[level-membership-for-orthopaedics-category]
Chapter 58 Combined Fractures of the Hip and Femoral Shaft: What Is the Best Treatment Method?
Ipsilateral fractures of the hip and femur are rare injuries that result from high-energy trauma. This injury pattern is most commonly seen in motor vehicle accidents.1,2 The mechanism of injury is an axial force applied along the femur as the occupant’s knee strikes the dashboard. If the hip is adducted when this force is applied, the resulting injury to the hip is usually a dislocation or acetabular fracture, or both. If the hip is in abduction, this will produce a femoral neck and shaft fracture.3 Given the rarity of this injury (i.e., occurring in less than 9% of all femoral shaft fractures), no large series are reported in the literature.1,2, 4 Nearly 60 different implant combinations have been described for this fracture pattern.5,6
OPTIONS
The main complications associated with isolated femoral neck fractures are high rates of nonunion and avascular necrosis of the femoral head. Complications associated with isolated femoral shaft fractures include malunion (i.e., >2 cm shortening, >10-degree varus or valgus alignment, and >20 degrees malrotation) and nonunion. Many authors contend that the complications of the femoral neck trump those of the femoral shaft. They suggest that avascular necrosis is the most significant complication and, therefore, the femoral neck fracture should be treated first.4,7, 8 Others suggest that the femur should be treated initially to allow for ease of closed reduction of the femoral neck fracture.3,5, 9 What are the most common complications of this injury pattern? In what order should fixation of the fractures proceed?
A large number of the femoral neck fractures associated with shaft fractures are missed (approximately 30%).1 Many of the femoral neck fractures are nondisplaced at the time of presentation (25–60%).1 (This may occur because some of the energy that would normally result in a displaced femoral neck fracture is dissipated by the shaft fracture.) In addition, many of these patients have multiple injuries with numerous “distracting” injuries. What is the best method of imaging the hip to avoid missing a fracture?
A spectrum of different hip fractures has been reported with this injury pattern. Hip fractures vary from intertrochanteric fractures to different types of intracapsular neck fractures. The position of the hip (degree of abduction) at the time of injury has been suggested as the determinant of the pattern of hip fracture produced.10 What is the most common type of hip fracture encountered with this injury? What is the most common type of femoral shaft fracture?
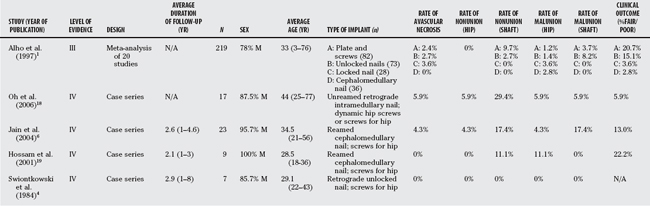
Many different implants and implant combinations have been used to treat this combination of fractures. Implant designs have changed over the time periods of many of the retrospective case series reported in the literature (Table 58-1). For example, the antegrade femoral intramedullary nail has evolved from the unlocked (Küntscher) nail, to the first-generation locked nail, to the second-generation cephalomedullary (or reconstruction) locked nail, and finally to the intramedullary hip screw device. Retrograde femoral nailing has also become increasingly popular since the late 1990s. However, the literature consists of small case series that involve a mixture of different implants from different periods. What are the optimal implants for this fracture pattern?
EVIDENCE
Alho1 conducted a meta-analysis on 65 studies published between 1970 and 1996 that incorporated 722 cases of ipsilateral hip and shaft fractures. This represents the largest summary of case series reported in the literature. He identified 10 studies (240 fractures) that included useful demographic data. This injury typically occurs in young individuals (mean age, 33 years) and results from a high-energy mechanism (85% motor vehicle accidents). Only 1% of cases occurred in elderly individuals. Approximately 18% of the femoral shaft fractures were reported as open, with a large number of comminuted fractures (i.e., 42% were Winquist type III or IV).11 The majority of shaft fractures occurred in the middle third of the femur (72%). For hip fractures, Alho1 reports that the majority of cases were femoral neck fractures (61%), with the rest being trochanteric fractures. Shuler and colleagues10 report on 52 cases of hip fracture with femoral shaft fracture and found 90% to be femoral neck fractures. They found that these hip fractures all tended to extend into the inferomedial neck regardless of the fracture type (i.e., midcervical, basocervical, or pertrochanteric). The extension of the fracture into the inferomedial neck (i.e., femoral calcar) makes it prone to displacement with weight bearing.
Complication rates for femoral neck fractures with an associated femoral shaft fracture tend to be less than with this injury in isolation. Alho1 quotes an avascular necrosis rate of 5% and no nonunions of 254 fractures (this includes displaced and nondisplaced fractures). For isolated displaced femoral neck fractures, the incidence rate of avascular necrosis is 22.5% and of nonunion is 6%.12 The reduced rate of avascular necrosis and nonunion seen with the combined injury may result from a greater rate of nondisplaced fractures (up to 60% for the combined injury),1 perhaps because much of the energy is dissipated through the femoral shaft fracture. Thus, the hip fracture tends to be less comminuted with less injury to the vasculature (i.e., posterior retinacular vessels).
An important consequence of the high rate of nondisplaced femoral neck fractures is that they tend to be missed on initial presentation. Alho1 states that the diagnosis of the hip fracture was delayed (from 1 day to several months) in 30% of cases. Tornetta and investigators13 conducted a Level II study on the effectiveness of a radiographic protocol to detect nondisplaced hip fractures in patients with femoral shaft fractures.13 A standard protocol of computed tomographic (CT) scan, dedicated internal rotation hip radiographs, and lateral intraoperative fluoroscopic hip images for all femoral shaft fractures was instituted, and the rate of missed hip fractures was recorded. This was compared with rates before institution of this protocol (i.e., when imaging was left to the discretion of the treating surgical team). They found that this protocol significantly decreased the rates of missed hip fractures (57% before vs. 6.3% after institution of the protocol). Of these imaging modalities, the authors found the CT scan to be the most useful (a poor-quality CT scan resulted in the only fracture that was missed on CT and subsequently diagnosed on an internal rotation hip radiograph). Thus, all femoral shaft fractures resulting from a high-energy mechanism (especially motor vehicle accidents) should undergo a CT scan of the ipsilateral hip before definitive fixation.
No comparative studies exist in the literature with regard to method of fixation for combined femoral neck and shaft fractures. Alho’s1 meta-analysis took 219 individual cases from 20 studies and segregated them into 4 groups based on fixation of the femoral shaft fracture: (1) plate and screws, (2) unlocked intramedullary nail, (3) first-generation locked intramedullary nail, and (4) cephalomedullary nail. This is Level III evidence given that it is a meta-analysis consisting of small, retrospective, comparative studies and case series. Methods of hip fixation varied among the groups, making the results for complications of the hip fracture unreliable. Alho1 concludes that the locked nailing treatment groups (i.e., first-generation and cephalomedullary nails) had significantly better overall clinical outcomes (P < 0.001) than the plate or unlocked nailing groups. Locked nails also had lower rates of femoral shaft nonunion and malunion (see Table 58-1) than either plating or unlocked nailing. No significant difference was found in rates of complications or clinical outcome noted between first-generation locked and cephalomedullary nails. Alho1 concluded that the femoral shaft fracture was the “key component” to this injury because this fracture exhibited greater complication rates than the hip fracture. In a review of complications associated with ipsilateral hip and femur fractures (level IV evidence), Watson and Moed9 found that 76% of identified complications were nonunion of the femoral shaft fracture. Among these cases of femoral shaft nonunion, they found that 86% were open fractures, 80% were treated with an unreamed nail, 100% had prolonged non–weight bearing, and 30% were treated with a cephalomedullary nail. They conclude that a reamed, second-generation, locked intramedullary nail was the optimal implant for treatment of the femoral shaft fracture in this combined injury.
AREAS OF UNCERTAINTY
Should a Displaced Femoral Neck Fracture Be Fixed before Fixation of the Femoral Shaft?
Numerous authors have advocated that the hip fracture be fixed before the femoral shaft fracture. The most common argument for this approach is that rates of avascular necrosis of the femoral head increase with time to reduction and fixation for displaced femoral neck fractures.4,7, 8 However, no clinical evidence suggests this is, indeed, the case (see Chapter 54). Level II clinical evidence suggests that the outcome of a displaced femoral neck fracture is dependent on anatomic reduction (i.e., no varus) and rigid fixation.14–16 Manipulation of the hip fracture (either through an open or closed approach) is simplified by fixation of the femoral shaft. Thus, we recommend fixation of the femoral shaft before fixation of the displaced femoral neck fracture (Level V evidence). No clinical studies in the literature compare these two approaches.
What Type of Implant Should Be Used for the Femoral Shaft Fracture?
Swiontkowski and colleagues4 advocate fixation of this injury with an unlocked retrograde nail. Treatment of femoral shaft fractures with locked retrograde nails has increased in popularity in recent years. Ricci and coworkers17 conducted a retrospective comparative trial (Level II evidence) for locked antegrade and retrograde nailing of isolated femoral shaft fractures. They found that rates of nonunion and malunion were not significantly different between the two methods of treatment. The incidence of knee pain was significantly greater for the retrograde nail, whereas the incidence of hip pain was significantly greater for the antegrade nail. The authors conclude that these two implants provide similar clinical results for femoral shaft fractures.
The retrograde femoral nail offers theoretical advantages to the antegrade femoral nail for the treatment of ipsilateral hip and femoral shaft fractures. Use of a retrograde nail allows the surgeon to use either a sliding hip screw or cannulated screws to fix the hip fracture, whereas with the use of an antegrade nail, the surgeon is obligated to use screws. With a nondisplaced femoral neck fracture, there is the risk for displacing the fracture when the antegrade nail is introduced. When a retrograde nail is used, the nondisplaced femoral neck fracture can be fixed before nailing the femur. No clinical studies compare these two methods of treatment for this injury. Only case series that show good results for retrograde nailing have been reported (Level IV evidence).4,18 It is our opinion that a retrograde nail should be used to fix the femoral shaft fracture with this injury. We believe that cannulated screws should be used for the femoral neck fracture in patients with adequate bone stock, and a sliding hip screw for patients with osteopenic bone or a combined intertrochanteric fracture (Level V evidence). For nondisplaced femoral neck fractures, the hip should be fixed before retrograde nailing the femur (Level V evidence). For displaced femoral neck fractures, the femur should be fixed before reducing and fixing the hip fracture (Level V evidence).
Do Cephalomedullary Nails Provide Improved Fixation?
Cephalomedullary nails have been advocated by some authors because they provide added fixation of the hip fracture.6 However, recent case series suggest that the clinical results of this type of fixation are inferior to those provided by a retrograde nail for ipsilateral hip and femoral shaft fractures (see Table 58-2).6,19 These case series have small sample sizes, and no trials directly compare these two types of implants for this injury pattern. Watson and Moed9 found a high rate of complications with the use of cephalomedullary nails, and therefore conclude that this implant should not be used with this fracture pattern (Level IV evidence).
TABLE 58-2 Summary of Recommendations for the Treatment of Ipsilateral Hip and Femoral Shaft Fractures
| RECOMMENDATIONS | LEVEL OF EVIDENCE/GRADE OF RECOMMENDATION |
|---|---|
No large comparative studies have been conducted to critically examine the implants used to treat this injury pattern. Based on limited case series and expert opinion, we make the following recommendations (Table 55A-2):
1 Alho A. Concurrent ipsilateral fractures of the hip and shaft of the femur. A systematic review of 722 cases. Ann Chir Gynaecol. 1997;86:326-336.
2 Alho A. Concurrent ipsilateral fractures of the hip and femoral shaft: A meta-analysis of 659 cases. Acta Orthop Scand. 1996;67:19-28.
3 Schatzker J, Barrington TW. Fractures of the femoral neck associated with fractures of the same femoral shaft. Can J Surg. 1968;11:297-305.
4 Swiontkowski MF, Hansen ST, Kellam J. Ipsilateral fractures of the femoral neck and shaft. A treatment protocol. J Bone Joint Surg Am. 1984;66-A:260-268.
5 Wolinsky PR, Johnson KD. Ipsilateral femoral neck and shaft fractures. Clin Orthop Relat Res.; 318; 1995; 81-90.
6 Jain P, Maini L, Mishra P, et al. Cephalomedullary interlocked nail for ipsilateral hip and femoral shaft fractures. Injury. 2004;35:1031-1038.
7 Swiontkowski MF. Ipsilateral femoral shaft and hip fractures. Orthop Clin North Am. 1987;18:73-84.
8 Peljovich AE, Patterson BM. Ipsilateral femoral neck and shaft fractures. J Am Acad Orthop Surg. 1998;6:106-113.
9 Watson JT, Moed BR. Ipsilateral femoral neck and shaft fractures: Complications and their treatment. Clin Orthop Relat Res.; 399; 2002; 78-86.
10 Shuler TE, Gruen GS, DiTano O, Riemer BL. Ipsilateral proximal and shaft femoral fractures: Spectrum of injury involving the femoral neck. Injury. 1997;28:293-297.
11 Winquist RA, Hansen ST. Comminuted fractures of the femoral shaft treated by intramedullary nailing. Orthop Clin North Am. 1980;11:633-648.
12 Damany DS, Parker MJ, Chojnowski A. Complications after intracapsular hip fractures in young adults. A meta-analysis of 18 published studies involving 564 fractures. Injury. 2005;36:131-141.
13 Tornetta P3rd, Kain MS, Creevy WR. Diagnosis of femoral neck fractures in patients with a femoral shaft fracture. Improvement with a standard protocol. J Bone Joint Surg Am. 2007;89-A:39-43.
14 Upadhyay A, Jain P, Mishra P, et al. Delayed internal fixation of fractures of the neck of the femur in young adults. A prospective, randomised study comparing closed and open reduction. J Bone Joint Surg Br. 2004;86-B:1035-1040.
15 Asnis SE, Wanek-Sgaglione L. Intracapsular fractures of the femoral neck: Results of cannulated screw fixation. J Bone Joint Surg Am. 1994;76-A:1793-1803.
16 Chua D, Jaglal SB, Schatzker J. Predictors of early failure of fixation in the treatment of displaced subcapital hip fractures. J Orthop Trauma. 1998;12:230-234.
17 Ricci WM, Bellabarba C, Evanoff B, et al. Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma. 2001;15:161-169.
18 Oh CW, Oh JK, Park BC, et al. Retrograde nailing with subsequent screw fixation for ipsilateral femoral shaft and neck fractures. Arch Orthop Trauma Surg. 2006;126:448-453.
19 Hossam ElShafie M, Adel Morsey H, Emad Eid Y. Ipsilateral fracture of the femoral neck and shaft, treatment by reconstruction interlocking nail. Arch Orthop Trauma Surg. 2001;121:71-74.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
Chapter 58 Combined Fractures of the Hip and Femoral Shaft: What Is the Best Treatment Method?
Ipsilateral fractures of the hip and femur are rare injuries that result from high-energy trauma. This injury pattern is most commonly seen in motor vehicle accidents.1,2 The mechanism of injury is an axial force applied along the femur as the occupant’s knee strikes the dashboard. If the hip is adducted when this force is applied, the resulting injury to the hip is usually a dislocation or acetabular fracture, or both. If the hip is in abduction, this will produce a femoral neck and shaft fracture.3 Given the rarity of this injury (i.e., occurring in less than 9% of all femoral shaft fractures), no large series are reported in the literature.1,2, 4 Nearly 60 different implant combinations have been described for this fracture pattern.5,6
OPTIONS
The main complications associated with isolated femoral neck fractures are high rates of nonunion and avascular necrosis of the femoral head. Complications associated with isolated femoral shaft fractures include malunion (i.e., >2 cm shortening, >10-degree varus or valgus alignment, and >20 degrees malrotation) and nonunion. Many authors contend that the complications of the femoral neck trump those of the femoral shaft. They suggest that avascular necrosis is the most significant complication and, therefore, the femoral neck fracture should be treated first.4,7, 8 Others suggest that the femur should be treated initially to allow for ease of closed reduction of the femoral neck fracture.3,5, 9 What are the most common complications of this injury pattern? In what order should fixation of the fractures proceed?
A large number of the femoral neck fractures associated with shaft fractures are missed (approximately 30%).1 Many of the femoral neck fractures are nondisplaced at the time of presentation (25–60%).1 (This may occur because some of the energy that would normally result in a displaced femoral neck fracture is dissipated by the shaft fracture.) In addition, many of these patients have multiple injuries with numerous “distracting” injuries. What is the best method of imaging the hip to avoid missing a fracture?
A spectrum of different hip fractures has been reported with this injury pattern. Hip fractures vary from intertrochanteric fractures to different types of intracapsular neck fractures. The position of the hip (degree of abduction) at the time of injury has been suggested as the determinant of the pattern of hip fracture produced.10 What is the most common type of hip fracture encountered with this injury? What is the most common type of femoral shaft fracture?
Many different implants and implant combinations have been used to treat this combination of fractures. Implant designs have changed over the time periods of many of the retrospective case series reported in the literature (Table 58-1). For example, the antegrade femoral intramedullary nail has evolved from the unlocked (Küntscher) nail, to the first-generation locked nail, to the second-generation cephalomedullary (or reconstruction) locked nail, and finally to the intramedullary hip screw device. Retrograde femoral nailing has also become increasingly popular since the late 1990s. However, the literature consists of small case series that involve a mixture of different implants from different periods. What are the optimal implants for this fracture pattern?
EVIDENCE
Alho1 conducted a meta-analysis on 65 studies published between 1970 and 1996 that incorporated 722 cases of ipsilateral hip and shaft fractures. This represents the largest summary of case series reported in the literature. He identified 10 studies (240 fractures) that included useful demographic data. This injury typically occurs in young individuals (mean age, 33 years) and results from a high-energy mechanism (85% motor vehicle accidents). Only 1% of cases occurred in elderly individuals. Approximately 18% of the femoral shaft fractures were reported as open, with a large number of comminuted fractures (i.e., 42% were Winquist type III or IV).11 The majority of shaft fractures occurred in the middle third of the femur (72%). For hip fractures, Alho1 reports that the majority of cases were femoral neck fractures (61%), with the rest being trochanteric fractures. Shuler and colleagues10 report on 52 cases of hip fracture with femoral shaft fracture and found 90% to be femoral neck fractures. They found that these hip fractures all tended to extend into the inferomedial neck regardless of the fracture type (i.e., midcervical, basocervical, or pertrochanteric). The extension of the fracture into the inferomedial neck (i.e., femoral calcar) makes it prone to displacement with weight bearing.
Complication rates for femoral neck fractures with an associated femoral shaft fracture tend to be less than with this injury in isolation. Alho1 quotes an avascular necrosis rate of 5% and no nonunions of 254 fractures (this includes displaced and nondisplaced fractures). For isolated displaced femoral neck fractures, the incidence rate of avascular necrosis is 22.5% and of nonunion is 6%.12 The reduced rate of avascular necrosis and nonunion seen with the combined injury may result from a greater rate of nondisplaced fractures (up to 60% for the combined injury),1 perhaps because much of the energy is dissipated through the femoral shaft fracture. Thus, the hip fracture tends to be less comminuted with less injury to the vasculature (i.e., posterior retinacular vessels).
An important consequence of the high rate of nondisplaced femoral neck fractures is that they tend to be missed on initial presentation. Alho1 states that the diagnosis of the hip fracture was delayed (from 1 day to several months) in 30% of cases. Tornetta and investigators13
[/not-level-membership-for-orthopaedics-category]
