Chapter 22
Common childhood orthopaedic conditions, their care and management
Julia Judd
University Hospital Southampton, Southampton, UK
Introduction
The purpose of this chapter is to review current knowledge and management of paediatric orthopaedic conditions and discuss some of the health issues which affect bone development of children. This will serve as a source of information for nurses caring for children with a musculoskeletal condition in hospital, in the outpatient setting and in primary care. The selected topics, description of the subject matter and the child’s pathway of care are of value to the practitioner in the advancement of their knowledge. The evidence base for this is represented through current literature in the subspecialty of paediatric orthopaedics, although in some areas the evidence may be old or lacking.
Musculoskeletal assessment
In the assessment of children it is important to use your ears, eyes and hands along with listening to the history given by the family and the child. It is vital to obtain a clear history about the presenting problem. The term ‘OLD CART’ is a useful tool for clinical examination (Dawson et al., 2012). Each ‘letter’ aims to prompt the recall of a series of statements which encourages the practitioner to ask the child and family about the Onset of the problem; Location of problems; Duration and Characteristics of symptoms; Associated factors that contribute to the problem; Relieving factors that make the problem better and Treatment so far.
Throughout the assessment the practitioner must take into account the family dynamics and involve the child, however young they are, listening to their description of the problem, using language that is age appropriate and using toys or favourite items to help the child to understand what is being asked. Information needs to be accessible in a variety of forms including written, visual and through play (Dawson et al., 2012). The environment should be friendly and welcoming to alleviate any fear that the child may have in coming into the hospital.
Try and build a rapport with the child before examining them. If they are very young it may be more appropriate to examine them on the parents lap. One format for examination is to use the look, feel, move approach to assess the presenting problem. This involves looking at the problem area, feeling and moving where the problem is and assessing associated joints whilst observing the child’s facial expressions and noticing pain or discomfort.
The orthopaedic practitioner should have sound domain-specific knowledge to be able to clinically assess the child and reach conclusions (Judd 2005). This means knowing what the normal musculoskeletal development for different age groups is and being able to interpret X-rays dependent on the child’s age and the bone or joint that is being assessed. Collectively the history and clinical examination should lead the practitioner to a plan for investigations and diagnosis.
A systematic approach is helpful when assessing a child. Look at the overall appearance, taking note of the child’s colour (pale or healthy), their stature and posture. How does the child stand? Look at the leg alignment. Is there evidence of asymmetry, such as genu varum/valgum (Figure 22.1), an abnormal rotational profile or leg length difference? Is there evidence of dysfunction? For example, tripping up, a limp, reduced range of motion in a joint or disability.

Figure 22.1 Genu Valgum
Normal variants
Many referrals from general practitioners to orthopaedic services relate to concerns regarding deviation from what parents believe to be the norm. Moloney et al., (2006) determined that half of child referrals (53%) to the hospital present with normal variants, predominated by in-toeing gait and flexible flat feet. In-toeing may be caused by femoral anteversion, tibial torsion or metatarsus adductus (forefoot adduction). An out-toeing gait may be due to femoral retroversion, external tibial torsion or flat feet. All of these are normal variants and are expected to resolve naturally with growth.
Developmental dysplasia of the hip, a neuromuscular problem, clubfoot or a slipped capital femoral epiphysis, however, contribute to in-toeing or out-toeing torsional abnormalities and will require orthopaedic intervention. Flat feet are commonly referred as a result of concern raised by a shoe shop. If the foot is flexible with the arch restored on tip toe standing, then parents can be reassured. The normal age for arch development is by age six although, if the child has ligamentous laxity, they may always have normal flexible flat feet. Orthotics are not required to restore an arch in a normal foot and are used only for the symptomatic foot.
Genu varum (bow legs) and genu valgum (knock knees) deformities can be physiological or pathological and diagnosis is made based on the age of the child, X-ray appearances and progression versus resolution. At birth, a baby’s legs are naturally bowed and this can look progressively worse, especially if the child walks at a young age. By the age of two years the legs will straighten, followed by valgus deformity between the ages of three to four years and gradual correction to normal by age six. It is important to exclude pathology such as rickets, Blounts disease or a metaphyseal dysplasia and to be aware that a unilateral deformity is probably pathological in origin.
Common conditions presenting in the neonate, infant, child and young person
Congenital muscular torticollis
Congenital muscular torticollis is a benign condition that is usually detected in early infancy. The baby tilts their head towards the affected side and turns their face in the opposite direction. This is caused by a fibrous tissue mass within the sternocleidomastoid muscle (SCM). The reason for this is unclear, but may be due to in-utero crowding or a decrease in the blood supply to the muscle. On palpation a firm tumour can be felt in the neck and there may be accompanying plagiocephaly (Luther 2002). Hollier et al. (2000) report a high incidence of 1 per 250 live births, associating difficult births as a causative factor. Resolution is usually within four to six months with stretching exercises if the condition is without other association. The incidence of developmental dysplasia of the hip in an infant with torticollis varies between 2–29% and should be excluded with a hip scan at six weeks of age (von Heideken et al., 2006). Physiotherapy is the mainstay of treatment and parents are taught stretching exercises to continue at home. For those who do not respond favourably by twelve months, a surgical release of the SCM is performed.
Developmental dysplasia of the hip
Developmental dysplasia of the hip (DDH) is the term used to describe a spectrum of disorders affecting the infant hip. Previously known as congenital dislocation of the hip (CDH), the term was changed to DDH to reflect that the condition is dynamic, can change and is not always detectable at birth. The hip joint may be dysplastic with a shallow acetabulum (acetabular dysplasia) that is unstable and subluxing or completely dislocated. Early recognition and appropriate treatment by skilled practitioners, predetermines a good outcome. Clinical guidelines (NIPE 2010) promote a uniform approach to infant screening and detecting abnormality promptly. Treatment decisions are determined by abnormal clinical and sonographic examination (Clarke and Castaneda 2012) and are reliant on the competence of the practitioner (RCN 2012). The primary aim of DDH treatment is to achieve a concentric and stable hip joint and ultimately normal development of the acetabulum and proximal femur with minimal possibility for subsequent reconstructive surgical intervention (Bolland et al., 2010). Early osteoarthritis, chronic pain and a reduction in activity levels are all possible sequelae of DDH and the earlier the intervention the more likely a successful outcome.
Aetiology and epidemiology
DDH is the most common congenital newborn defect (75%). The cause is unknown, although there are multifactorial traits; gender, hormonal influence, race, hyperlaxity, uterine malposition, geographic and environmental influences. Box 22.1 outlines some of the associated risk factors. The incidence of true DDH is difficult to determine accurately as the definition lends itself to a broad spectrum of the condition, giving variance to the accurate incidence. Over the years, authors have strived to clarifiy the terminology and there have been improved methods of detection and diagnosis. The introduction of screening of neonates at risk and sonography has improved diagnostic technique (Kokavec and Bialik 2007). Reported incidence of hip instability is as high as 20 per 1000 live births and varies depending on geographic location. Many of these, which are due to ligamentous laxity, stabilise within the first couple of weeks. The incidence of true hip dislocation in the United Kingdom (UK) is reported as one to two per 1000 live births (Clarke and Taylor 2012).
DDH is more common in females, with increased prevalence in first born infants. The latter is believed to be due to the tight structure of the uterus and subsequent reduced capacity for foetal movement. The risk of late DDH was found to be 29% in breech presentation at four to six month follow-up (Imrie et al., 2010), despite normal ultrasound at six weeks. Research studies to assess prophylactic hip abduction splints for this category of patient are ongoing (Clarke and Judd 2012).
Box 22.1 Associated risk factors for DDH
The infant hip is at risk of DDH if the baby is subject to the recognised risk factors. Early appropriate intervention will result in normal hip development in the majority of babies.
Diagnosis
A routine part of the neonate’s postpartum check is hip examination. The practitioner assesses for equal leg length and looks for asymmetry of the gluteal and thigh folds. More importantly, reduced hip abduction and instability are indicative of DDH. In the UK the NHS Newborn and Physical Examination Programme (NIPE) recommend examiners be trained and are competent in the Ortolani and Barlow tests (NIPE 2010). The Barlow test demonstrates hip instability as the hip displaces posteriorly out of the actebulum and the Ortolani test produces an audible clunk as the dislocated hip is relocated back into the acetabulum. Babies with a positive clinical examination and those that meet the screening criteria are referred to a specialist clinic for hip ultrasound (see Box 22.2 and Figure 22.2).
Box 22.2 Infant hip screening criteria (NIPE 2010)
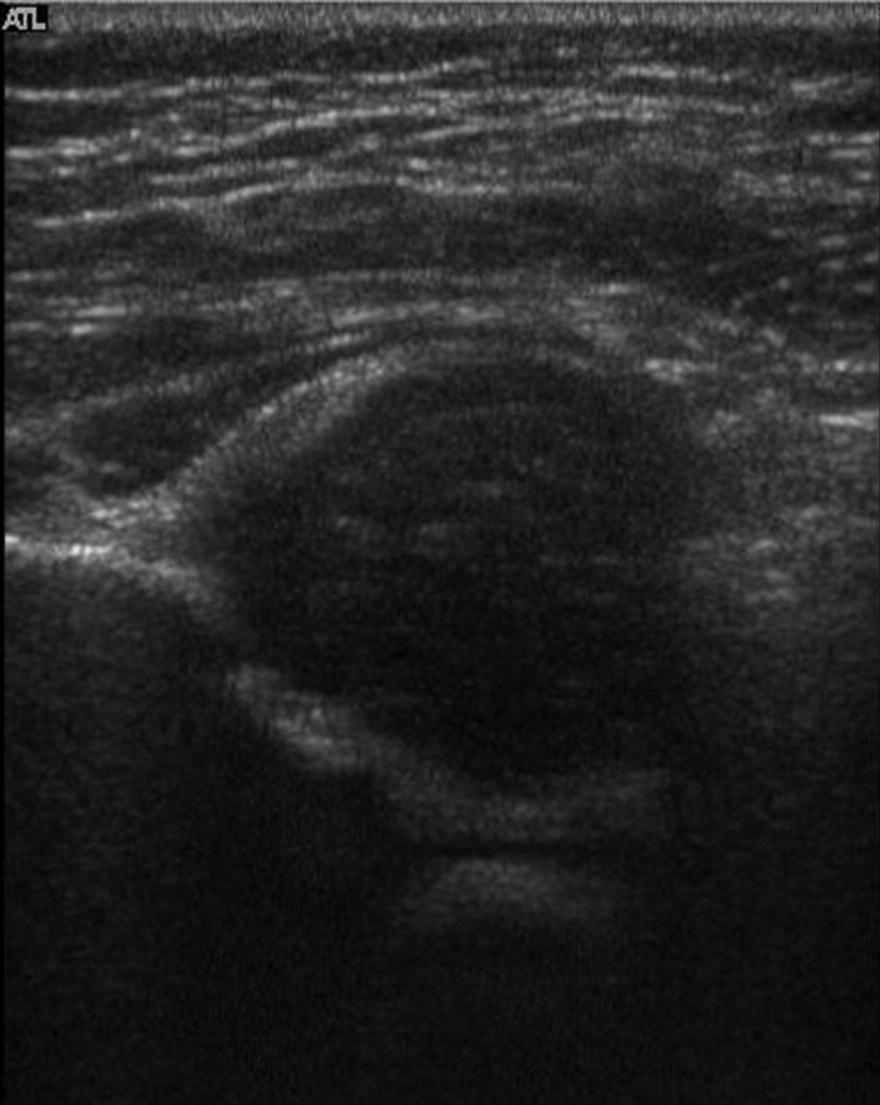
Figure 22.2 Hip ultrasound showing a dysplastic hip
As an adjunct to clinical assessment, ultrasound clarifies clinical findings. It is not feasible, however, to scan all babies’ hips due to the inordinate expense and requirement for resources (American Academy of Pediatrics 2000). Guidelines ensure practitioners make the appropriate referrals at the correct time (Box 22.2).
It is important to obtain a good family and birth history (Judd 2012a) prior to a clinical and sonographic examination. The ossific nucleus (secondary ossification centre) is normally present in the infant’s hip at the approximate age of four months but later in an infant with DDH. An X-ray therefore is not helpful in determining the hip structure and ultrasound is the gold standard to show true hip dislocation or dysplasia. A static coronal view can be measured using the Graf method to assess for dyplasia (Eastwood and de Gheldere 2010). A further dynamic stress test in the transverse plane will assess for instability. Combined, the two images detect the degree of abnormal hip morphology.
Late diagnosis of DDH is commonly detected by the parent who notices their child has a short leg or a limp when there is a unilateral presentation. A child with bilateral dislocated hips will present with a waddling gait. Confirmation is made by X-ray (see Figure 22.4) and clinical examination. Hip abduction is markedly reduced and if unilateral, the affected side shows a shortened limb. The later the diagnosis, the more interventional the treatment and potential for the development of degenerative joint disease. Because DDH is often neglected or treated inappropriately it has become the most common cause of secondary osteoarthritis of the hip.
Guidelines (NIPE 2010) advise the practitioner on when to refer to a specialist paediatric orthopaedic doctor and tested algorithms of treatment are available in the literature (Clarke and Taylor 2012). Multi-centred research studies aim to amalgamate findings to improve knowledge of DDH management and to test new theories. The Institute of Infant Hip Dysplasia (IHDI) strives to create a gold standard for referral and treatment, looking at timing of intervention, method of treatment, failure and complication rates.
Treatment
Treatment of DDH is dependent on the age of the child at presentation (Clarke and Taylor 2012):
Newborn to four months
The Pavlik harness is the most common hip abduction orthosis for the treatment of DDH. Reported as having a 95% success rate, it is effective for dysplastic and unstable hips. It should be abandoned early if a fixed irreducible hip fails to respond to treatment in the first week as there is an increased risk of subsequent avascular necrosis (AVN). It is also contraindicated in neurological hip dislocation (Clarke and Taylor 2012). The harness consists of shoulder and leg straps secured to a chest band (Figure 22.3).

Figure 22.3 Pavlik harness. Reproduced with permission from Wiley.
The optimum position for treatment and prevention of complications, such as femoral nerve palsy and AVN, is 90 degrees of hip flexion and 60 degrees of hip abduction. Weekly ultrasound scans confirm successful treatment and allows the practitioner to check and adjust the harness position and ensure compliance. The infant wears the harness for six weeks full time, following which they are gradually weaned out of it. Follow-up is recommended with serial X-rays until the age of five years to exclude residual dysplasia and late onset complications.
Parents are often upset by the diagnosis and the visual appearance of their baby in the harness. Close observation of the infant and reassurance and support of the parents are required to ensure successful treatment (Atalar et al., 2007). The consequence of not treating the infant’s hip is extremely detrimental and will condemn the child to significant surgical intervention later. It is important to give parents written information on how to care for their baby (Box 22.3 shows an abbreviated sample information leaflet) and advice on appropriate and useful websites (for further information of the care of a baby in a harness, see: www.steps-charity.org.uk).
Early years treatment
Between the ages of 4–12 months, surgical correction is necessary to reduce the hip. For these infants either the Pavlik harness failed and was abandoned early or the diagnosis was not detected on initial clinical examination. Surgical correction is usually deferred until the ossific nucleus is evident on scan, to prevent potential for subsequent AVN (Luedtke et al., 2000).

Figure 22.4 X-ray showing a dislocated left hip: the ossific nucleus is absent
There is some consensus that a week of pre-operative gallows traction to stretch the vascular supply to the femoral head reduces the risk of post-operative AVN although this is not proven (Luedtke et al., 2000). Gallows traction is not a pre-requisite and does not affect whether the hip reduces by closed manipulation or by open surgery. An arthrogram and adductor tenotomy is performed as part of the surgical procedure and if the hip does not reduce concentrically with a closed manipulation, the hip joint is opened to remove obstructing soft tissue such as the labrum. The hip position may be confirmed post-operatively by CT scan to confirm concentric reduction. A hip spica in the human position maintains the femoral head in the acetabulum for six weeks if an open reduction or 12 weeks for a closed reduction (Chapter 21). Sequential broomstick casts (six weeks) and night splint casting (six weeks) may be used to complete the surgical programme (Table 22.1) or as an alternative ring splints or a hip abduction orthosis. For the older child who presents late (aged >18 months) a femoral shortening is required in addition to the open hip reduction to reduce the tension on the hip and protect from AVN. The 18-month-old child is too heavy for Gallows traction as they would be heavier than the upper weight limit of 16 kg (Davis and Barr 1999).
Table 22.1 An example Surgical programme
| Gallows raction | ||
| Closed reduction | Open reduction | |
| Six weeks hip spica | Six weeks hip spica | |
| Six weeks hip spica | Changed under GA | |
| Six weeks Broomstick plasters | Six weeks Broomstick plasters | Changed under GA |
| Six weeks night splints | Six weeks night splints | Changed under GA |
Further surgical procedures
Children who have undergone a closed or open hip reduction for either late presentation or failed Pavlik harness may subsequently need further surgery to improve acetabular cover. Residual hip dysplasia following treatment for DDH has a reported incidence of 2–17% (Cashman et al., 2002). Of those children requiring pelvic osteotomy 60% previously underwent a closed reduction of the hip and 20% open reduction. This is usually by the age of three to four years to prevent progressive dysplasia, instability and eventual early osteoarthritis. The most important predictive factor for further surgery was found to be the initial achievement of a stable concentric reduction at closed or open reduction (Bolland et al., 2010).
A pelvic osteotomy aims to realign the bony structure of the hip joint and therefore the weight bearing forces. A triangular shaped bone graft taken from the iliac crest is inserted into the osteotomy site above the acetabulum. This is fixed with two pins which are removed at six weeks under general anaesthetic (Figure 22.5). Post-operatively the child is nursed in a one and half hip spica cast to immobilse the hip joint until the bone graft has fused. The optimum timing is before school age, giving the femoral head and acetabulum opportunity to remodel with growth.

Figure 22.5 X-ray showing a pelvic osteotomy – the graft is secured with pins
Specific nursing considerations
The child in a hip spica requires considerable care. It is a stressful time for the parents who require support emotionally and practically as well as needing written information on caring for their child (Clarke and McKay 2006).
An epidural is effective pain management for the first 48 hours if the child has had an open hip reduction after which Paracetamol is usually sufficient. This modality can provide excellent pain relief but can also be problematic. The line can migrate (comes out of epidural space), the child requires close observation and monitoring and the epidural site cannot not be visualised due to being covered by the spica.
The spica needs to dry naturally and the child is nursed on pillows alternating from front to back for the first 24 hours. A fibreglass covering is applied on day one post-operatively and waterproof tape is secured around the edges of the spica cast for protection (Sparks et al., 2004). The parents are taught ‘nappy care’ and instructed on the frequency of checking the nappy for dampness and changing promptly to prevent the spica from becoming soiled. The parents should check their child’s skin daily for signs of friction or rash. They can use a cloth to wash their child taking care not to get the cast wet. Hair washing is possible with the child resting on the legs of an adult who sits beside the bath. Holding the child’s head over the edge of the bath, another adult can use the shower attachment to wash the hair.
The child in a spica cast is both heavy and awkward to lift; refer to Chapter 21 to view a picture of a hip spica in the human position. The occupational therapist (OT) can teach the parents handling techniques and how to turn their child safely. An assessment of the home will highlight issues early. A hoist may be required in the home. If the child cannot be securely and safely transported in the car, it may be necessary to arrange ambulance transfer home.
There are a number of ways to clothe a child in a spica. Trousers can be split and Velcro added to secure seams. Dresses are the easiest clothing for girls. Online companies advertise specific clothing made especially for children in spica casts.
Intervention for the young person
As the child gets older, a hip with residual dysplasia will give intrusive pain. A total hip arthroplasty for young and active patients, however, is not the best option. There is a risk of loosening and the revision rates are high. Alternative non-arthroplasty choices for the young patient include proximal femoral and periacetabular osteotomies to re-align the femoral head or re-position the acetabulum to delay the onset of arthritis. Surgical management of the problematic hip in adolescent and young adult patients can be challenging and technically difficult to do. As well as hip pain the patients may also have associated chronic instability. The optimum time for operative intervention is before there is too much wear on the cartilage and before arthritis sets in.
Legg Calvé Perthes disease
Legg Calvé Perthes disease (LCPD) (also known as Perthes disease) is a condition of the child’s hip of unknown aetiology which results in a deformed femoral head due to avascular necrosis. The condition is believed to be due to ischemia of the femoral head due to an interruption of its blood supply. Studies suggest that the articular cartilage, the bony femoral epiphysis, the growing physis and the metaphysis are all affected (Catterall et al., 1982). The aim of treatment, whether conservative or surgical, is to manage the child’s symptoms and preserve hip joint congruency throughout the approximate two year disease process (Herring, 1998). Outcomes of Perthes disease are largely dependent on age at diagnosis as well as on treatment modalities (Daly et al., 1999). Studies suggest that >50% of patients will develop osteoarthritis in their 60s (Perry et al., 2012) and require early total hip replacements. Recent research has investigated the effect of bisphosphonates on animals with induced Perthes. Early results of ongoing research have shown effectiveness on increasing bone density, bone mineral content and strength (Little and Kim 2011).
Aetiology and epidemiology
The cause of Perthes is unknown. A study by Glueck et al. (1996), however, found 75% of participants had abnormal coagulation properties. Thrombophilia as a cause, however, has not been proven and debate regarding the reason for the temporary deficient blood supply of the femoral head continues (Kim 2010). Studies of epidemiology indicate a varied incidence of between 6–15.6 per 100 000. A higher incidence is reported in lower socioeconomic and urban areas and a lower incidence in rural areas. Ethnicity may be a factor as Caucasians are affected more than other races with fewer numbers affected in the African and Chinese populations. It is also more common in the Japanese and in some parts of central Europe (Nochimson 2011). The condition predominantly affects boys from four to eight years and children who are small for their age and have a low BMI (body mass index) (Judd and Wright 2005). The condition is bilateral in 10% of cases.
Diagnosis
The child usually presents to the general practitioner with a history of limp and complaints of pain in either their hip or knee. Clinical examination frequently reveals reduced hip abduction with pain at the extreme of movement on the affected side. An initial radiograph may show evidence of the disease, but often it is the subsequent X-rays or an MRI which demonstrates changes in the appearance of the femoral head and confirms the diagnosis (Dillman and Hernandez 2009) (see Figure 22.6). There is a number of classification systems used to grade the stage of the disease and used in the further monitoring of the disease status (Box 22.4). A bone age (left hand X-ray) is also useful in determining the child’s actual skeletal and chronological ages which assists with treatment planning strategies. MRI can also be used.
Box 22.4 Herring classification for grading stage of Perthes disease (Herring et al., 2004)
The disease process covers an approximate two year period from when the femoral head starts to collapse to the remodeling phase; eventually with the blood supply re-innervated (Figure 22.3). The duration of the disease and its course is variable and treatment outcomes are therefore difficult to predict (Maxwell et al., 2004). During the early stages, when the femoral head is collapsing and softening, there is a risk of extrusion beyond the outer rim of the acetabulum. Left untreated the enlarged femoral head can impinge and become deformed. The best treatment for Perthes disease is debated. The aim of treatment is to prevent femoral head deformity, containing it within the acetabulum to allow for optimal re-modelling and resulting in a better long term outcome (Bowen et al., 2011). However, the expected result is worse if the child is over the age of eight years at diagnosis.

Figure 22.6 X-ray showing Perthes disease of the left hip – note the collapsing femoral head. Reproduced with permission from The Journal of Bone and Joint Surgery, Inc.
Treatment
The treatment of Perthes disease is dependent on the age of the child, the stage of the disease, the X-ray appearance and the child’s symptoms and clinical evaluation. The aim is to maintain femoral head containment through the disease process either non-operatively or operatively. Conservative management includes non-steroidal therapy such as Ibuprofen to minimise inflammation of the hip joint synovium, ‘slings and springs’ traction to maintain hip joint movement, non-adhesive traction and physiotherapy with hydrotherapy. Hip abduction orthoses are used in some centres to protect the femoral head.
Under five years – treatment is usually non-operative with 3–6 monthly X-rays monitoring the hip’s progression with symptoms managed with simple analgesics and a change in lifestyle. The child needs to refrain from impact sports and activities which are likely to cause pain such as jumping from a height. Swimming is recommended to prevent stiffness in the hip and maintain the joint’s range of movement. If symptoms become severe and unmanageable at home, the child may be admitted to hospital. A period of bed rest and hydrotherapy (with or without simple skin traction) is normally sufficient to settle pain and muscle spasm (Judd and Wright, 2005). The child may need to use crutches or a Zimmer frame to assist mobility and offload the affected hip when symptomatic. Occasionally, if symptoms are relentless, the hip can be protected by applying broomstick plasters (Petrie cast) for 4–6 weeks. This is a temporary measure which, in many units, has been replaced with a surgical shelf acetabuloplasty.
Over five years – there are a variety of surgical options to treat Perthes ranging from femoral or pelvic procedures to improve both hip containment and articular congruence.
Shelf acetabuloplasty – the aim is to provide additional cover for the extruding femoral head (Figure 22.7) and facilitate maintenance of a free range of hip movement. In turn the femoral head will remodel in the revascularisation phase of the disease to the shape of the new hip socket. A hip arthrogram is performed to show the cartilaginous component of the femoral head and the degree of subluxation. The shelf is a corticocancellous graft taken from the ilium. It is inserted into a previously made notch on the outer edge of the acetabulum and secured in position by reattaching the reflected head of the rectus femoris muscle (van der Geest et al., 2001). Post-operatively the child may be nursed on simple skin traction for 48 hours to allow muscle spasm to settle, prior to application of a single hip spica to immobilise the hip joint and reduce post-operative pain.

Figure 22.7 X-ray showing Shelf acetabuloplasty of the left hip
Varus derotation femoral osteotomy – reserved for the older child with residual deformity at the end of treatment. The proximal femur is realigned, tilting the femoral head into the acetabulum to achieve improved containment and facilitate femoral remodelling ability. This prevents subluxation and redirects the force through the hip when weight bearing.
Arthrodiastasis – designed to protect the femoral head and preserve its height during the early fragmentation stage of the disease. The hip joint is distracted using an external monolateral fixator for two to six months. The distraction causes the hip joint to open, thereby increasing the space, reducing the weight bearing forces and encouraging restoration of the synovial circulation. Although good results have been achieved, this significant interventional procedure is not without complications; including pin site infection and residual stiffness in the hip and knee joint (Chapter 8). Studies are of small numbers and long-term follow up to skeletal maturity are required to assess whether arthrodiastasis results in a better outcome (Maxwell et al., 2004). From the child’s point of view the fixator is unsightly and cumbersome and psychological support from the outset is recommended.
Slipped capital femoral epiphysis
A slipped capital femoral epiphysis (SCFE) is a condition where the head of the femur slips off the physis. The neck or the metaphysis of the femur is the section that moves, normally migrating anteriorly and superiorly (Sun et al., 2011), while the femoral head maintains its normal position in the acetabulum. The slip occurs through the widened hypertrophic zone of the growth plate and may be acute (sustained after a traumatic episode) or chronic (occurring slowly over a period of time). 25% of cases are bilateral, half of which present sequentially.
Aetiology and epidemiology
The incidence of SCFE is two to three per 100 000 and is more common in male adolescents. Although the cause is unknown, risk factors and associated traits include: obesity, delayed skeletal maturity, hypothyroidism, endocrine abnormalities, puberty and vitamin D deficiency (Clarke and Page 2012). It is suggested that the growth plate plays a part in the cause. The perichondral fibrocartilaginous ring which surrounds the physis contributes to its strength. It is at its strongest during infancy, diminishing as the child gets older. In addition, the physis is widened and therefore potentially weakened during the adolescent growth spurt which is the most common time for a slip to occur. The condition is more common in boys with a ratio of 2.4 per female and more prevalent in the 10–16 year age group in boys (average 13.4 years) and 10–14 year age group in girls (average 11.5 years). Children presenting outside these age perimeters should be investigated for causative factors such as endocrine or systemic disorders.
Diagnosis
A child who presents with pain and a limp over the age of eight years should be investigated for SCFE with an anteroposterior (AP) and frog lateral X-ray views. The AP view is not always helpful and will be normal in 14% of cases (Benson et al., 2002). For a suspected SCFE, which is not evident on X-ray an MRI is useful in detecting a pre-slip (Lalaji et al., 2002) in a child who presents with symptoms.
Slipped Capital Femoral Epiphysis can be classified as (Southwick, 1967):
- acute – symptoms <2 weeks
- chronic – symptoms >2 weeks
- acute-on-chronic – long term pain with a sudden episode of acute pain.
The X-ray findings are described according to the degree of displacement:
- mild (grade 1, 0˚–30˚ of displacement),
- moderate (grade 2, 30˚ to 60˚)
- severe (grade 3, 60˚ to 90˚+).
On presentation with an acute slip the child will complain of pain of less than three weeks’ duration in their groin, thigh or knee. They will limp and have an out-toeing gait. With a chronic slip their symptoms will have been more insidious in nature (Uglow and Clarke 2004). They may be able to weight bear, indicating that the slip is stable. If there is an unstable slip the child is unable to bear weight due to pain. In a severe unstable slip the examination will show a shortened leg lying in external rotation with markedly restricted range of movement. X-ray findings may be subtle or obvious. The AP view will show widening of the physis and a loss of epipyhseal height. There is increased density in the femoral neck (Blanch sign) and Klein’s line drawn up the superior aspect of the femoral neck does not cross the femoral head (see Figure 22.8).
Treatment
The prognosis of SCFE is linked to the prompt recognition of the condition and the severity of the slip. The aim of treatment is to reduce the complication rate of AVN and chondrolysis (Uglow and Clarke 2004). Early intervention within 24 hours of diagnosis reduces the rate of AVN to 7% with surgery; after this time increasing the rate of AVN to 87.5% (Walter et al., 2011). It is important to determine whether the slip is stable or unstable. The latter has a poorer prognosis with increased probability of avascular necrosis whilst a stable slip may deteriorate and become unstable if not treated. Attempting to realign the femoral head will damage the blood supply and risk AVN. Stabilisation of the slip with single screw fixation (see Figure 22.9) is advocated for mild to moderate slips to prevent further slipping and maintain position until physeal fusion (Judd and Wright 2005).
Moderate and severe slips are difficult to manage. Gentle intra–operative reduction of the hip, taking care not to damage the blood supply, is advocated by some surgeons prior to screw fixation. Osteotomies of the femoral neck can be performed to realign the femoral neck in a severe slip but subsequent AVN, chondrolysis and reduced range of hip movement are all significant complications (Lawane et al., 2009). There is some debate whether the contralateral hip of a child with a unilateral slip should be fixed at initial presentation. A study by Riad et al. (2007) demonstrated that the younger the patient, the greater the probability of increased development of a contralateral slip.
Post-operatively the child mobilises non-weight bearing with crutches for the first six weeks, progressing to partial weight bearing for another six weeks. X-rays are taken at each stage to assess position of screw fixation and possible AVN. Patients are followed up radiographically until the physis has fused, negating the possibility of further slippage.
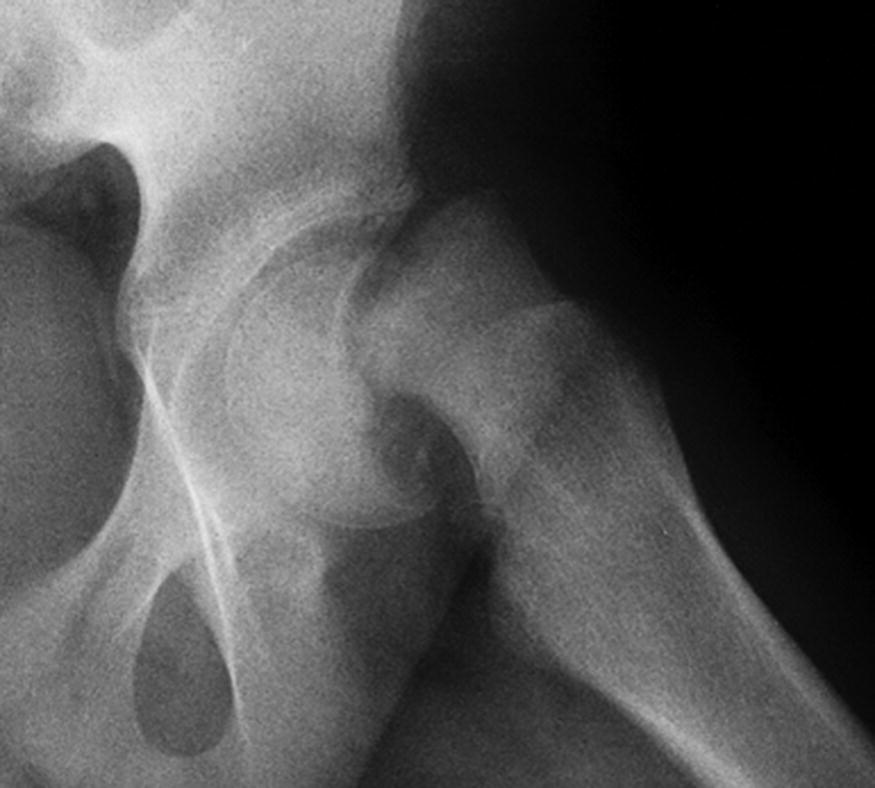
Figure 22.8 X-ray showing slipped left femoral capital epiphysis where Klein’s line does not intersect the epiphysis

Figure 22.9 X-ray showing slipped left femoral capital epiphysis, fixed with a left screw
Vitamin D deficiency
Vitamin D deficiency is associated with rickets, fractures and musculoskeletal symptoms (Judd 2011). Previously thought of as a condition of the past, it is no longer a rarity and is linked to a number of health issues. Studies suggest a concerning association with deformity and generalised bone and muscle pain. In the UK the increase in vitamin D deficiency is attributed to the varied ethnic population, poor diet and lifestyle choices made by families.
Accepted sufficient blood serum levels of vitamin D have been agreed as >75 nmols/L (Pearce and Cheetham 2010) with some variance according to population and environmental factors. Below 20 nmols/L is considered deficient. 80–90% of vitamin D is made through synthesis in the skin and the remaining 10–20% is acquired through diet. In efforts to protect children from sun exposure parents use high factor sun protection creams and cover children’s skin with clothing. A reduction in time spent outdoors due to a preference for indoor activities also contributes to lack of sunlight exposure as do cultural dress codes (Judd and Wright 2011). The best source of vitamin D is exposure to sunlight with 20–30 minutes a day recommended without application of sunscreen (Judd and Wright 2011). Dark skinned children do not synthesise vitamin D well due to increased melanin and are therefore prone to deficiency. In addition to reduced synthesis in the skin, hypovitaminosis D is the primary cause of rickets as it results in poor absorption of calcium and phosphorus minerals from foods. Circulating blood levels of vitamin D are low, resulting in bone softening, non-specific musculoskeletal symptoms and deformity.
Vitamin D deficiency is a global problem and is not restricted to culture, race or demographics. Low vitamin D levels have been associated with musculoskeletal problems such as SCFE, cerebral palsy, fractures and poor bone healing (Clarke and Page 2012). Guidance (DoH 2012) advises practitioners to be aware of at-risk groups within the population and recommends that older people, pregnant women, infants and young children receive vitamin D supplementation.
An X-ray of a child with rickets will show evidence of widened growth plates which have a cupped and splayed appearance (see Figure 22.10). Due to loading on the leg’s long bones, genu varum and valgum is noticeable with abnormality depicted on leg alignment radiographs (see Figure 22.11). Clinical findings are of bowed legs (tibia vara) or knock knees (genu valgum). Skeletal deformity may be symmetric or asymmetric. The wrists and ankles are swollen and enlarged due to reduced mineralisation of the physis. The incidence of fracture and re-fracture rates are increased. There may be permanent skeletal deformities such as rachitic rosary (ends of the ribs are enlarged) and scoliosis. Children may present due to a delay in walking, have poor muscle development and tone and complain of muscle pain.
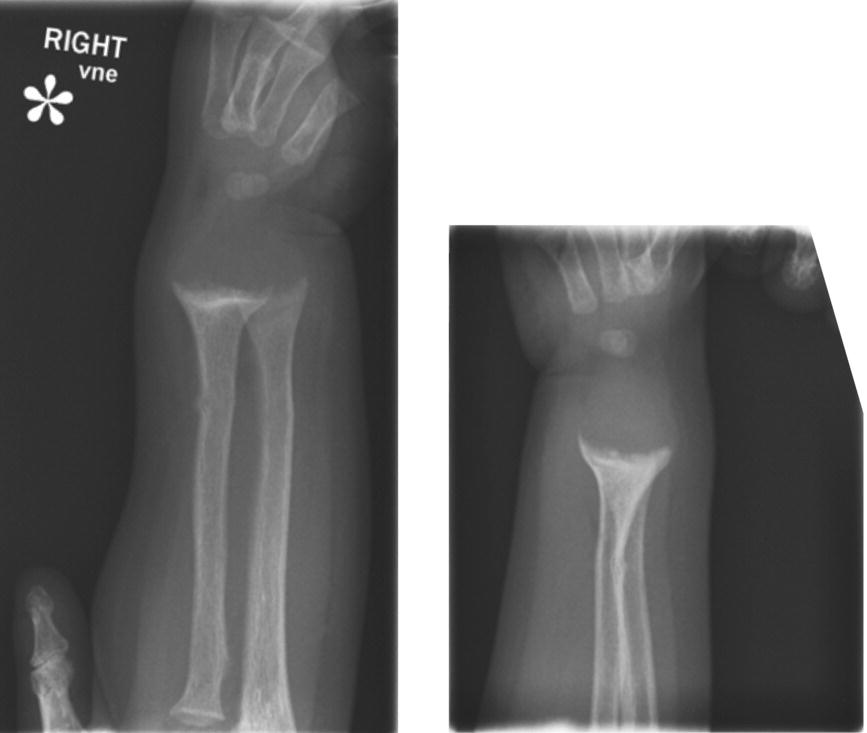
Figure 22.10 Wrist X-ray showing widened and cupped physis
Management
Vitamin D deficiency is an ever-increasing problem with new evidence linking it to a number of health issues. Shared care of the child and family is important with both orthopaedic and endocrinology teams contributing to the overall management. Where levels are simply insufficient (20–75 nmols/L) supplementation of 400 iu per day is recommended. At risk population groups (pregnant women, infants, young children and older people) should receive supplements routinely (Gillie 2006). Deficient levels of vitamin D require a treatment dose of 6000 iu of cholecalciferol daily for three months with calcium supplements for two weeks. Dosages are adjusted according to the results of repeated blood tests at the end of three months (Judd 2012b). Supplementation should be supported by maintaining a dietary intake of vitamin D rich foods (Chapter 10) and adequate exposure to the sun.
Poor diet, whether an excess of the ‘wrong’ foods or a reduced intake of the ‘right’ foods, can contribute to both vitamin D deficiency and future osteoporosis. Obese children tend to have low vitamin D; vitamin D is a fat soluble vitamin and obesity may prevent the storage of the vitamin (Elizondo-Montemayor et al., 2010). An excess consumption of carbonated drinks affects the body’s ability to absorb calcium due to the presence of phosphoric acid (Wyshak 2000). This results in poor bone density and an increased risk of fracture as well as poor fracture healing (Tucker et al., 2006). Eating disorders can result in a reduced intake of calcium and vitamin D; if there is concern review by a dietician, who can advise parents and monitor the child, should be requested.
Uncorrected deformity following treatment with 25 hydroxyvitamin D may need surgical intervention. A classical picture of rickets is deformed leg alignment. Genu varum or valgum can be simply corrected through a minimally invasive procedure using guided growth plates. These slow down the physeal growth on one side whilst the other continues to grow. They are removed when the limbs are clinically straight (Ballal et al., 2010). More invasive procedures are reserved for residual tibia vara, requiring proximal tibial and/or femoral osteotomies (Zaki and Rae 2009). An alternative is to correct the deformity using an external fixator following the osteotomy. The literature reports non-union of the osteotomy, the possibility of fracture through the regenerate and the recurrence of the deformity (Petje et al., 2008, Fucentese et al., 2008, Choi et al., 2002).
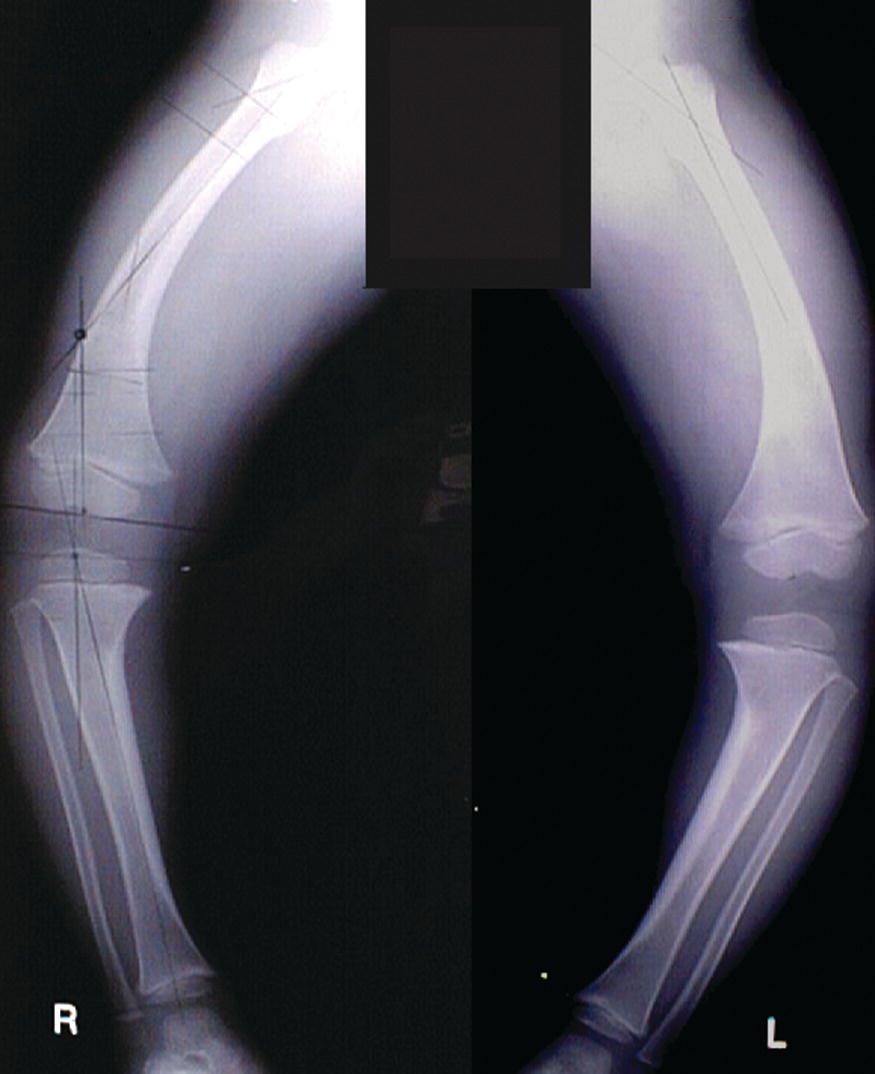
Figure 22.11 X-ray showing rickets
Congenital talipes equino varus
Congenital talipes equino varus (CTEV), or ‘club foot’, is the most common structural deformity of the lower limb present at birth (see Figure 22.12).
The name comes from:
- Congenital – at birth
- Talipes (talus = ankle bone)
- Pes (pes = Foot)
- Equino – characteristic of a horse; the term describes the position of the heel
- Varus – inward turning
The condition involves abnormal alignment of the foot bones and contractures of the joint capsules, ligaments and tendons:
- The deformity is seen at the hindfoot and forefoot
- The heel is in equinus (high) and in varus (turned inward)
- The forefoot is supinated (rotated) and adducted (turned inwards).

Figure 22.12 Club foot (CTEV)
The core problem of the foot deformity is the abnormal positioning of the talus and subsequent malaligned relationship with the calcaneus and navicular bones. Muscle, tissue and vascular structure are all abnormal (Cummings et al., 2002). The deformity may be detected antenatally on the mother’s 20-week ultrasound scan or noted at birth. Pre-natal counselling has proven to be valuable for the expectant parents; giving an explanation of the proposed treatment and reassurance of the excellent functional outcomes (Bar-on et al., 2005). They should be made aware that as the child grows they will notice the affected foot to be shorter by 1–2 sizes and the calf muscle to be thinner.
Aetiology
The cause of club foot (CTEV) is unknown. It occurs in one per 1000 births in Caucasians but varies in different races, with an incidence in Polynesians of 6.8 per 1000 for example. It is bilateral in 50% of cases and more common in males. Strong genetic links are reported in the literature; a sibling has a 30% chance of having club foot deformity and a reported 24% of children with CTEV will have a positive family medical history.
Treatment
Treatment for idiopathic club foot is primarily non-operative, although this may be dependent on place of birth and treatment availability (Judd and Wright, 2005). The overall aim of treatment is to give the child a pain-free, functional ‘foot-shaped’ foot, so they are able to wear normal shoes and perform normal daily activities (Ponseti, 1992). At birth the foot will have varying degrees of stiffness in the hind-foot and forefoot. For the best results, early intervention before the age of one month is advocated since much of the skeleton is cartilaginous, allowing the ligaments, tendons and muscles to be readily stretched (Hart et al., 2005, Ponseti and Smoley 2009).
Prior to initial orthopaedic assessment parents can be taught simple stretching exercises and massage to maintain suppleness in the foot. They are usually extremely keen for their baby to be reviewed by a paediatric orthopaedic specialist and to commence treatment. Information available via the Internet has meant parents have enhanced knowledge and choice regarding their baby’s treatment (Judd 2004).
The management of the foot begins with an assessment of its severity using a grading system. Different assessment tools exist to classify the foot deformity and are useful in the evaluation of patient outcomes (Judd 2004). The Pirani scoring system is a recognised and universally accepted simple tool to use (Dyer and Davis 2006). Divided into sections to give a score for the hind-foot and for the forefoot, it gives an assessment of the flexibility in the foot as a whole (Figure 22.13). An audit of outcomes using the Pirani score as an assessment tool demonstrated that higher total scores and a high hind-foot score predicted a potential relapse of deformity (Goriainov et al., 2010).
Figure 22.13 Pirani score
The Ponseti method is a conservative technique for the treatment of club foot which has gained popularity over the last ten years. Commenced ideally before one month of age, weekly gentle manipulation and application of above knee moulded serial casts, will gradually correct each component of the foot deformity (Figure 22.14). The average number of casts is six, with more or less required dependent on the severity of the foot deformity. Parents can remove the casts in the bath on the morning of the clinic. If done earlier, the foot may relapse from its new position. Parents should be reassured that the treatment is not painful, but their baby will dislike having their leg held still. Feeding at the same time as the procedure is calming (Faulks and Luther 2005).
Approximately 70% of babies will require a percutaneous Achilles tenotomy to correct the heel equinus (Ponseti, 1992, Goriainov et al., 2010). This is commonly performed using a topical anaesthetic cream, following which a final cast is applied for three weeks, holding the ankle in a dorsi-flexed position while the tendon heals in its new position. The final stage of the correction is maintained by the infant wearing ‘boots on a bar’ in the overcorrected position of 70 degrees of abduction (Figure 22.15). These are worn for three months for twenty three hours per day and then at night time only until the age of four.

Figure 22.14 Ponseti cast

Figure 22.15 Boot on a bar
The child is reviewed in the clinic at three to four monthly intervals to review the progress of the foot as it grows. Compliance with the boots and bar can sometimes be problematic and it is vital to ensure they fit correctly, with the heel positioned snuggly down in the boot. Poor outcomes of club foot correction using the Ponseti method have been attributed to lack of compliance with the boot and bar for the four-year duration (Ponseti 1992).
Approximately 20–40% of children will require a tibialis anterior tendon transfer to correct dynamic forefoot supination. Considered to be part of the Ponseti technique, the problem is usually detected in the early years when the child is up and running around. The tendon is transferred into the lateral cuneiform adjusting the muscle pull to bring the forefoot around. Post-operatively a cast is required for six to eight weeks.
Assessment of the atypical club foot
The atypical club foot commonly co-exists with other diagnoses, such as arthrogryposis. It is important to examine the baby by fully assessing the upper and lower limbs and spine and hips, looking for associated anomalies. Assessment of the foot demonstrates a deep posterior heel crease and a deep plantar crease that extends across the entire sole of the foot, creating tightness in the plantar aspect. This type of foot tends not to respond well to conservative management alone and may require minimal surgical intervention (Faulks and Luther 2005).
Surgical correction
Surgical correction is reserved for the recalcitrant club foot, when there is little or no progression in correction with manipulation. The procedure may be minimal, with a soft tissue release, or more interventional addressing all the components of the deformity and requiring a posteromedial plantar lateral release (Cummings et al., 2002). Surgery may be performed in either one or two stages, the latter proven to reduce the incidence of wound infection (Uglow and Clarke 2000). The corrected position is held with casts for three months (Judd and Wright 2005).
Relapsed club foot
Bradish and Noor (2000) report a 20% recurrence rate of clubfoot deformity. Severely stiff feet have a greater tendency to relapse. The child needs regular follow-up throughout growth to detect deformity recurrence, which commonly occurs in the hind foot with reduced ankle dorsiflexion and heel varus. With walking on the lateral border of the foot, forefoot supination may also feature (Ponseti 2002). Surgery may involve capsular releases, tendon transfers or osteotomies. Plaster casts hold the corrected foot for 6–12 weeks depending on the surgery. Routine plaster care and neurovascular observations should be carried out. Pain is controlled with a nerve block and Oramorph initially, with subsequent simple analgesics. If the child has had bony surgery an epidural for 48 hours is optimal (Judd and Wright 2005).
Amplified musculoskeletal pain syndrome
Amplified musculoskeletal pain syndrome (AMPS) is also known as:
- Chronic regional pain syndrome
- Reflex sympathetic dystrophy
- Fibromyalgia.
There is no assumed cause and the pain is increased to a point that the child can no longer manage. Commonly AMPS in children is initiated by minor insignificant trauma, psychological stress or an illness. The trauma maybe a simple fracture or a soft tissue injury and, although the injury itself heals, the pain does not resolve within the expected time frame. The pain pathway is dysfunctional. There is an abnormal short circuit within the spinal cord so that the transmission of pain to the brain is also transmitted to the neurovascular nerves. The signal causes the blood vessels to constrict, resulting in a reduced blood flow and deprivation of oxygen to the bones, muscles and skin. The result is a buildup of acid waste products such as lactic acid with the subsequent production of pain. The new pain signal transmits across the abnormal circuit, further reducing the blood flow and consequently produces more pain (Sherry 2008). How pain is perceived and how individuals cope with pain is influenced by a number of external factors (Chapter 11). The child with AMPS is noted to experience higher levels of stress. The pain, however, not only affects the individual but also has a psychological and social impact on the immediate family.
Signs and symptoms of AMPS may include some or all of the following (Miller, 2003):
- allodynia – pain that comes from a stimulus that is not normally painful e.g. wearing a sock or gentle light touch
- hyperalgesia (increased sensitivity to a pain) – pain that is disproportionate to the injury
- burning sensation
- muscle cramps
- X-rays may reveal some osteoporosis as a result of disuse
- intermittent colour changes of the skin
- shiny appearance or mottling of the skin
- clammy skin or increased sweating
- diffuse swelling
- coolness or warmth of the affected limb
- reduced mobility.
Epidemiology
The majority of children who present with AMPS are female and are from higher socioeconomic backgrounds. It is more common in the adolescent population with a mean age of onset at 12 to 13 years. In a study by Perquin et al. (2000) of 6636 Dutch children, 25% reported recurrent or continuous pain for >3 months. Similarly Roth-Isiqkeit et al.’s (2005) study of 749 children in Germany gave a result of 30.8% reporting symptoms for >6 months. The prevalence is significantly higher in females and is increased with age. The site of symptoms is frequently the lower limb and overall AMPS is the commonest reason for school non-attendance. Predisposing factors to AMPS have been reported as:
- hypermobility
- significant previous pain experiences
- family members response to pain and their coping strategies
- emotional personality – high achievers, pleasers, high anxiety levels.
Management
The patient pathway begins immediately on diagnosis. Early recognition of the problem and prompt action is key to success in treatment (Taylor 2002, Littlejohn 2004). Once all investigations such as bloods, radiographs and scans have proven that there is no organic cause for the pain, medical intervention should be stopped with emphasis placed on rehabilitation (Clinch and Ecclestone, 2009). Management of children with AMPS involves the whole family. A clear discussion with the child and family supported with written information regarding the diagnosis and requirement for involvement with the rehabilitation programme is vital to a successful outcome. It is important to get the child and family on-board (Clinch and Ecclestone 2009) and help them to understand the necessity of physiotherapy and continued compliance. Early intervention for mild symptoms that are suggestive of impending AMPS will abate further deterioration with a reassuring prognosis.
Background history may reveal a role model within the family who has chronic pain (Littlejohn 2004), a major life event as a trigger to symptoms, such as parental marital problems, a house or school move, sporting stressors and high parental expectations. All of these can affect the child’s response to their pain and their involvement and progression with rehabilitation. Family interactions can be intense with enmeshment between the child and mother or sometimes the father.
A major part of the rehabilitation programme is the emphasis on ownership. The child needs to acknowledge that to get better they have to participate at all levels and work with practitioners and therapists to improve. The perception from the child and family may be an expectation that the health professionals will solve the problem. A usual course of action would be to identify the problem, to review what the child can or cannot do and discuss treatment that has failed. This problem-focused approach is negative whereas the aim is for positivity.
Solution-focused approach
The solution-focused approach encourages ownership of the problem, involving the child in their rehabilitation. The focus is to get to the problem via the solution, utilising positive discussion which always focuses on strengths and achievements (Iveson 2002, Sherry et al., 1999). The child is encouraged to think forward to the future and where they would like to be in terms of wellness and activity. ‘Scaling’ is used where the child allocates a score to where they are currently and where they are aiming to get to in their rehabilitation. The aim of the practitioner is to empower the child and encourage them to aim high. A successful tool is to use a scenario where the child endeavors to climb a mountain on which they have placed goals to reach at each stage of improvement. It is crucial that the team have a unified approach, with the nurses and therapists working with the child and family to build a rapport, aiming to help them to reach their goals. Early psychological support may also be useful especially if progress is slow. Guided imagery, externalising the pain, distraction techniques, and teaching the child relaxation methods can all be employed with the assistance of the play specialist. It is important for the team to stress their understanding of the symptoms and not to ignore the fact that the pain exists. However, the pain that the child feels is not harmful or protective of the body. Pain medication is gauged and is dependent on symptoms and progress. It varies from simple analgesics to antidepressants (Amitriptyline) and anticonvulsants (Gabapentin). The latter two are used for neuropathic pain (nerve damage) (Sherry 2008).
Recommended further reading
- Glasper, E.A., McEwing, G. and Richardson, J. (eds) (2007) Oxford Handbook of Children’s and Young People’s Nursing. Oxford University Press, Oxford.
- Kelsey, J. and McEwing, G. (eds) (2008) Clinical Skills in Child Health Practice. Churchill Livingstone Elsevier, Edinburgh.
References
- American Academy of Pediatrics, Committee on Quality Improvement, Subcommittee on Developmental Dysplasia of the Hip (2000) Clinical Practice Guideline: Early Detection of Developmental Dysplasia of the Hip. Pediatrics, 105(4), 896–905.
- Atalar, H., Sayli, U., Yavuz, O.Y., Uras, I. and Dogruel, H. (2007) Indicators of successful use of the Pavlik harness in infants with developmental dysplasia of the hip. International Orthopaedics, 31(2), 145–150.
- Ballal, M.S., Bruce, C.E. and Nayagam, S. (2010) Correcting genu varum and genu valgum in children by guided growth: temporary hemiepiphysiodesis using tension band plates. Journal of Bone Joint Surgery (Britain), 92(2), 273–276.
- Bar-On, E. Mashiach, R. Inbar, O. Weigl, D. Katz, K. and Meizner, I. (2005) Prenatal ultrasound diagnosis of club foot. Outcome and recommendations for counselling and follow up. Journal of Bone and Joint Surgery, 87-B(7), 990–993.
- Benson, M.K.D., Fixsen, J.A., Macnicol, M.F. and Parsch, K. (2002) Children’s Orthopaedics and Fractures. 2nd edn. Churchill Livingstone, London.
- Bolland, B.J., Wahed, A., Al-Hallao, S., Culliford, D.J. and Clarke, N.M.P. (2010) Late reduction in congenital dislocation of the hip and the need for secondary surgery: radiologic predictors and confounding variables. Journal of Pediatric Orthopaedics, 30(7), 676–682.
- Bowen, J.R., Guille, J.T., Jeong, C. et al. (2011) Labral support shelf arthroplasty for containment in early stages of Legg-Calve-Perthes disease. Journal of Pediatric Orthopaedics, 31(2 Suppl), S206–S211.
- Bradish, C.F. and Noor, S. (2000) The Ilizarov method in the management of relapsed clubfeet. Journal of Bone Joint Surgery (British), 82B, 387–391.
- Cashman, J.P., Round, J., Taylor, G. and Clarke, N.M. (2002) The natural history of developmental dysplasia of the hip after early supervised treatment in the Pavlik harness: a prospective, longitudinal follow-up. Journal of Bone Joint Surgery (British), 4–B, 418–412.
- Catterall, A., Pringle, J., Byers, P.D. et al. (1982) A review of the morphology of Perthes’ disease. Journal of Bone and Joint Surgery (Britain), 64(3), 269–275.
- Choi, I.H., Kim, J.K., Chung, C.Y. et al. (2002) Deformity correction of the knee and leg lengthening by Ilizarov method in hypophosphataemic rickets: outcomes and significance of serum phosphate level. Journal of Pediatric Orthopaedics, 22, 626–631.
- Clarke, N.M.P. and Castaneda, P. (2012) Strategies to improve non-operative childhood management. Orthopaedic Clinics of North America, 43, 481–489.
- Clarke, N.M.P. and Judd, J. (2013) La cadera neonatal limítrofe: observación versus Pavlik. Revista Mexicana de Ortopedia Pediátrica, 15(1), 14–18. www.medigraphic.org.mx
- Clarke, N.M.P. and Page, J.E. (2012) Vitamin D deficiency: a paediatric orthopedic perspective. Current Opinion in Pediatrics, 24(1), 46–49.
- Clarke, S. and McKay, M. (2006) An audit of spica cast guidelines for parents and professionals caring for children with developmental dysplasia of the hip. Journal of Orthopaedic Nursing, 10(3), 128–137.
- Clarke, N.M.P. and Taylor, C.C. (2012) Diagnosis and management of developmental hip dysplasia. Paediatrics and Child Health, 22(6), 235–238.
- Clinch, J. and Ecclestone, C. (2009) Chronic musculoskeletal pain in children: assessment and management. Rheumatology, 48(5), 466–474.
- Cummings, R.J., Davidson, R.S., Armstrong, P.F. and Lehman, W.B. (2002) Congenital clubfoot. An instructional course lecture, American Academy of Orthopaedic Surgeons. Journal of Bone and Joint Surgery, 84A(2), 290–308.
- Daly, K., Bruce, C. and Catterall, A. (1999) Lateral shelf acetabuloplasty in Perthes’disease. A review at the end of growth. Journal of Bone and Joint Surgery (Britain) 81, 380–384.
- Davis, P. and Barr, L. (1999) Principles of traction. Journal of Orthopaedic Nursing, 3(4), 222–227.
- Dawson, P., Cook, L., Holliday. LJ. and Reddy, H. (2012) Oxford Handbook of Clinical Skills for Children’s and Young People’s Nursing. Oxford University Press, Oxford.
- Department of Health (DoH) (2012) Vitamin D: Advice On Supplements For At Risk Groups. Available at: http://www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/Dearcolleagueletters/DH_132509 (accessed 3 March 2012).
- Dillman, J.R. and Hernandez, R.J. (2009) MRI of Legg-Calvé-Perthes Disease. The American Journal of Roentgenology, 193 (5), 1394–1407.
- Dyer, P.J. and Davis, N. (2006) The role of the Pirani scoring system in the management of club foot by the Ponseti method. Journal of Bone Joint Surgery (Britain) 88–B(8), 1082–1084.
- Eastwood, D.M. and de Gheldere, A. (2010) Clinical examination for developmental dysplasia of the hip in neonates: how to stay out of trouble. British Medical Journal, 340, c1965.
- Elizondo-Montemayor, L., Ugalde-Casas, P.A., Serrano-González, M., Cuello-García, C.A. and Borbolla-Escoboza, J.R. (2010) Serum 25-hydroxyvitamin d concentration, life factors and obesity in Mexican children. Obesity (Silver Spring), 18(9), 1805–1811.
- Faulks, S. Luther, B. (2005) Changing Paradigm for the Treatment of Clubfeet. Orthopaedic Nursing, 24(1), 25–30.
- Fucentese, S.F. Neuhaus, T.J. Ramseier, L.E. Ulrich Exner, G. (2008) Metabolic and orthopedic management of X-linked vitamin D-resistant hypophosphatemic rickets. Journal of Children’s Orthopaedics, 2(4), 285–291.
- Gillie, O. (2006) A new health policy for sunlight and vitamin D, in Health Research Forum Occasional Reports: No 2. Available at: http://www.healthresearchforum.org.uk/reports/sunbook.pdf (accessed 13 April 2013).
- Glueck, C.J., Crawford, A., Roy, D. et al. (1996) Association of antithrombotic deficiencies and hypofibrinolysis with Legg-Calve Perthes’ Disease. Journal of Bone and Joint Surgery (British), 78A: 3–13.
- Goriainov, V., Judd, J. and Uglow, M. (2010) Does the Pirani score predict relapse in clubfoot? Journal of Childrens Orthopaedics, 4(5), 439–444.
- Hart, E.S., Grottkau, B.E., Rebello, G.N. and Allbright, M.B. (2005) The newborn foot. Diagnosis and management of common conditions. Orthopaedic Nursing, 24(5), 313–321.
- von Heideken, J., Green, D.W., Burke, S.W. et al. (2006) The relationship between developmental dysplasia of the hip and congenital muscular torticollis. Journal of Pediatric Orthopaedics, 26, 805–808.
- Herring, J.A. (1998) Legg-Calve Perthes Disease, in Pediatric Orthopaedic Secrets (ed. L.T. Staheli). Hanley and Belfus, Philadelphia.
- Herring, J.A., Kim, H.T. and Browne, R. (2004) Legg-Calve-Perthes disease. Part I: Classification of radiographs with use of the modified lateral pillar and Stulberg classifications. Journal of Bone and Joint Surgery (America), 86–A(10), 2103–2120.
- Hollier, L., Jeong, K., Grayson, B. and McCarthy, J. 2000 Congenital muscular torticollis and associated craniofacial changes. Plastic and Reconstructive Surgery, 105(3), 827–834.
- Imrie, M., Scott, V., Stearns, P., Bastrom, T. and Mubarak, S.J. (2010) Is ultrasound screening for DDH in babies born breech sufficient? Journal of Children’s Orthopaedics, 4(1), 3–8.
- Institute of Infant Hip Dysplasia (IHDI). www.hipdysplasia.org
- International Association for the Study of Pain (IASP). http://www.iasp-pain.org/Content/NavigationMenu/GeneralResourceLinks/PainDefinitions/default.htm
- Iveson, C. (2002) Solution-focused brief therapy. Advances in Psychiatric Treatment, 8: 149–156. Available at: http://apt.rcpsych.org/content/8/2/149.full (accessed 3 March 2012).
- Judd, J. (2004) Congenital talipes equino varus – evidence for using the Ponseti method of treatment. Journal of Orthopaedic Nursing, 8(3), 160–163.
- Judd, J. (2005) Strategies used by nurses for decision-making in the paediatric orthopaedic setting. Journal of Orthopaedic Nursing, 9(3), 166–171.
- Judd, J. (2011) Rickets: a 21st-century disease? Nursing in Practice (March/April). Available at: www.nursinginpractice.com (accessed 3 March 2012).
- Judd, J. (2012a) History taking, in Oxford Handbook of Clinical Skills for Children’s and Young People’s Nursing (eds P. Dawson, L. Cook, L. Holliday and H. Reddy), Oxford University Press, Oxford.
- Judd, J. (2012b) Rickets in the 21st century: A review of the consequences of low vitamin D and its management. International Journal of Orthopaedic and Trauma Nursing, 17, 199–208.
- Judd, J. and Wright, E. (2005) Joint and Limb Problems in Children. In: Kneale, J. and Davis, P. (Eds) Orthopaedic and Trauma Nursing, 2nd edn. Churchill Livingston, Edinburgh.
- Judd, J. and Wright, E. (2011) Vitamin D deficiency in the paediatric orthopaedic patient: the epidemiology and evidence of sunlight exposure – a follow-up audit on the sun habits of families. Poster presentation, Pediatric Orthopedic Society of North America Conference, 11–14 May 2011.
- Kim, H. (2010) Legg-Calvé-Perthes Disease. A review article. Journal of American Academy of Orthopaedic Surgeons, 18, 676–686.
- Kokavec, M. and Bialik, V. (2007) Developmental dysplasia of the hip. Prevention and real incidence. Bratislavske lekarske listy 108(6), 251–254. Available at: http://www.bmj.sk/2007/10806-03.pdf (accessed 16th September 2012).
- Lalaji, A., Umans, H. and Schneider, R. (2002) MRI features of confirmed ‘pre-slip’ capital femoral epiphysis: a report of two cases. Skeletal Radiology, 31, 362–365.
- Lawane, M., Belouadah, M. and Lefort, G. (2009) Severe slipped capital femoral epiphysis: The Dunn’s operation. Orthopaedics Traumatology and Surgery Research, 95(8), 588–591.
- Little, D.G. and Kim, H.K. (2011) Potential for bisphosphonate treatment in Legg-Calve-Perthes disease. Journal of Pediatric Orthopaedics, 31(2), S182–S188.
- Littlejohn, G.O. (2004) Reflex sympathetic dystrophy in adolescents: lessons for adults. Arthritis and Rheumatism (Arthritis Care and Research), 51(2), 151–153.
- Luedtke, L.M., Flynn, J.M. and Pill, S.G. (2000) Review of avascular necrosis in developmental dysplasia of the hip and contemporary efforts at prevention. The University of Pennsylvania Orthopaedic Journal, 13, 22–28.
- Luther, B.L. (2002) Congenital muscular torticollis. Orthopaedic Nursing, 21(3), 21–28.
- Maxwell, S.L., Lappin, K.J., Kealey, W.D., McDowell, B.C. and Cosgrove, A.P. (2004) Arthrodiastasis in Perthes’ disease. Preliminary results.The Journal of Bone and Joint Surgery (Britain), 86(2), 244–250.
- Miller, R.L.S. (2003) Reflex sympathetic dystrophy. Orthopaedic Nursing, 22(2), 91–99.
- Moloney, D., Heffernan, G., Dodds, M. and McCormack, D. (2006) Normal variants in the paediatric orthopaedic population. Irish Medical Journal, 99(1), 13–14.
- NHS Newborn and Infant Physical Examination Programme (NIPE) (2010) Ultrasound Examination of the Hips in Screening for Developmental Dysplasia of the Hips (DDH) Available at: http://newbornphysical.screening.nhs.uk/standards#fileid10855 (accessed 3 March 2012).
- Nochimson, G. (2011) Legg-Calve-Perthes Disease in Emergency Medicine. Available at: http://emedicine.medscape.com/article/826935 (accessed 16 September 2012).
- Pearce, S.H.S. and Cheetham, T.D. (2010) Diagnosis and management of vitamin D deficiency. British Medical Journal, 340, b5664.
- Perquin, C.W., Hazebroek-Kampschreur, A.A.J.M., Hunfeld, J.A.M. et al. (2000) Pain in children and adolescents: a common experience. Pain, 87(1), 51–58.
- Perry, D.C., Green, D.J., Bruce, C.E. et al. (2012) Abnormalities of vascular structure and function in children with Perthes disease. Pediatrics, 130(1), 126–131.
- Petje, G., Meizer, R., Radler, C., Aigner, N. and Grill, F. (2008) Deformity correction in children with hereditary hypophosphatemic rickets. Clinical Orthopaedics and Related Research, 466 (12), 3078–3085.
- Ponseti, I.V. (1992) Treatment of Congenital Clubfoot. Journal of Bone and Joint Surgery (American), 74A(3), 448–454.
- Ponseti, I.V. and Smoley, E.N. (2009) The classic congenital club foot: the results of treatment. Clinical Orthopaedics and Related Research, 467(5), 1133–1145.
- Riad, J., Bajelidze, G. and Gabos, P.G. (2007) Bilateral slipped capital femoral epiphysis: predictive factors for contralateral slip. Journal of Pediatric Orthopedics, 27(4), 411–414.
- Roth-Isigkeit, A., Thyen, U., Stöven, H., Schwarzenberger, J. and Schmucker, P. (2005) Pain among children and adolescents: restrictions in daily living and triggering factors. Pediatrics, 115(2), e152–e162.
- Royal College of Nursing (RCN) (2012) A Competence Framework for Orthopaedic and Trauma Practitioners. RCN, London.
- Sherry, D., Wallace, C., Kelley, C., Kiddler, M. and Sapp, L. (1999) Short and long-term outcomes of children with complex regional pain syndrome type I treated with exercise therapy. The Clinical Journal of Pain, 15, 218–223.
- Sherry, D. (2008) Amplified musculoskeletal pain: treatment approach and outcomes. Journal of Pediatric Gastroenterology and Nutrition, 47(5), 693–694.
- Southwick, W.O. (1967) Osteotomy through the lesser trochanter for slipped capital femoral epiphysis. Journal of Bone and Joint Surgery, 49–A, 807–835.
- Sparks, L., Rush Ortman, M. and Aubuchon, P. (2004) Care of the child in a body cast. Journal of Orthopaedic Nursing, 8(4), 231–235.
- Sun, W., Li, Z., Shi, Z. et al. (2011) Early and middle term results after surgical treatment for slipped capital femoral epiphysis. Orthopaedic Surgery, 3(1), 22–27.
- Taylor, G.R. and Clarke, N.M.P. (1997) Monitoring the treatment of developmental dysplasia of the hip with the Pavlik harness. Journal of Bone and Joint Surgery (Britain), 79–B, 719–723.
- Taylor, L.M. (2002) Complex regional pain syndrome: comparing adults and adolescents. Topics in Advanced Practice Nursing eJournal 2(2). Available at: http://www.medscape.com/viewarticle/430537_1 (accessed 3 March 2012).
- Tucker, K.L., Morita, K., Qiao, N. et al. ( 2006) Colas, but not other carbonated beverages, are associated with low bone mineral density in older women: The Framingham Osteoporosis Study. American Journal of Clinical Nutrition, 84(4), 936–942.
- Uglow, M.G. and Clarke, N.M.P. (2000) Relapse in staged surgery for congenital talipes equinovarus. Journal of Bone and Joint Surgery (Britain), 82B(5), 739–743.
- Uglow, M.G. and Clarke, N.M.P. (2004) The management of slipped capital femoral epiphysis. Journal of Bone and Joint Surgery (British), 86–B(5), 631–635.
- Walter, K.D., Lin, D.Y. and Schwartz, E. Slipped Capital Femoral Epiphysis. Available at: http://emedicine.medscape.com/article/91596-overview (accessed 16 September 2011).
- Wyshak, G. (2000) Teenaged girls’ carbonated beverage consumption and bone fractures. Archives of Pediatric and Adolescent Medicine, 154(6), 610–613.
- Zaki, S.H. and Rae, P.J. (2009) High tibial valgus osteotomy using the Tomofix plate – Medium-term results in young patients. Acta Orthopædica Belgica, 75, 360–367.
Related posts:
 Professional development, competence and education
The complications of musculoskeletal conditions and trauma
Professional development, competence and education
The complications of musculoskeletal conditions and trauma
 The team approach and nursing roles in orthopaedic and musculoskeletal trauma care
The team approach and nursing roles in orthopaedic and musculoskeletal trauma care
 Soft tissue, peripheral nerveand brachial plexus injury
Soft tissue, peripheral nerveand brachial plexus injury
 Key musculoskeletal interventions
Key musculoskeletal interventions
