are supposed to carry them out unless the family negotiates directly with the physician to change them. Conflict may also exist between the nurse and physician regarding care of older adults. For example, a physician may decline to perform a medical procedure on an older patient secondary to advanced age or preexisting comorbidities.
3. Family involvement. For example, when a young adult is diagnosed with cancer, numerous issues may arise concerning the presence of family members during procedures and the extent of their involvement in the overall care. Such issues are based on the family’s real need to feel significant and adequate in meeting the young adult’s needs.
4. Quality of parental care. This can become an issue when nurses are unhappy with how parents are participating in their child’s care. It is helpful to offer parenting classes that can encourage parents to meet other parents and can model positive parenting techniques. Fear of being a bad parent, by not responding to every cry an infant makes, is a good example of an area where the nurse can educate the parents on responding to their infant’s physical and emotional needs.
5. Staff inconsistency. This is another issue that is easily prevented. Make sure that staff members on each shift are consistent in enforcing hospital policies and that they notify other shifts of any attempts at manipulation by family members or patients.
Conflict Resolution
What Are Ways to Resolve Conflict?
Unresolved conflicts waste time and energy and reduce productivity and cooperation among the people with whom you work. In contrast, when conflicts are resolved, they strengthen relationships and improve the performance of everyone involved (Kim, Nicotera, & McNulty, 2015). The key to managing conflict successfully is tailoring your response to fit each conflict situation instead of just relying on one particular technique. Each technique represents a different way to achieve the outcome you want and to help the other person achieve at least part of the outcome that he or she wants. How do you know which technique to use? That depends on the following:
• How much power do you have in this situation compared with the other person?
• How much do you value your relationship with the person with whom you are in conflict?
• How much time is available to resolve the conflict?
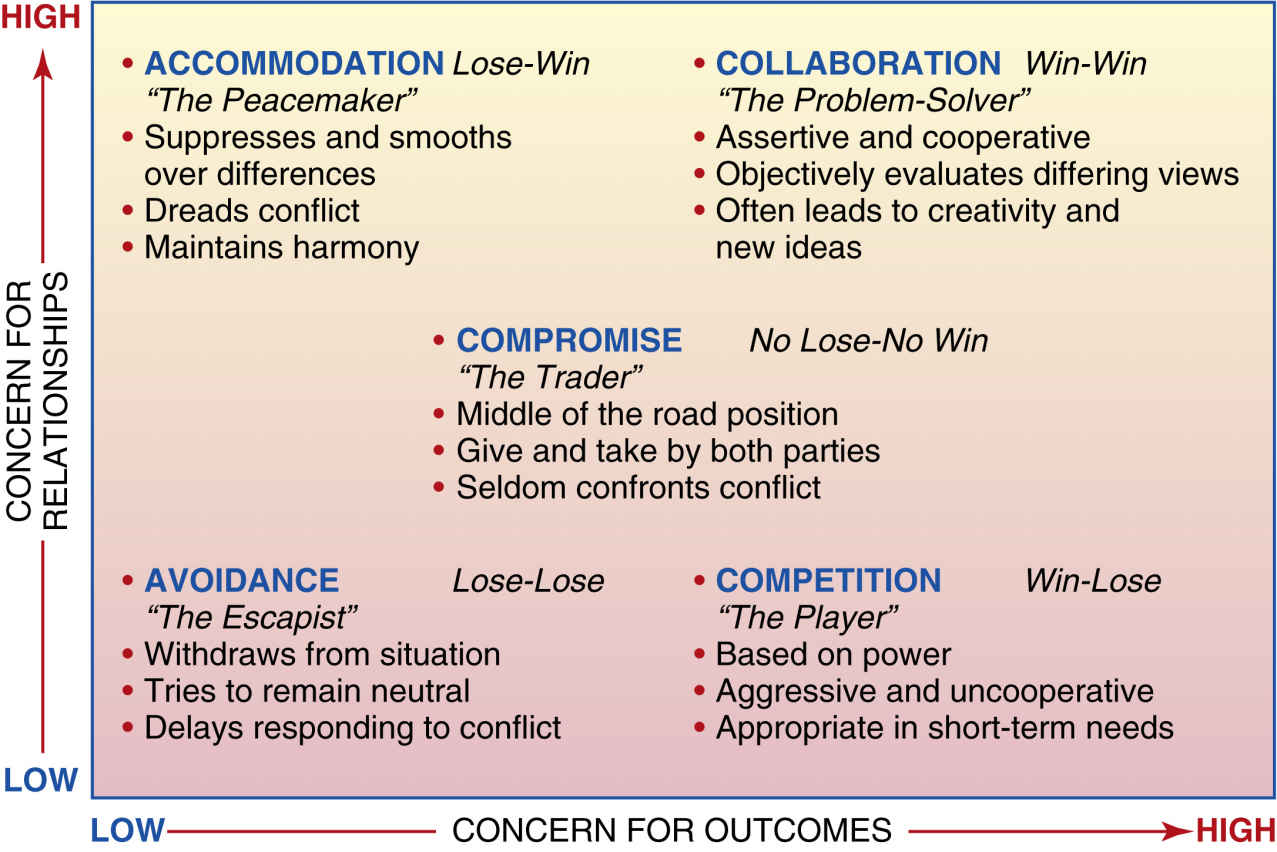
An example of a model for conflict resolution can be found in Fig. 13.1. This model incorporates several views of conflict resolution. Filley (1975) described three basic strategies for handling conflict, according to outcome: win-win, lose-lose, and win-lose. Various others have identified the following five responses to resolve conflict: competition, accommodation, avoidance, compromise, and cooperation. In a recent study, the prevalent style for conflict resolution used by nursing students was compromise, followed by avoidance (Hamilton, 2008). As noted in this research study, compromise attempts to meet the needs of individuals on both sides of a conflict, whereas collaboration, which may take more time, offers the best avenue or approach to settling the conflict that will satisfy both participants (win-win solution). A research study by Iglesias and Vallejo (2012) examined predominant conflict resolution styles used by a sample of Spanish nurses in two work settings, academic and clinical, in order to determine differences between these environments. Their findings indicated that conflict management styles varied according to work setting, with nurses in an academic environment using most frequently the compromising style and nurses in the clinical environment using the accommodating style most frequently.
Let us look at an example and apply the model.
Suppose the charge nurse on your unit has posted the vacation schedule for the month of December. You, as a recent graduate, have requested to be off during the week of Christmas. You notice on the schedule that none of the recent graduates has received the Christmas holidays off. You feel that this is unfair, because you will not have an opportunity to be with your family during the Christmas holidays. How can you resolve this conflict?
FIG. 13.1 Model for conflict resolution. (Modified from Douglas, E., & Bushardt, W. (1988). Interpersonal conflict: Strategies and guidelines for resolution, J Am Med Rec Assoc 56(18); Sullivan, E., & Decker, P. (1988). Effective management in nursing. Menlo Park, CA: Addison-Wesley.)
Competition
This is an example of the win-lose situation. In this situation, force—or the use of power—occurs. It sets up a type of competition between you and your charge nurse. Typically, competition is used to resolve conflict when one person has more power in a situation than the other. In the given situation, the charge nurse refuses your request for Christmas vacation, explaining that the staff members with more seniority have priority for vacation at Christmas time.
Avoidance
Avoidance is unassertive and uncooperative and leads to a lose-lose situation. In some situations, avoidance is not considered a true form of conflict resolution because the conflict is not resolved and neither party is satisfied. In the given situation, you would not have approached the charge nurse with the Christmas schedule issue. Usually, both persons involved feel frustrated and angry. There are some situations in which avoiding the issue might be appropriate, such as when tempers are flaring or when strong anger is present. However, this is only a short-term strategy; it is important to get back to the problem after emotions have cooled.
Accommodation
Accommodation is the lose-win situation, in which one person accommodates the other at his or her own expense but often ends up feeling resentful and angry. In the given situation, the charge nurse would put her own concern aside and let you have your way, possibly even working for you during the scheduled slot. The charge nurse loses and the graduate nurse wins in this situation, which may set up conflict among staff and other recent graduates. When is accommodation the best response? Is it when conflict would create serious disruption, such as arguing, or when the person with whom you are in conflict has the power to resolve the conflict unilaterally? In this response to conflict, differences are suppressed or played down while agreement is emphasized.
Compromise
Compromise or bargaining is the strategy that recognizes the importance of both the resolution of the problem and the relationship between the two people. Compromise is a moderately assertive and cooperative step in the right direction, in which one creates a modified win-lose outcome. In the given situation, the charge nurse compromises with you by allowing you to have Christmas Eve off with your family but not the entire week. The problem lies in the reduced staffing that will occur for a short period. The compromise may not be totally satisfactory for either party, but it may be offered as a temporary solution until more options become available.
Collaboration
Collaboration is the strategy that involves a high level of concern for the problem, the outcome, and the relationship. It deals with confrontation and problem solving. The needs, feelings, and desires of both parties are taken into consideration and re-examined while searching for proper ways to agree on goals. Collaboration is a win-win solution with a commitment to resolve the issues at the base of the conflict. It is fully assertive and cooperative. In the given situation, you and the charge nurse discuss the week of Christmas vacation and the staffing needs and agree that you will work the first three days of that week and the charge nurse will work the second half of that week. You also agree to be there the first part of the week to complete the audit on the charts from the previous week for the charge nurse. In this situation both persons are satisfied, and there is no compromising what is most important to each person. That is, the charge nurse gets her audit completed, and the recent graduate is able to spend half of the Christmas week with her family. What is your particular style for resolving conflict? (See Critical Thinking Box 13.1.)
CRITICAL THINKING BOX 13.1Conflict Questionnaire
Directions: Consider situations in which you find your wishes differing from those of another person. For each of the following statements, think how likely you are to respond to each situation in the manner described. Check the rating that best corresponds to your response.
From Thomas, K. W. (1977). Toward multidimensional values in teaching: The example of conflict behaviors, Academy of Management Review, 2, 487.
What Are Some Basic Guidelines for Choosing the Technique to Use?
In some situations, certain techniques and responses work best. You may have to use accommodation or avoidance when you lack the power to change the situation. When you have conflict in a relationship that you value, it might be more helpful to use accommodation, compromise, or collaboration. When there is no immediate, pressing sense of urgency to solve an issue, then any of the five techniques can be used. However, when you are facing an emergency situation or a rapidly approaching deadline, your best bet is to use competition or accommodation. Just remember the following key behaviors in managing conflict:
▪ Deal with issues, not personalities.
▪ Take responsibility for yourself and your participation.
▪ Communicate openly.
▪ Avoid placing blame.
▪ Listen actively.
▪ Sort out the issues.
▪ Identify key themes in the discussion.
▪ Stay focused in the present; don’t dwell on the past.
▪ Weigh the consequences.
▪ Identify resolution options.
▪ Develop an outcome and obtain consensus.
Suppose that you follow all of these suggestions and you still are confronted with that difficult situation or that difficult person. Read on.
Dealing with Difficult People
What Are Some Techniques for Handling Difficult People?
Now that we have discussed types of conflict-management techniques, we are ready to look at techniques for handling difficult people. How do you deal with an abusive physician or supervisor? How do you react when someone constantly complains and gripes about something? How do you handle the know-it-all who will not even listen to your thoughts about an issue? (See Research for Best Practice Box 13.1 for suggestions on managing difficult employees.)
I am sure, if you have not already, you will run into in the near future a Sherman tank (Fig. 13.2). According to Bramson (1981), Sherman tanks are the attackers. They come out charging and are often abusive, abrupt, and intimidating. But more important, they tend to be downright overwhelming.
Remember Dr. Smith, who flew into a tirade because you forgot to have a suture removal set at his patient’s bedside at 8 AM sharp? Remember how you felt? “My heart was beating so loud I could hear it, and I was sure everyone else around could hear it, too. I was so furious at him for the comments he made.”
In understanding Sherman tanks, it is important to realize that they have a strong need to prove to themselves and to others that their view of the situation is right. They have a very strong sense of what others ought to do but often lack the caring and the trust that would be helpful in getting something done. They usually achieve what they want, but to do so causes them a lot of disagreements, lost friendships, and uncomfortable relationships with their co-workers. Sherman tanks are often very confident and tend to devalue those whom they feel are not confident. Unfortunately, they demean others in a way that makes them look very self-important and superior. How do you cope with a Sherman tank? The most important thing is to keep your fear and anger under control and to avoid an outright confrontation about who is right and who is wrong. The following are some specific things you should do:
RESEARCH FOR BEST PRACTICE BOX 13.1Managing Difficult Employees
Practice Issue
Nurse managers are often faced with a difficult employee. The difficult employee’s negative conflict behavior affects team performance effectiveness, job satisfaction, and turnover intention. According to Pareto’s 80/20 rule, 20% of employees/workers will cause 80% of the problems, which means that a small number of issues are responsible for a large percentage of the effect.
In an environment of team collegiality, there is less negative conflict, increased commitment to the organization, and greater satisfaction, autonomy, and control over practice. In professional practice environments, nurses experience constructive conflict approaches, and effectiveness is enhanced in the workplace.
It is part of the nurse manager role to create an environment that facilitates professional practice. This type of environment requires that employees are socialized to their nursing role. In these professional practice environments, the unique preferences, perspectives, opinions, concerns, and choices of the individuals are recognized and valued. During nursing school, professional role socialization (“think like a nurse”) is initiated and later solidified during the early years of practice when the new graduate incorporates knowledge, skills, attitude, and affective behavior associated with carrying out the expectations of the nursing role.
Additionally, nurse managers may encounter conflict among employees in which the nurse manager needs to serve as a mediator among the employees involved in an argument or disagreement. The role of a mediator is to assist disputants in coming to a resolution or agreement. The mediator assists the parties involved by “defining problems, enumerating priorities, exploring alternatives, and facilitating resultant negotiations” (Cheng, 2015, p. 311).
Implications for Nursing Practice
Effective role socialization occurs when the nurse engages in actions that benefit other nurses and/or patients and families by helping, supporting, and encouraging mutual goal accomplishment and/or well-being.
• There needs to be positive interdependence among the nursing staff.
• Nurses need to understand and use constructive conflict-management skills.
• Employ mediation techniques when disputes arise between employees and/or patients and their families.
• There needs to be high trust among the nursing staff.
• Prosocial behavior should be noted among staff with the feeling of “sink or swim together” versus “you sink and I swim.”
• Do not procrastinate in dealing with difficult employees, patients, or their families.
• A high basic self-esteem is noted among nursing staff in an empowering, healthy workplace environment.
• The conflict negotiation strategy used may be collaboration (win-win) or mediation.
Considering This Information
How might you use some of the strategies listed in this chapter to handle a difficult employee? What types of activities are you involved in as a student that promote a positive professional practice environment? What essential skills would be important for a nurse to possess to serve as a mediator?
FIG. 13.2 Sherman tank.
• Do not allow yourself to be run over; step aside.
▪ Stand up for yourself. Defend yourself, but without fighting. Seek support when warranted.
▪ Give them a little time to run down and express what they might be ranting about.
Sometimes, it is necessary to be rude; get your word in any way that you can.
▪ If possible, try to get them to sit down. Be sure to maintain eye contact with them while you are assertively stating your opinions and perceptions very forcefully.
▪ Do not argue with them or try to cut them down.
• When they finally hear you, be ready to be friendly.
Next to the Sherman tanks are the snipers (Fig. 13.3). The snipers are the pot-shot artists. They are not as openly aggressive as the Sherman tanks. Their weapons are their innuendoes, their digs, and their nonplayful teasing, which is definitely aimed to hurt you. Snipers tend to choose a hidden rather than a frontal attack. They prefer to undercut you and make you look ridiculous. So, when you are dealing with snipers, remember to expose the attack, that is, “smoke them out.” Ask them very calmly:
“That sounded like a put-down. Did you really mean it that way?” Or you might say, “Do I understand that you don’t like what I’m saying? It sounds as if you are making fun of me. Are you?”
When a sniper is giving you criticism, be sure to obtain group confirmation or denial. Ask questions or make statements such as, “Does anyone else see the issue this way?” “It seems as though we have a difference of opinion,” or “Exactly what is the issue here? What is it that you don’t like about what occurred?” One way to prevent sniping is by setting up regular problem-solving meetings with that person.
FIG. 13.3 The sniper.
Also difficult to cope with are the constant complainers. These people often feel as though they are powerless, so they draw attention—but seldom action—to their problem. A complainer points out real problems but does it from a very unconstructive stance. Coping with a complainer can be a challenge. First, it is important to listen to the complaints, acknowledge them, and make sure you understand what the person said by paraphrasing it or checking out your perception of how the person feels. Do not necessarily agree with the person; with a complainer, it is important to move into a problem-solving mode by asking very specific, informative questions and encouraging him or her to submit complaints in writing. For example, try communicating with the constant complainer in the following manner:
“Did I understand you to say that you are having difficulty with your patient assignment?”
“Would it be helpful if I went to the pharmacy for you, so that you could complete your chart on your preoperative patient?”
Next are the maddening ones: the clams (Fig. 13.4). The clams have an entirely different tactic from the previous three. They just refuse to respond when you need an answer or want to have a discussion. It might be helpful to try to read a clam’s nonverbal communication. Watch for wrinkled brows, a frown, or a sigh. How to deal with clams? Try to get them to open up by using open-ended questions and waiting very quietly for a response. Do not fill in their silence with your own conversation. Give yourself enough time to wait with composure. Sometimes a little “clamming” on your own part might be helpful by using the technique called the “friendly, silent stare,” or FSS. The way to set up the FSS is to have a very inquisitive, expectant expression on your face with raised eyebrows, wide eyes, and maybe a slight smile—all nonverbal cues to the clam that you are waiting for a response. When clams finally open up, be very attentive. Watch your own impulses—do not bubble over with happiness just because they have finally given you two moments of their time. Avoid the polite ending; in other words, get up and say, for example:
FIG. 13.4 The clam.
“This was important to me. I’m not going to let this issue drop. I’ll be back to talk to you tomorrow at 2 o’clock.” Do not be the nice guy and say, “Thanks for coming in. Have a nice weekend. I’ll see you tomorrow.”
Be very direct and inform the clam what you are going to do, especially if the desired discussion did not occur.
What Is Anger?
Anger is something that we feel. Usually when we become angry, we assume it is because we are upset about what someone has done to us. Often we want to pay them back or take out our rage on them. Usually when anger occurs, it is difficult to see beyond the moment, because most people are consumed with thoughts of revenge or the wrongdoing that has occurred to them. Weiss and Cain (1991) state that “Anger is often a cover-up emotion … that disguises what is really going on inside you.” But anger is a signal, and according to Lerner (1997), it is “one worth listening to” (p. 1). She goes on further to say that:
Our anger may be a message that we are being hurt, that our rights are being violated, that our needs or wants are not being adequately met, or simply that something is not right. Our anger may tell us that we are not addressing an important emotional issue in our lives, or that too much of ourselves—our beliefs, values, desires, or ambitions—are being compromised in a relationship. Our anger may be a signal that we are doing more and giving more than we can comfortably do or give. Or our anger may warn us that others are doing too much for us, at the expense of our own competence and growth. Just as physical pain tells us to take our hand off the hot stove, the pain of our anger preserves the very integrity of our self. Our anger can motivate us to say “no” to the ways in which we are defined by others and “yes” to the dictates of our inner self. (p. 1)
No matter what, when feelings of frustration, disappointment, or powerlessness take over, there is no doubt that anger is in the making. Anger seems to begin in situations fraught with threats and anxiety.
Anger has two faces. One is guilt, which is anger aimed inward at what we did or did not do, and the other is resentment, which is anger directed toward others at what they did or did not do.
The following is true about both guilt and resentment: They both accumulate over time and lead to a cycle of negative energy that poisons our relationships and stifles our personal growth.
There is another side of the coin, however. If feeling angry signifies a problem, then ventilating anger does not necessarily solve it. Actually, ventilating anger may serve to maintain it if change and successful resolution do not occur. Tavris (1984) suggests that we learn two things about handling anger: first, how to think about anger, and second, how to reduce the tension. More about this later in the chapter.
Box 13.1 shows a summary of different anger styles. Just think about anger from a cardiovascular point of view. Most authorities consider anger one of the most damaging and dangerous emotions, because your pulse and blood pressure become elevated, sometimes to dangerous heights.
What Is the Solution for Handling Anger?
Change the image of it!
Stop
Appraise the situation. Do not do a thing. You are at a pivotal point. You have two ways to go: One is to become angry; the other is to reevaluate the situation. Try to look at a way to reinterpret the annoying comment. Consider the following example:
“Who does that charge nurse think she is to treat me like I’m a dummy!” or “How could someone be so thoughtless as to not remember my birthday!” You can reinterpret these and say to yourself, “Maybe if she weren’t so unhappy, she wouldn’t have considered doing such a thing” or “Maybe that person’s having a rough day.” The important thing here is to empathize with the person and to try to find justifications for the behavior that was so annoying to you.
Look
What image about yourself or another is about to be or has been breached—what shoulds, musts, or need tos have been violated? In other words, what has just occurred that has led you to feel angry with yourself or with another?
After receiving the end-of-shift report and making patient rounds, a recent graduate goes into a patient’s room to take vital signs. Within moments the patient has a cardiac arrest. Two hours later, while completing her charting, the recent graduate states guiltily, “I should have taken those vital signs earlier. It just needs to be the first thing I do when I get on the unit. I should have been on top of this. I must do better.” Notice the self-criticism in the recent graduate’s comments. Guilt, like resentment, can be a habit. It demonstrates—too clearly—how we respond to a situation in a negative manner. To help you get in touch with these feelings, try eliminating the words “must” and “should” from your vocabulary for just an hour. It is quite surprising to find out how frequently we use these terms.
BOX 13.1Anger Characteristics and Triggers
What Is Your Anger Style?
Passive Characteristics
• Avoidance—no eye contact or avoiding communicating with others; “silent treatment or cold shoulder”
• Withdrawing emotionally
• Becoming ill or anxious
• Sitting on the fence and not making a decision
• Talking about frustrations but showing no feelings
• Doing little or nothing or putting things off to thwart other’s plans
• Not feeling anger when something is wrong
Aggressive Characteristics
• Acting out or lashing out at another person; out of control behavior
• Bullying
• Incivility—offensive, intimidating, or hostile action
• Explosive, sudden outburst and release of feelings
• Taking anger out on someone or something else (i.e., kicking the dog, breaking things)
• Violence—getting physical or hurting people
• Bringing up old grievances
Passive-Aggressive Characteristics
• Resenting and blaming others; opposition to the demands of others
• Hidden action to get back at someone; conscious revenge
• Procrastination and intentional mistakes in response to others’ demands; intentional inefficiency; “forgetting” to do things and using forgetfulness as an excuse
• Cynical, sullen, or hostile attitude
• Frequent complaints about feeling underappreciated or cheated; self-deprecating
What Are Red Flags and Long-Standing Issues That Trigger Anger?
• Experiencing feelings of being discounted, threatened, humiliated, rejected, insecurity
• Having to wait a long time for a person or an appointment
• Getting caught in traffic congestion or crowded buses, airplanes, or other similar frustrating situations
• Joking comments made about sensitive topics
• Friends borrowing items and not returning them or returning them in disrepair
• Friends borrowing money and not paying you back
• Being wrongly accused of some action or comment
• Having to clean up after someone who does not keep things as tidy as you expect
• Having a neighbor who plays loud music or is engaged in other behavior that is inconsiderate
• Being placed on hold for long periods of time while on the telephone
• Having your computer crash and losing valuable data
• Being given wrong directions when asking for assistance
• Having money or property stolen
• Being taken for granted by family and friends
Valentine, P. E. (2001). A gender perspective on conflict management strategies of nurses. Journal of Nursing Scholarship, 33 (1), 69–74.
Vivar, C. (2006). Putting conflict management into practice: A nursing case study. Journal of Nursing Management, 14, 201–206. doi: 10.1111/j.1365-2934.2006.00554.x
Change
How do you change the image? One of the ways is to use humor. Humor makes the anger (guilt and resentment) tolerable. Remember that it is difficult to laugh and frown at the same time. (It only takes 15 facial muscles to laugh, but twice that many to frown.) If reappraising the situation and using humor both fail as ways to manage your anger, some suggest venting the anger—for example, by getting mad, yelling, shouting, telling someone off, or breaking things. Although this might make us feel better momentarily, in the long run such outbursts make us feel worse.
Why does this method of venting anger, that is, letting it all hang out, make us feel worse? First, think of all the physiological changes that are occurring in your body: blood pressure, pulse, and respirations increase; the muscles contract; and adrenalin is released. Sound familiar? It is the “fight or flight” adrenal response. Can it be healthy to maintain a constant state of stress and readiness to respond? Another disadvantage of an uninhibited outburst of anger is that it may lead the other person to retaliate.
It might be important to recognize the difference between venting and acknowledging our anger. A typical expression of anger might be something such as the following:
“Hey, you turkey, what do you think you’re doing? Don’t you know how to put that catheter in? Are you stupid or something? Either you figure it out, or you get out of here. You hear me?”
This approach is insulting, demeaning, and accusatory. It is also likely to lead to some type of provoking response. In contrast, when we acknowledge our feelings, we make statements such as “I feel angry about …” or “I feel hurt about …” or “I feel guilty about .…” The use of “I” statements is our first step toward taking responsibility for ourselves by owning up to our own feelings instead of blaming others.
Venting anger simply does not work unless you want to intimidate those around you, coerce them into submission with a hot temper, or, even worse, look childish while ranting, raving, and beating the floor or each other with foam bats. So, what does work? Face it, embrace it, and erase it!
First, acknowledge the anger (face it): Ask “What am I feeling? Anger? Guilt? Rage? Resentment?”
Second, identify the provoking or triggering situation (embrace it): Ask “What caused this feeling? Whose problem is it?”
Third, determine what changes need to occur (erase it): Ask “What can I change? Can I accept what I cannot change?” Then take action and let go of the rest. Other ways to handle anger and remove yourself from the vicious cycle of guilt and resentment are in the following sections.
Move.
Get Active
Try exercise or anything involving physical activity, such as walking, aerobics, and running. Clean the garage or a kitchen drawer. If you are sitting, get up. If you are in bed, move your arms around. Just get active and do something!
Focus.
Refocus on Something Positive
Think of your cup as half full, not half empty. Look at the provoking situation: “My charge nurse won’t give me Christmas off. However, I am not scheduled to work either Christmas Eve or New Year’s Eve. So, by working Christmas Day, I’m assured the other days off.”
Breathe.
Pay Attention to Your Breathing
Slow it down. Take deep, slow breaths, feeling the air move through your nose and down into your lungs. Check out your body for areas of tenseness. Often anger can be felt as tightness in the chest and abdomen.
Conflict is an inevitable part of our day-to-day experience. How we negotiate and handle conflict and anger may not always be easy. You might be thinking right now “This looks good on paper, but in real life, it is not that easy to put into practice.” If you are feeling this way, take a risk and try changing your approach and viewpoint.
The important thing is learning about yourself.
How do you cope with conflict? How do you handle difficult people? How do you respond when angry?
Sexual Harassment in the Workplace
In today’s world, sexual harassment as a source of conflict has been taken seriously, as evidenced by the widespread visibility and increased recognition of the issue. The potential impact of harassment on nursing students both in the classroom and in the practice area is significant. According to Dowell (1992), nursing administrators and educators must be proactive in writing and implementing policies regarding sexual harassment. Valente and Bullough (2004) concur that employers should outline consequences and infractions of sexual harassment in their policies, as well as provide ongoing education about what constitutes sexual harassment and enforce a “no tolerance” policy (pp. 239–240). In a study by Libbus and Bowman (1994), 70% of female staff nurses surveyed reported sexual harassment by male patients and co-workers, with the most common complaint being sexual remarks and inappropriate touching. In addition, in a survey of nursing administrators, 68.8% of those who responded reported sexist attitudes among employees in their organizations, and 47.7% reported observing instances of sexual harassment (Blancett & Sullivan, 1993). These studies reflect the prevalence of sexual harassment in health care settings during the 1990s. With the introduction of sexual harassment awareness and training instituted by health care agencies, since this time, there have been few if any research studies reflecting the prevalence or sexual harassment in today’s health care workplace. Valente and Bullough (2004) have also noted that sexual harassment cases are often unreported by the victim. This might also explain why there is limited data on sexual harassment in the workplace setting.
The issue of sexual harassment came to the forefront during the 1991 confirmation hearings of Supreme Court Justice Clarence Thomas (Allen, 1992). A once-secretive problem is now openly discussed in newspapers and by the media. As awareness about sexual harassment increased, we all realized how little we knew about it and what we could do about it. The majority of cases involve women who report being harassed by men, but the reverse has also occurred. In nursing, the stereotypical situation of sexual harassment involves a nurse (i.e., a woman) and a doctor (i.e., a man) because of the large number of nurses who are women. However, with the increase in the number of men entering the nursing profession, there is the potential for men to experience sexual harassment in the workplace. Roth and Coleman (2008) agree that actual and perceived barriers exist that prevent men from entering the nursing profession. In an effort to remove existing barriers and attract more men into the nursing profession, the authors recommend that the image of men in nursing and the media’s depiction of male nurses should be showcased as positive and that increasing staff diversity by recruiting men within the nursing workforce should be embraced by both the public and nursing profession (Fig. 13.5).
FIG. 13.5 Sexual harassment.
What Is Sexual Harassment?
According to Friedman (1992), “sexual harassment refers to conduct, typically experienced as offensive in nature, in which unwanted sexual advances are made in the context of a relationship of unequal power or authority” (p. 9). He goes on to explain that victims of sexual harassment are subjected to sexually oriented verbal comments, unwanted touching, and requests for sexual favors. The typical problem, known as quid pro quo harassment, arises when unwelcome sexual advances have been made and an employee is required to submit to those demands as a condition either of employment or of promotion. “Hostile work environment” has been used as a legal claim to show that “the atmosphere in the work (or other) environment is so uncomfortable or offensive by virtue of sexual advances, sexual requests, or sexual innuendoes that it amounts to a hostile environment” (Friedman, 1992, p. 16). Hershcovis and Barling (2010) succinctly state, “Sexual harassment has been described in terms of its three subcomponents: gender harassment, unwanted sexual attention, and quid pro quo” (p. 875). Let us look at hypothetical examples of how sexual harassment can affect nursing.
Samantha, a recent graduate, was receiving continued requests from a male patient to provide him with a complete bed bath. However, when a male nurse was assigned to this patient the following day, the patient reported to the male nurse that he was capable of bathing himself and proceeded to take a shower.
Lisa, the evening charge nurse, was quite excited that Tom, a recent graduate, was going to work on her unit. Lisa pursued Tom by repeatedly asking him for assistance with patient care, and, when she called him into her office, she would touch him inappropriately.
What Can I Do About It?
There are two ways to handle this type of workplace conflict: informally and formally through a grievance procedure. Start with the most direct measure. Ask the person to STOP! Tell the harasser in clear terms that the behavior makes you uncomfortable and that you want it to stop immediately. Also, you might want to put your statement in writing to the person, keeping a copy for yourself. Tell other people, such as family, friends, personal physician, or minister, what is happening and how you are dealing with it. Friedman (1992) suggests keeping a written journal of harassing events, including all attempts used to try to stop the harassment. The need to exercise power and control, rather than sexual desire, is frequently the motive of the sexual harasser (perpetrator). If sexual harassment is occurring as a result of miscommunication and misinterpretation of actions and is primarily sexually driven, not power driven, then telling the perpetrator to stop will often clear up any misconceptions. However, if the perpetrator is power driven, the harassment will continue as long as he or she views the victim as passive, powerless, and frightened. What may be most difficult for the recent graduate is facing the fear that surrounds threats of job insecurity or public embarrassment (Friedman, 1992).
If a direct request to the perpetrator to stop does not work, then an informal complaint may be effective, especially if both parties realize a problem exists and want it to be solved. The goal of the informal method is to stop the harassment but not to punish the perpetrator. This method assists the person filing the complaint in maintaining some type of harmonious relationship with the perpetrator. According to Friedman (1992), “a formal grievance usually requires filing a written complaint with an official group such as a hearing” (p. 65). This is a legal procedure that is guided and regulated by federal and state laws specific to this type of grievance. Before a 1991 amendment to the Civil Rights Act (Title VII), the means of correcting this bad situation—making it right or compensating the victim for difficulty encountered—were quite restricted. What has occurred as a result of this act is that victims of intentional discrimination may now seek compensatory and punitive damages. Each state has an Equal Employment Opportunity Commission, which has as its specific charge the enforcement of Title VII.
Unfortunately, sexual harassment may be a form of conflict you are faced with in the workplace. It is important to learn to deal with your feelings and to be aware of actions to take in case this happens to you. When this type of situation is resolved in a constructive, positive manner, it allows you an opportunity to feel better about your ability to manage conflict.
Conclusion
Most of us have experienced conflict. Building effective conflict-management skills is key to working with patients, staff, and physicians. Various models exist to provide a framework for effective conflict resolution; the “win-win” model of collaboration is the strategy that aims for the highest level of resolution and is fully assertive and cooperative in approach. It requires creative nursing management and understanding to recognize and acknowledge that conflict will exist whenever human relationships are involved. This needs to be tempered with open, accurate communication and active listening by maintaining an objective, not emotional, stance as conflict resolution strategies are implemented. Review the Relevant Websites and Online Resources.





 Relevant Websites and Online Resources
Relevant Websites and Online Resources