Common Bile Duct Surgery and Choledochoduodenostomy
Cystic Duct Anatomy and Variants
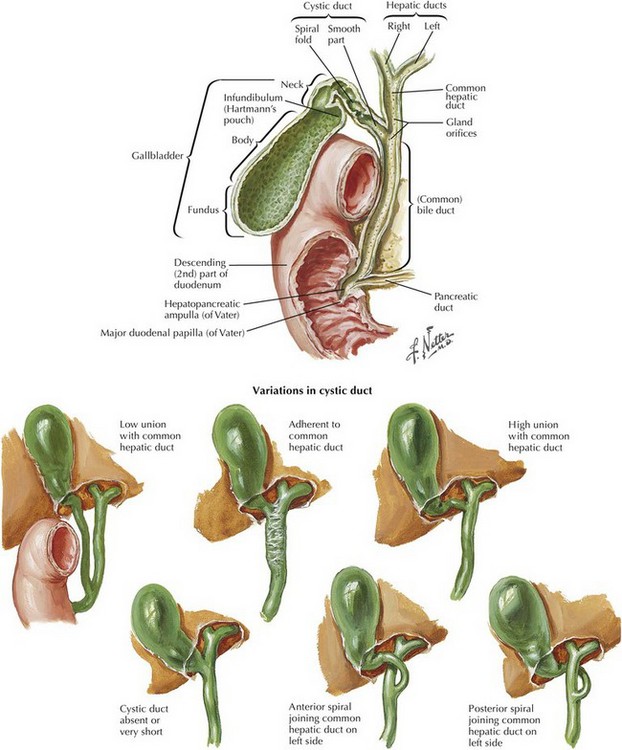
In most individuals (64% to 75%) the cystic duct joins the hepatic duct at approximately a 40-degree angle (Fig. 13-1). Less frequently (17% to 23%) the cystic duct runs parallel to the hepatic duct for a distance and may even enter the duodenum separately. In 8% to 13% of individuals the cystic duct may enter the hepatic duct on the left side after passing in front of or behind the common hepatic duct. Infrequently, the gallbladder may be sessile, with little to no cystic duct.
Laparoscopic Common Bile Duct Exploration
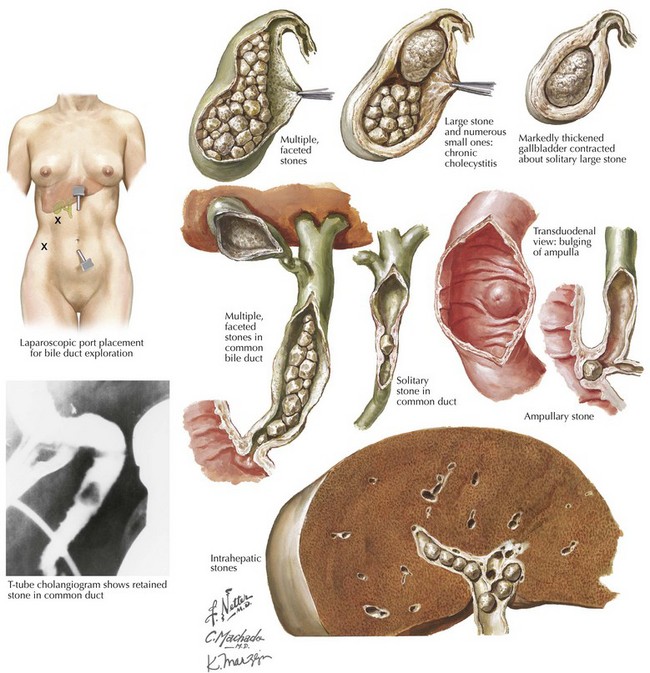
If CBD stones are identified at laparoscopic cholecystectomy, laparoscopic CBD exploration may be warranted (Fig. 13-2). Successful laparoscopic CBD exploration avoids the risks associated with deferring treatment of a CBD stone or a subsequent endoscopic procedure.
Transcystic Approach
The transcystic approach to CBD exploration avoids a choledochotomy and eliminates the subsequent need for a T tube. After controlling the cystic duct on the gallbladder side, a cystic ductotomy is created and a cholangiocatheter placed. The cystic duct may need to be dilated with a balloon before subsequent interventions to extract calculi (Fig. 13-3, A).
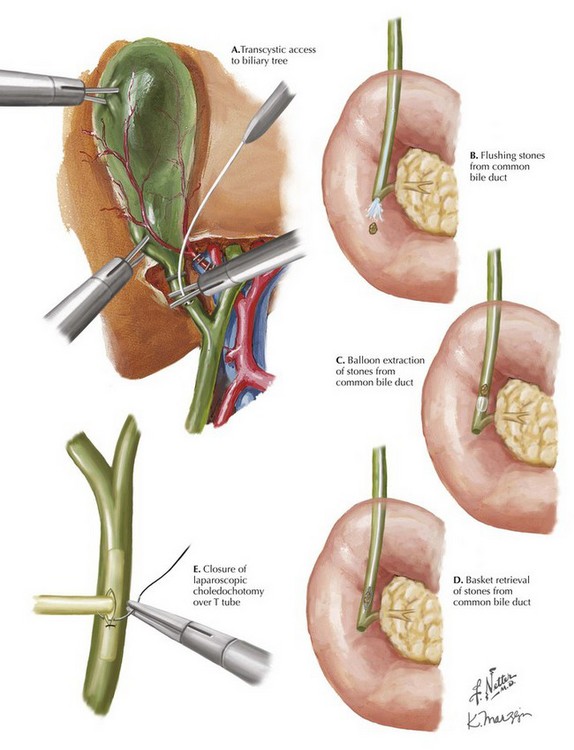
The CBD is irrigated with saline to flush the stone. If unsuccessful, balloon catheters or wire baskets can be passed into the CBD under fluoroscopic guidance to capture and retrieve the stones. An additional option is antegrade balloon dilation of the sphincter under fluoroscopic guidance, followed by flushing to clear the duct of stones (Fig. 13-3, B-D). After clearance of the CBD, the cystic duct is ligated with clips or an endoloop.
Transductal/Choledochotomy Approach
Choledochoscopy can be performed. The choledochotomy is typically closed over a T tube using laparoscopic suturing techniques and absorbable sutures (Fig. 13-3, E). Alternately, an antegrade stent can be placed through the sphincter, and the choledochotomy can be primarily closed without a T tube.
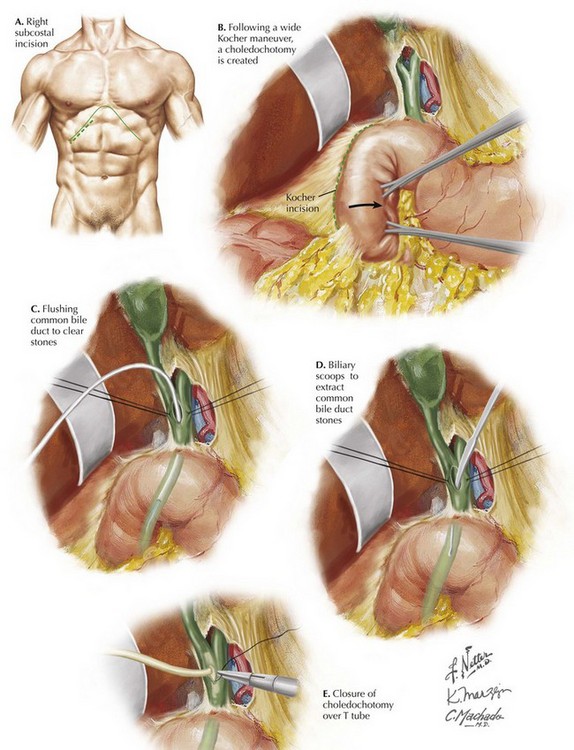
Open Common Duct Exploration
When minimally invasive options are not feasible or fail, open CBD exploration may be warranted. In addition, open exploration may be performed at open cholecystectomy when CBD stones are identified. The procedure is generally performed through a right subcostal incision (Fig. 13-4, A). An upper midline incision may be used as an alternative. After a wide Kocher maneuver, a choledochotomy is created (Fig. 13-4, B). A variety of instruments can be used to extract the stones: irrigation catheters, balloon catheters, biliary scoops, stone forceps, Bakes dilators, and flexible choledochoscopes. After clearance of the CBD, the choledochotomy is closed over a T tube using absorbable sutures (Fig. 13-4, C-E).
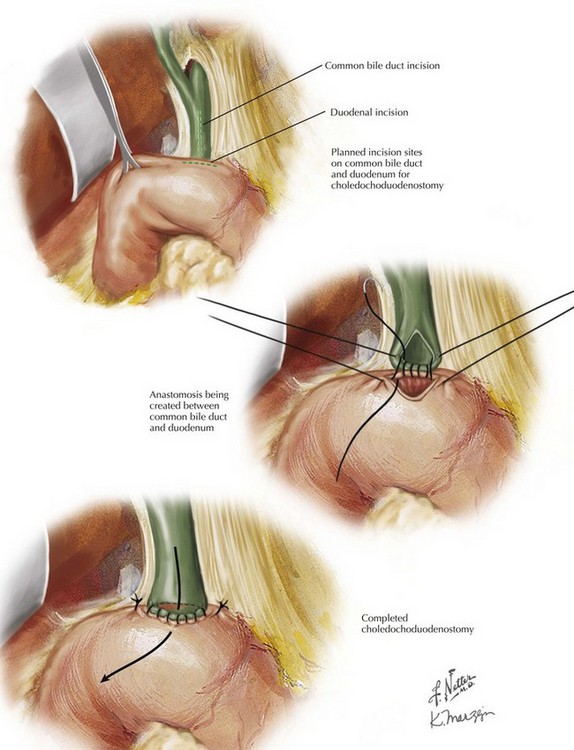
Choledochoduodenostomy
A wide Kocher maneuver is performed and the CBD exposed. A choledochotomy of 2-cm length is made as close to the duodenum as possible. The biliary tree is cleared of calculi. A longitudinal duodenotomy is created, also 2 cm in length and adjacent to the choledochotomy (Fig. 13-5). An anastomosis is created between the CBD and the duodenum using synthetic absorbable sutures.
Cameron, J, Sandone, C. Atlas of gastrointestinal surgery, 2nd ed. Hamilton: BC Decker; 2007.
DeAretxabala, X, Bahamondes, J. Choledochoduodenostomy for common bile duct stones. World J Surg. 1998;22:1171–1174.
Extrahepatic biliary tract and gallbladder. In: Skandalakis J, Colborn G, Weidman T, et al, eds. Skandalakis’ surgical anatomy. Athens: BMP, 2004.
Petelin, JB. Laparoscopic common bile duct exploration. Surg Endosc. 2003;17(11):1705–1714.