Chapter 74 Compartment Syndromes and Volkmann Contracture
Anatomy
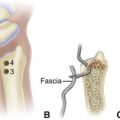
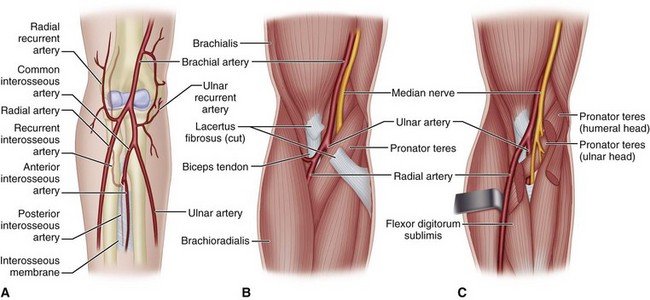
Four interconnected compartments of the forearm are recognized (Fig. 74-1): (1) the superficial volar compartment, (2) the deep volar compartment, (3) the dorsal compartment, (4) and the compartment containing the mobile wad of Henry (brachioradialis and extensor carpi radialis longus and brevis). The volar compartments are most commonly involved, but the dorsal and mobile wad compartments can be involved alone or in addition to the volar compartments. Clinically differentiating isolated or combined involvement of the deep and superficial volar compartments usually is difficult; however, the deep volar compartment (flexor digitorum profundus, flexor pollicis longus, and pronator quadratus) may be solely involved.

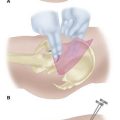
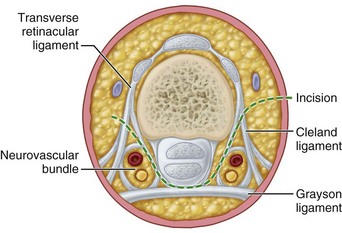
In the hand, each interosseous muscle is surrounded by a tough investing fascial layer, each making an individual compartment as shown by the injection dissections of Halpern and Mochizuki. The adductor pollicis muscle and the thenar and hypothenar muscles form three separate compartments (Fig. 74-2). The neurovascular bundles of each digit also are compartmentalized by fascial layers, making them vulnerable to excessive swelling (Fig. 74-3).

Etiology
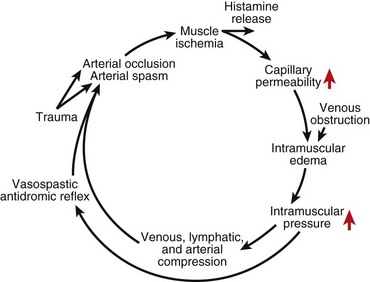
Any situation that causes a decrease in compartment size or increase in compartment pressure can initiate compartment syndrome. As the intracompartmental pressure increases, capillary blood perfusion is reduced to a level that cannot maintain tissue viability. The increase in interstitial pressure overcomes the intravascular pressure of the small vessels and capillaries, causing the walls to collapse and impeding local blood flow. In a canine model, muscle necrosis was shown to occur with a rise in pressure to within 20 mm below diastolic pressure. The local tissue ischemia leads to local edema, which increases intracompartmental pressure. This cycle of increasing muscle ischemia was depicted by Eaton and Green as shown in Figure 74-4.
Diagnosis
Measuring Compartment Pressures in the Forearm and Hand Using a Hand-Held Monitoring Device











Management
Acute Compartment Syndrome of the Forearm
Forearm Fasciotomy and Arterial Exploration
 For the volar fasciotomy, make a curvilinear incision similar to McConnell’s combined exposure of the median and ulnar nerve neurovascular bundles as described by Henry (Fig. 74-5). Make an anterior curvilinear incision medial to the biceps tendon, crossing the elbow flexion crease at an angle. Carry the incision distally into the palm to allow for a carpal tunnel release, but avoid crossing the wrist flexion crease at a right angle.
For the volar fasciotomy, make a curvilinear incision similar to McConnell’s combined exposure of the median and ulnar nerve neurovascular bundles as described by Henry (Fig. 74-5). Make an anterior curvilinear incision medial to the biceps tendon, crossing the elbow flexion crease at an angle. Carry the incision distally into the palm to allow for a carpal tunnel release, but avoid crossing the wrist flexion crease at a right angle.
 Divide the lacertus fibrosus proximally, and evacuate any hematoma.
Divide the lacertus fibrosus proximally, and evacuate any hematoma.







 Do not close the skin at this time; anticipate secondary closure later.
Do not close the skin at this time; anticipate secondary closure later.




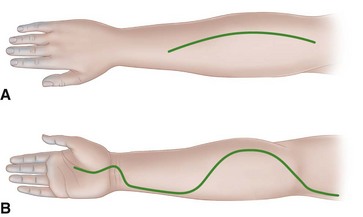
FIGURE 74-5 Incisions used in forearm in severe Volkmann contracture. A, Extensive opening of fascia of dorsum of forearm in dorsal compartment syndromes. B, Incision used for anterior forearm compartment syndromes in which skin and underlying fascia are released completely throughout. SEE TECHNIQUES 74-2, 74-4, AND 74-5.
Postoperative Care
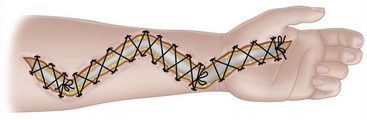
The arm is elevated for 24 to 48 hours after surgery. If closure is not possible within 5 days, a split-thickness skin graft should be applied. Alternatively, closure of fasciotomy wounds can be accomplished gradually with progressive tension using vessel loops. The vessel loops are tightened progressively postoperatively during dressing changes. Wound closure by this method usually can be accomplished in 2 weeks (Fig. 74-6). A vacuum-assisted wound closure system may be used to assist in wound management. The splint is worn until sutures are removed or as determined by fracture care.
Hand Fasciotomies
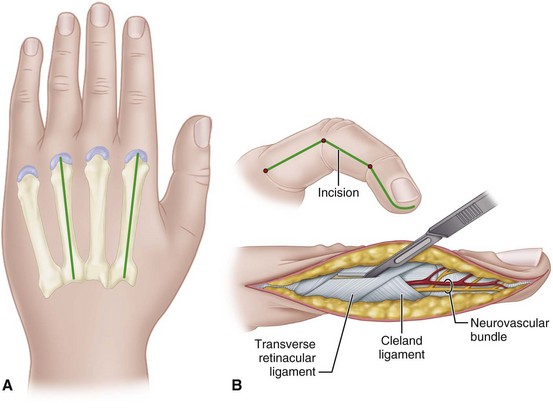
 Make two dorsal parallel incisions through the skin overlying the second and fourth metacarpals, beginning at the level of the metacarpophalangeal joints and extending just distal to the wrist (Fig. 74-7A). Make each incision down to the musculofascial area.
Make two dorsal parallel incisions through the skin overlying the second and fourth metacarpals, beginning at the level of the metacarpophalangeal joints and extending just distal to the wrist (Fig. 74-7A). Make each incision down to the musculofascial area.



 Release the carpal tunnel through a palmar midline incision.
Release the carpal tunnel through a palmar midline incision.
 Do not attempt to débride the interosseous muscles at this point. If the fingers are tensely swollen, and capillary refill is delayed, continue with digital fasciotomies through midlateral incisions along the radial border of the ring and small fingers and the ulnar border of the index and long fingers (Fig. 74-7B).
Do not attempt to débride the interosseous muscles at this point. If the fingers are tensely swollen, and capillary refill is delayed, continue with digital fasciotomies through midlateral incisions along the radial border of the ring and small fingers and the ulnar border of the index and long fingers (Fig. 74-7B).


Established Volkmann Contracture of the Forearm
If a compartment syndrome is untreated or inadequately treated, compartment pressures continue to increase until irreversible tissue ischemia occurs. Volkmann ischemic contracture is the result of several different degrees of tissue injury; however, the earliest changes usually involve the flexor digitorum profundus muscles in the middle third of the forearm (Fig. 74-8). The typical clinical picture of established Volkmann contracture includes elbow flexion, forearm pronation, wrist flexion, thumb adduction, metacarpophalangeal joint extension, and finger flexion.
A severe contracture involves the flexors and extensors of the forearm. Fractures of the forearm bones and scars on the skin also may be present. Sensory feedback usually is impaired because the nerves are strangulated by the contracted and scarred muscles surrounding them. The preferred treatment in these instances is early excision of all necrotic muscles, combined with complete median and ulnar neurolysis to restore sensibility and possibly intrinsic function. Although one author recommended this be done no sooner than 3 months but no later than 1 year after the ischemic event, others have recommended surgical intervention within 3 weeks to prevent additional contractures from developing. Tendon transfers to restore function should be performed as a secondary procedure. These may include transfer of the brachioradialis to the flexor pollicis longus and the extensor carpi radialis longus to the flexor digitorum profundus tendons. If motors to restore finger flexion are unavailable, a free innervated muscle transfer using the gracilis muscle may be considered (see Chapter 63). In one long-term study (32 years), substantial improvement was noted with excision of fibrotic muscle, neurolysis, and tendon transfers or free gracilis transfer; however, tendon lengthening alone rarely was satisfactory. Oishi and Ezaki recommended for severe Volkmann ischemic contracture a two-stage procedure with initial muscle débridement and neurolysis followed by a free functioning gracilis transfer after return of sensation and intrinsics to the hand. Satisfactory results also have been reported using a free medial gastrocnemius myocutaneous flap for reconstruction in patients with established Volkmann contracture.
Muscle Sliding Operation of Flexors for Established Volkmann Contracture
The muscle sliding operation was first described by Page in 1923 and was endorsed by Scaglietti in 1957. It has been used for Volkmann and other contractures caused by conditions such as brain damage and burns. In the case of Volkmann contracture, usually the muscle is fibrotic and noncontractile and a muscle sliding operation alone is rarely indicated. For this technique, see Chapter 72.
Excision of Necrotic Muscles Combined with Neurolysis of Median and Ulnar Nerves for Severe Contracture
 Make an extensive volar forearm incision (see Fig. 74-5), and excise all avascular masses of the flexor profundus and sublimis muscles, leaving any muscle that might survive or appears viable.
Make an extensive volar forearm incision (see Fig. 74-5), and excise all avascular masses of the flexor profundus and sublimis muscles, leaving any muscle that might survive or appears viable.



This is a salvage procedure that may result in only modest improvement. If the contracture is diffuse but incomplete throughout all digital and wrist flexors, the muscle sliding technique may be considered (see Chapter 72).
Two-Staged Free Gracilis Transfer
First Stage






Second Stage
 Identify the brachial artery in the forearm and follow it distally to determine its suitability or that of any branches. Also identify a vein for anastomosis because the vena comitantes or subcutaneous veins may not be suitable.
Identify the brachial artery in the forearm and follow it distally to determine its suitability or that of any branches. Also identify a vein for anastomosis because the vena comitantes or subcutaneous veins may not be suitable.










 Flex the wrist to ensure that the tenodesis allows the fingers to extend appropriately.
Flex the wrist to ensure that the tenodesis allows the fingers to extend appropriately.

Established Intrinsic Muscle Contractures of the Hand
The proper surgical release of established intrinsic muscle contractures depends on the severity of the contractures. When the contractures are mild (Fig. 74-9), the metacarpophalangeal joints can be passively extended completely, but while they are held extended, the proximal interphalangeal joints cannot be flexed (positive intrinsic tightness test); the distal intrinsic release of Littler may be indicated (Fig. 74-10).

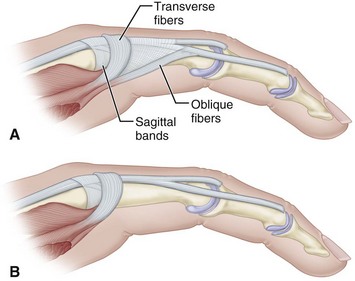
FIGURE 74-10 Littler release of intrinsic contracture. A, Extensor aponeurosis at level of metacarpophalangeal joint consists of long extensor tendon, transverse fibers (which flex metacarpophalangeal joint), and oblique fibers (which extend interphalangeal joint). Crosshatched part is resected from each side of hood. B, Appearance of aponeurosis after release. SEE TECHNIQUE 74-6.
In contractures that are more severe, the interosseous muscles are viable but contracted and the intrinsic tightness test is positive. Active spreading of the fingers may be possible. In these instances, the contracted muscles may be released from the metacarpal shafts by a muscle sliding operation (Fig. 74-11A).
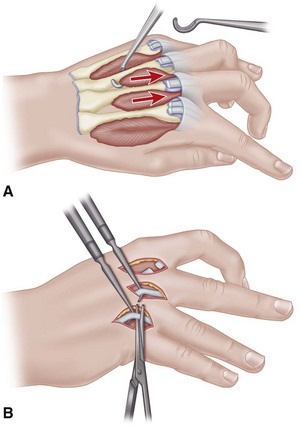
In the most severe contractures, the intrinsic muscles not only may be contracted but also necrotic and fibrosed, so any useful muscle excursion is absent. In these instances, the tendon of each muscle must be divided to release the contractures (Fig. 74-11B). Other procedures, such as capsulotomies and tendon transfers, also may be necessary.
Release of Established Intrinsic Muscle Contractures of the Hand
 The same procedure is done on any finger as needed.
The same procedure is done on any finger as needed.
 Make a single midline incision on the dorsum of the proximal phalanx extending from the metacarpophalangeal joint to the proximal interphalangeal joint to allow good exposure of both sides of the extensor aponeurosis. Incise the insertion of the oblique fibers of the extensor aponeurosis into the extensor tendon; make the incision parallel with the tendon (see Fig. 74-10A).
Make a single midline incision on the dorsum of the proximal phalanx extending from the metacarpophalangeal joint to the proximal interphalangeal joint to allow good exposure of both sides of the extensor aponeurosis. Incise the insertion of the oblique fibers of the extensor aponeurosis into the extensor tendon; make the incision parallel with the tendon (see Fig. 74-10A).

 After adequate excision of the oblique fibers, the proximal interphalangeal joint should have full passive flexion with the metacarpophalangeal joints in neutral (see Fig. 74-10B).
After adequate excision of the oblique fibers, the proximal interphalangeal joint should have full passive flexion with the metacarpophalangeal joints in neutral (see Fig. 74-10B).







Adducted Thumb
Crushing injuries, infections, or deep burns result in extensive fibrosis within the thumb web that cannot be treated by release of the skin alone; rather, the scarred components of the contracted skin, muscle, fascia, and capsule must be excised with care to avoid damaging the radial artery near the carpometacarpal joint. This excision produces a deep fissure that must be filled with skin and subcutaneous fat to provide an elastic functioning web. Usually this can be accomplished by dorsal rotation or a sliding flap with supplemental skin grafting (Figs. 74-12 and 74-13). If adjacent dorsal skin is unsuitable for transfer, a cross arm flap may be considered. The cross arm flap is fashioned as a double triangle, one on the dorsal surface and one on the volar surface of the web, to eliminate any line of scar paralleling the border of the web. The first and second metacarpals are fixed in the desired position with Kirschner wires. When motion in the carpometacarpal joint can be restored, any necessary tendon transfers for apposition can be done later, but if motion cannot be restored, the carpometacarpal joint must be arthrodesed to maintain the new position of the thumb permanently.
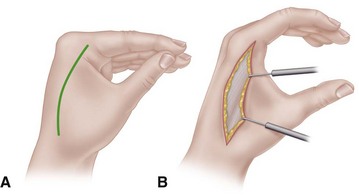
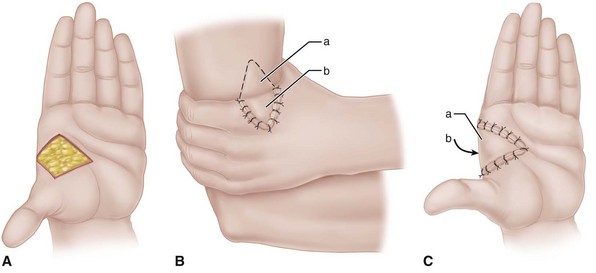
Paralysis of the muscles of apposition can result in secondary contracture of the skin and joint capsule and in contracture of the thumb web, requiring release by a Z-plasty or by a local flap and a skin graft as described by Brand and Milford (see Fig. 74-13). Contracted fascia and bands of muscle must be released, and capsulotomy of the carpometacarpal joint must be done at the same time.
Occasionally, a useless index finger may provide a filleted pedicle with which a satisfactory thumb web can be constructed in one stage. This procedure not only widens the web in that the index metacarpal is excised but also provides skin that can be repositioned over a nearby defect or scar (see discussion of filleted graft in Chapter 65).
Compartment Syndrome and Volkmann Contracture
Boody AR, Wongworawat MD. Accuracy in the measurement of compartment pressures: a comparison of three commonly used devices. J Bone Joint Surg. 2005;87A:2415.
Croutzet P, Chassat R, Masmejean EH. Mini-invasive surgery for chronic exertional compartment syndrome of the forearm: a new technique. Tech Hand Up Extrem Surg. 2009;13:137.
Elliott KG, Johnstone AJ. Diagnosing acute compartment syndrome. J Bone Joint Surg. 2003;85B:625.
Grottkau BE, Epps HR, Di Scala C. Compartment syndrome in children and adolescents. J Pediatr Surg. 2005;40:678.
Gülgönen A. Invited review article. Surgery for Volkmann’s ischaemic contracture. J Hand Surg. 2001;26B:283.
Hovius SER, Ultee J. Volkmann’s ischemic contracture: prevention and treatment. Hand Clin. 2000;16:647.
Hwang RW, de Witte PB, Ring D. Compartment syndrome associated with distal radial fracture and ipsilateral elbow injury. J Bone Joint Surg. 2009;91A:642.
Kalyani BS, Fisher BE, Roberts CS, Giannoudis PV. Compartment syndrome of the forearm: a systematic review. J Hand Surg. 2011;36A:535.
Kumar PR, Jenkins JPR, Hodgson SP. Bilateral chronic exertional compartment syndrome of the dorsal part of the forearm: the role of magnetic resonance imaging in diagnosis: a case report. J Bone Joint Surg. 2003;85A:1557.
Lipschitz AH, Lifchez SD. Measurement of compartment pressures in the hand and forearm. J Hand Surg. 2010;35A:1893.
McQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome: who is at risk? J Bone Joint Surg. 2000;82B:200.
Oishi SN, Ezaki M. Free gracilis transfer to restore finger flexion in Volkmann ischemic contracture. Tech Hand Upper Extrem Surg. 2010;14:104.
Ronel DN, Mtui E, Nolan WB, 3rd. Forearm compartment syndrome: anatomical analysis of surgical approaches to the deep space. Plast Reconstr Surg. 2004;114:697.
Ultee J, Hovius SER. Functional results after treatment of Volkmann’s ischemic contracture. Clin Orthop Relat Res. 2005;431:42.
Van den Brand JG, Nelson T, Verleisdonk EG, van derWerken C. The diagnostic value of intracompartmental pressure measurement, magnetic resonance imaging, and near-infrared spectroscopy in chronic exertional compartment syndrome: a prospective study in 50 patients. Am J Sports Med. 2005;33:699.
Verleisdonk EJ, van Gils A, van der Werken C. The diagnostic value of MRI scans for the diagnosis of chronic exertional compartment syndrome of the lower leg. Skeletal Radiol. 2001;30:321.
Yang CC, Chang DS, Webb LX. Vacuum-assisted closure for fasciotomy wounds following compartment syndrome of the leg. J Surg Orthop Adv. 2006;15:19.
Yuan PS, Pring ME, Gaynor TP, et al. Compartment syndrome following intramedullary fixation of pediatric forearm fractures. J Pediatr Orthop. 2004;24:370.
Compartment Syndrome and Volkmann Contracture
Allen MJ, Barnes MR. Chronic compartment syndrome of the flexor muscles in the forearm: a case report. J Hand Surg. 1989;14B:47.
Allen MJ, Steingold RF, Kotecha M, et al. The importance of the deep volar compartment in crush injuries of the forearm. Injury. 1985;16:273.
Amendola A, Rorabeck CH, Vallett D, et al. The use of magnetic resonance imaging in exertional compartment syndromes. Am J Sports Med. 1990;18:29.
Asgari MM, Spinelli HM. The vessel loop shoelace technique for closure of fasciotomy wounds. Ann Plast Surg. 1999;43:225.
Broström L-A, Stark A, Svartengren G. Acute compartment syndrome in forearm fractures. Acta Orthop Scand. 1990;61:50.
Brumback RJ. Compartment syndrome complicating avulsion of the origin of the triceps muscle. J Bone Joint Surg. 1987;69A:1445.
Bunnell S. Ischaemic contracture, local, in the hand. J Bone Joint Surg. 1953;35A:88.
Chuang DC, Carver N, Wei FC. A new strategy to prevent the sequelae of severe Volkmann’s ischemia. Plast Reconstr Surg. 1996;98:1023.
Dellaero DT, Levin LS. Compartment syndrome of the hand: etiology, diagnosis, and treatment. Am J Orthop. 1996;25:404.
Eaton RG, Green WT. Epimysiotomy and fasciotomy in the treatment of Volkmann’s ischemic contracture. Orthop Clin North Am. 1972;3:175.
Eichler GR, Lipscomb PR. The changing treatment of Volkmann’s contractures from 1955 to 1965 at the Mayo Clinic. Clin Orthop Relat Res. 1967;50:215.
Fazi B, Raves JJ, Young JC, et al. Fasciotomy of the upper extremity in the patient with trauma. Surg Gynecol Obstet. 1987;165:447.
Gainor BJ. Closed avulsion of the flexor digitorum superficialis origin causing compartment syndrome: a case report. J Bone Joint Surg. 1984;66A:467.
Gelberman RH, Garfin SR, Hergenroeder PT, et al. Compartment syndromes of the forearm: diagnosis and treatment. Clin Orthop Relat Res. 1981;161:252.
Gelberman RH, Zakaib GS, Mubarak SJ, et al. Decompression of forearm compartment syndrome. Clin Orthop Relat Res. 1978;134:225.
Goldie BS, Jones NF, Jupiter JB. Recurrent compartment syndrome and Volkmann contracture associated with chronic osteomyelitis of the ulna. J Bone Joint Surg. 1990;72A:131.
Green TL, Louis DS. Compartment syndrome of the arm: a complication of the pneumatic tourniquet: a case report. J Bone Joint Surg. 1983;65A:270.
Halpern AA, Mochizuki RM. Compartment syndrome of the interosseous muscles of hand: a clinical and anatomic review. Orthop Rev. 1980;9:121.
Harris C, Jr., Riordan DC. Intrinsic contracture in the hand and its surgical treatment. J Bone Joint Surg. 1954;36A:10.
Hastings H, Misamore G. Compartment syndrome resulting from intravenous regional anesthesia. J Hand Surg. 1987;12A:559.
Hazeltine M, Duranceau L, Gariepy G. Presentation of breast carcinoma as Volkmann’s contracture due to skeletal muscle metastases. J Rheumatol. 1990;17:1097.
Henry AK. Exposures of long bones and other surgical methods. Bristol, England: John Wright & Sons; 1927.
Heppenstall RB, Sapega AA, Scott R, et al. The compartment syndrome: an experimental and clinical study of muscular energy metabolism using phosphorus nuclear magnetic resonance spectroscopy. Clin Orthop Relat Res. 1988;226:138.
Hung LK, Kinninmonth WG, Woo ML. Vibrio vulnificus necrotizing fasciitis presenting with compartmental syndrome of the hand. J Hand Surg. 1988;13B:337.
Jones R. Address on Volkmann’s contracture with specific reference to treatment. BMJ. 1928;2:639.
Kline SC, Moore JR. Neonatal compartment syndrome. J Hand Surg. 1992;17A:256.
Kutz JE, Singer R, Lindsay M. Chronic exertional compartment syndrome of the forearm: a case report. J Hand Surg. 1985;10A:302.
Littler JW. The hand and upper extremity. In: Converse, JM, ed. Reconstructive plastic surgery. Philadelphia: WB Saunders, 1977.
Liu XY, Ge BF, Win YM, et al. Free medial gastrocnemius myocutaneous flap transfer with neurovascular anastomosis to treat Volkmann’s contracture of the forearm. Br J Plast Surg. 1992;45:6.
Madigan RR, Hanna WT, Wallace SL. Acute compartment syndrome in hemophilia. J Bone Joint Surg. 1981;63A:1327.
Matava MJ, Whitesides TE, Jr., Seiler JG, 3rd., et al. Determination of the compartment pressure threshold of muscle ischemia in a canine model. J Trauma. 1994;37:50.
Matsen FA, Winquist RA, Krugmire RB. Diagnosis and management of compartmental syndromes. J Bone Joint Surg. 1980;62A:286.
McHale KA, Geissele A, Perlik PD. Compartment syndrome of the biceps brachii compartment following rupture of the long head of the biceps. Orthopedics. 1991;14:787.
Moed BR, Fakhouri AJ. Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma. 1991;5:134.
Mubarak SJ, Carroll NC. Volkmann’s contracture in children: aetiology and prevention. J Bone Joint Surg. 1979;61B:285.
Mubarak SJ, Owen CA, Hargens AR, et al. Acute compartment syndrome: diagnosis and treatment with the aid of the Wick catheter. J Bone Joint Surg. 1978;60A:1091.
Murphy JB. Myositis. JAMA. 1914;63:1240.
Naidu S, Heppenstall RB. Compartment syndrome of the forearm and hand. Hand Clin. 1994;10:13.
O’Neil D, Sheppard JE. Transient compartment syndrome of the forearm resulting from venous congestion from a tourniquet. J Hand Surg. 1989;14A:894.
Page CM. An operation for the relief of flexion-contracture in the forearm. J Bone Joint Surg. 1923;5B:233.
Palumbo RC, Abrams JS. Compartment syndrome of the upper arm. Orthopedics. 1994;17:1144.
Pedowitz RA, Tourounghi FM. Chronic exertional compartment syndrome of the forearm flexor muscles. J Hand Surg. 1988;13A:694.
Ridings P, Gault D. Compartment syndrome of the arm. J Hand Surg. 1994;19B:147.
Rorabeck CH. Tourniquet-induced nerve ischemia: an experimental investigation. J Trauma. 1980;20:280.
Rowland SA, Fasciotomy: the treatment of compartment syndrome. Green, DP, ed. Operative hand surgery, ed 3, New York: Churchill Livingstone, 1993.
Scaglietti O. Sindromi cliniche immediate e tardive da lesioni vascolari nelle fratture degli arti. Riforma Med. 1957;71:749.
Schnall SB, Holtrom PD, Silva E. Compartment syndrome associated with infection of the upper extremity. Clin Orthop Relat Res. 1994;306:128.
Seiler JG, III., Womack S, De L’Aune WR, et al. Intracompartmental pressure measurements in normal forearm. J Orthop Trauma. 1993;7:414.
Sheridan GW, Matsen FA. Fasciotomy in the treatment of acute compartment syndrome. J Bone Joint Surg. 1976;58A:112.
Simpson NS, Jupiter JB. Delayed onset of forearm compartment syndrome: a complication of distal radius fracture in young adults. J Orthop Trauma. 1995;9:411.
Smith RJ, Intrinsic contracture. Operative hand surgery. Green DP, ed. Operative hand surgery, New York, Churchill Livingstone, 1982;vol 1.
Steinberg BD, Gelberman RH. Evaluation of limb compartments with suspected increased interstitial pressure: a noninvasive method for determining quantitative hardness. Clin Orthop Relat Res. 1994;300:248.
Stockley I, Harvey IA, Getty CJM. Acute volar compartment syndrome of the forearm secondary to fractures of the distal radius. Injury. 1988;19:101.
Styf J, Forssblad P, Lundborg G. Chronic compartment syndrome in the first dorsal interosseous muscle. J Hand Surg. 1987;12A:757.
Thomas JJ. Nerve involvement in the ischaemic paralysis and contracture of Volkmann. Ann Surg. 1909;49:330.
Trumble T. Forearm compartment syndrome secondary to leukemic infiltrates. J Hand Surg. 1987;12A:563.
Tsuge K. Treatment of established Volkmann’s contracture. J Bone Joint Surg. 1975;57A:925.
Volkmann R. Die ischaemischen Muskellähmungen und Kontrakturen. Zentralbl Chir. 1881;8:801.
Whitesides TE, Jr., Haney TC, Morimoto K, et al. Tissue pressure measurements as a determinant for the need of fasciotomy. Clin Orthop Relat Res. 1975;113:43.
Whitesides TE, Jr., Harada H, Morimoto K. Compartment syndromes and the role of fasciotomy, its parameters and techniques. Instr Course Lect. 1977;26:179.
Zuker RM, Egerszegi EP, Manktelow RT, et al. Volkmann’s ischemic contracture in children: the results of free vascularized muscle transplantation. Microsurgery. 1991;12:341.
Brand PW, Milford LW, Web deepening with sliding flap for adducted thumb in the hand. Crenshaw, AH, ed. Campbell’s operative orthopaedics, ed 4, St. Louis: CV Mosby, 1963.
Howard LD, Jr. Contracture of the thumb web. J Bone Joint Surg. 1950;32A:267.
Littler JW. The prevention and the correction of adduction contracture of the thumb. Clin Orthop Relat Res. 1959;13:182.