Complications of Hysteroscopy
At any phase of operative hysteroscopy, a complication can occur. Obviously, it is best to avoid complications; however, if such an event happens, then recognition is mandatory. Because operative sheaths are large, cervical dilation is required to permit entry of the hysteroscope into the uterus. Perforation of the uterus may happen during dilation (Fig. 112–1). A diagnostic laparoscopic exam will allow the surgeon to determine whether to repair the injury. If bleeding continues after a reasonable clotting time, then the uterine wound should be sutured. Perforation may occur during intrauterine operations. If the injury results from the use of conventional tools (e.g., hysteroscopic scissors), then a laparoscopic view of the injury and surrounding viscera is acceptable (Fig. 112–2). If no continuing bleeding is observed, then no repair is required. If bleeding continues or is pulsatile in nature, then the wound must be hemostatically sutured (figure-of-8). When an energy device perforates the uterus (laser fiber or electrosurgical device), then laparotomy is necessary (Fig. 112–3). The surrounding intestine must be carefully and methodically inspected to determine whether a hole has been made in the small or large bowel (Fig. 112–4A, B). Similarly, the urinary tract and great vessels should be examined for injury.
A variety of complications result from the intravascular uptake of hysteroscopic media. These include fluid overload with resulting pulmonary edema. The latter can happen with any distending medium. Careful attention therefore is required to keep track of fluid deficits (the volume of injected fluid/the volume of returned fluid). The infusion of hypo-osmolar fluid can result in an even more serious complication, hyponatremia. Fluids such as glycine and sorbitol are hypotonic, whereas mannitol is iso-osmolar (Figs. 112–5 and 112–6).
A number of pumps have been employed to facilitate delivery of the distending medium to the uterus. Several of these pumps have utilized carbon dioxide (CO2) gas or air as the driving force to push fluid into the uterus. These pumps are dangerous and should be avoided because patients have been killed or injured when high-pressure gas inadvertently entered the vascular space (Figs. 112–7 and 112–8). Roller-type pumps are safe and effective.
A common complication with hysteroscopic surgery is bleeding from the operative site. This can be managed by placing a balloon within the uterus. The balloon is inflated carefully with up to 5 mL of sterile water to tamponade the bleeding vessels. If the uterine cavity is enlarged, a balloon of greater capacity may be placed with it (Fig. 112–9).
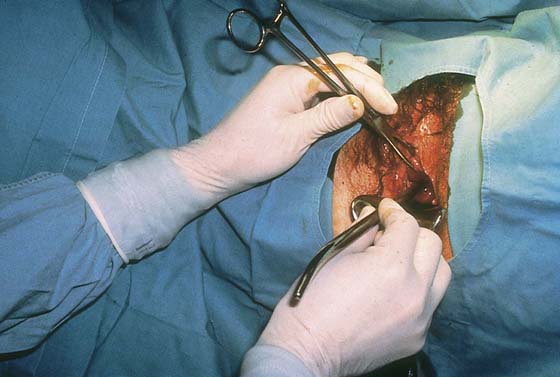
FIGURE 112–1 The cervix is undergoing dilation to allow passage of the operating sheath. Perforation of the uterus may occur; however, operative interventions and long-term adverse sequelae are uncommon.

FIGURE 112–2 Hysteroscopic scissors are seen via the laparoscope as it perforates the uterus. As with the dilator, unless persistent bleeding is observed, no treatment is required.

FIGURE 112–3 When a laser fiber or electrode perforates the uterus, a laparotomy is needed to determine whether adjacent structures have been injured.
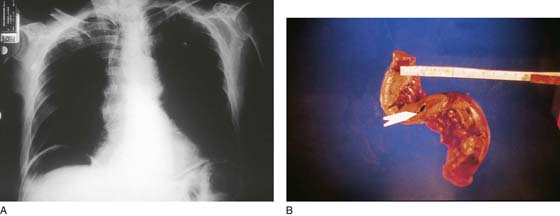
FIGURE 112–4 A. This abdominal upright film illustrates free air under the diaphragm after perforation of the uterus with an energy device. The radiograph was taken 3 days after hysteroscopic surgery associated with perforation. B. A piece of resected small intestine obtained after hysteroscopic perforation with a monopolar electrode. Note the extensive thermal injury to the bowel. The intestinal injury was responsible for leakage of contents and air into the abdominal cavity.
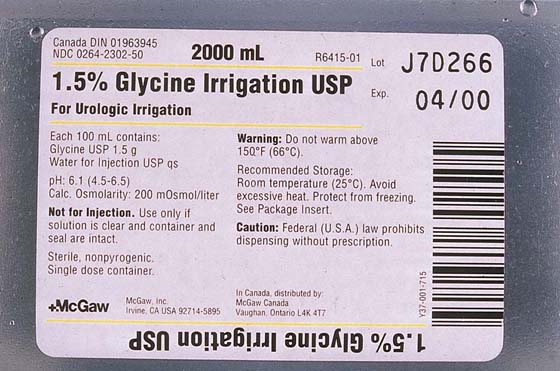
FIGURE 112–5 Glycine (1.5%) used for uterine distention has an osmolality of 200 mOsm/L. This hypotonic solution also is subsequently degraded to urea and ammonia.
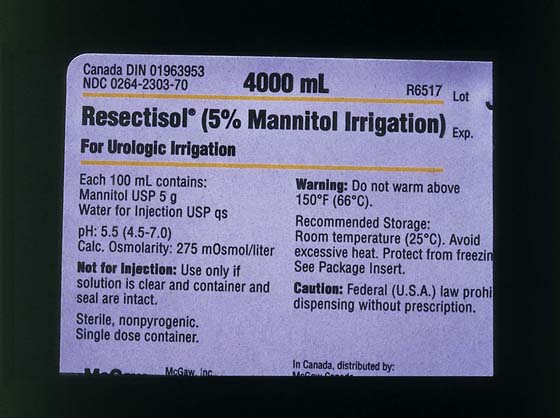
FIGURE 112–6 Mannitol (5%) is iso-osmolar at 275 mOsm/L. It is a significantly safer distention medium than glycine.

FIGURE 112–7 This Hyskon pump utilized carbon dioxide (CO2) gas to drive Hyskon into the uterus. When the Hyskon reservoir became exhausted and the ball valve failed, high-pressure CO2 gas was infused into the uterus.

FIGURE 112–8 This nitrogen-driven, low-viscosity, hysteroscopic-medium pump was withdrawn from the market. Air embolism can occur via valve failure after the liquid medium has emptied into the uterus.
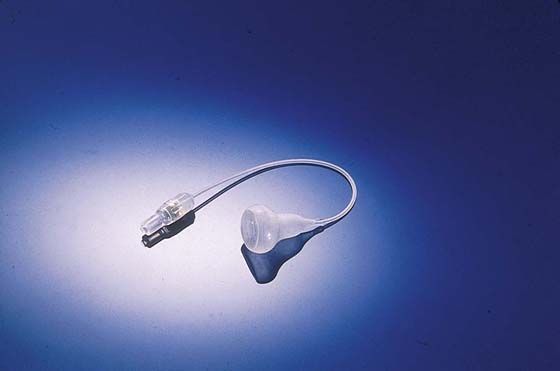
FIGURE 112–9 This specially designed balloon (Mentor) is placed into the uterus and filled with 2 to 5 mL of sterile water. Pressure from the balloon on the uterine wall tamponades the bleeding vessel(s).






