[level-membership-for-plastic-reconstructive-surgery-category]
Chapter 11 Combined abdominoplasty and breast enlargement by autologous tissue transfer or transabdominal implant placement
A Augmentation Mammaplasty by Reverse Abdominoplasty
Key Points
• Augmentation mammaplasty by reverse abdominoplasty (AMBRA) may be a viable option for patients with upper abdominal skin laxity and adiposity who desire autologous tissue breast augmentation and/or mastopexy combined with reverse abdominoplasty.
• Patients with epigastric or subcostal incisional scars that exclude them as candidates for conventional abdominoplasty, can safely undergo AMBRA.
Introduction
Relative to conventional abdominoplasty, reverse abdominoplasty has been less frequently studied.1–4 This is in part due to the fact that the reverse abdominoplasty technique necessitates an upper abdominal scar, and that most patients present with lower, rather than upper, abdominal laxity. In patients with relatively normal infraumbilical abdomen tissues who request that the lax epigastric tissues be addressed, or patients who are not candidates for conventional abdominoplasty because of previous subcostal incisional scars, reverse abdominoplasty may be the safer, better, or sole option.5
Preoperative Planning/Patient Selection
The key steps in determining a patient’s suitability for the AMBRA procedure are a careful evaluation of the soft tissues of the upper epigastrum and performing a “breast suspension” test (Fig. 11.1). The patient is asked to lift each breast with a cupped hand. This should restore an esthetic result to the upper abdomen and umbilicus. Some patients benefit from suction-assisted lipectomy to the lower abdomen for contouring. Other patients would be better served by a mini-abdominoplasty to address moderate skin laxity of the lower abdomen. These adjuncts can help optimize the final result of AMBRA, without undue added risk.


Surgical Technique
These preoperative markings are conducted while the patient is standing upright, to delineate the inframammary folds, and breast markings for mastopexy are performed concurrently. Then the patient is placed supine to allow the surgeon to retract the excess upper abdominal tissues cephalad, which is an adaptation of the Lockwood technique.6 The redundant soft tissues of the upper abdomen are then folded over to mark the “safe” zone of skin excision that permits tension-free closure with the inframammary fold. This area can be de-epithelialized without sacrificing a tension-free closure of the upper abdominal–IMF wound (Fig. 11.2). This de-epithelialized tissue provides the bulk for each breast’s augmentation.

Superiorly Based Augmentation Mammaplasty by Reverse Abdominoplasty
The patient is returned to a fully supine position, and with cephalic tension on the flap, the de-epithelialized border of the skin apron is anchored to the perichondrium, periosteum, and deep fascia along the lower border of the breast. A nipple–areola complex located slightly lower on the breast mound (1 to 2 cm) than ideal, to allow for lower pole descent, is preferred. The edge of the abdominal skin flap is then reinforced along its entire length with sutures to the periosteum. The central midline supraumbilical abdominal area is then liposuctioned to emphasize the median raphe. The closure of upper and lower wounds is the same except that Scarpa’s fascia is approximated in the lower abdominal closure, followed by dermal closure (Box 11.1).
Box 11.1
Optimizing outcomes pearls
1. AMBRA is a forgiving technique, if the surgeon preserves the dominant central abdominal perforators and avoids venous and lymphatic compromise.
2. In patients undergoing AMBRA with concomitant lower abdominal adiposity, a mini-abdominoplasty or panniculectomy can treat persistent lower abdominal skin and tissue redundancy without compromising central abdominal vascularity.
Peri- and Postoperative Care
Case Examples
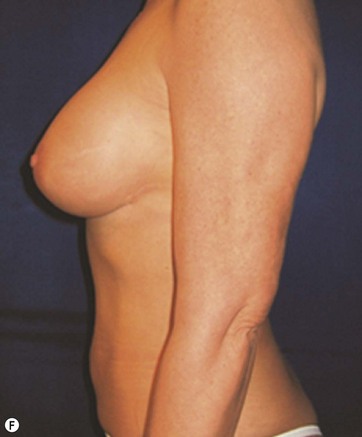
A 70-year-old patient desired fuller breasts and superior and central abdominal tightening (Fig. 11.3A, B, C, D).




The case example shown in Fig. 11.4 depicts a patient who had previous submuscular breast augmentation and was unhappy with her sagging epigastric soft tissues and breast appearance.





Complications and Their Management
Versus conventional abdominoplasty, the AMBRA scar is more difficult to conceal, but the normal venous, lymphatic and periumbilical arterial inflow to the flap are preserved. Moon and Taylor’s description of the periumbilical perforator network spurred the evolution of modern microsurgical breast reconstruction.7 Thus, the reverse abdominoplasty technique is forgiving, if the surgeon preserves the dominant central abdominal perforators and avoids venous and lymphatic compromise.
There is no risk for capsular contracture or other device-related problems with the AMBRA technique, and it provides a natural-feeling breast. Other techniques for autologous breast have been suggested to provide these same benefits versus synthetic implants.8–13 However, augmentation mammaplasty by reverse abdominoplasty also provides concurrent abdominal contouring. The result can make for a dramatic improvement in selected patients. Admittedly, the AMBRA technique requires more operative time than its implant-based version. A major disadvantage of AMBRA is the required transverse epigastric scar, which encompasses both inframammary creases and crosses the midline in the presternal region. This scar has been surprisingly well tolerated by our patients, who might not otherwise be abdominoplasty candidates.
B Transabdominal Breast Augmentation
Introduction
A desire for combined cosmetic procedures, particularly the so-called “mommy makeover” has increased interest in perfecting techniques that safely and reliably result in a pleasing esthetic outcome. In our experience, in an appropriately selected patient population, we have frequently utilized the transabdominal breast augmentation (TABA) in the pursuit of these goals. Though TABA has been described before, these published reports have been limited by short-term follow up and small case series. In addition, the majority of these surgeons utilized general anesthesia, which differs from our experience. Often those patients who desire abdominoplasty are seldom nulliparous and have concomitant involutional breast volume loss and either resultant ptosis or pseudoptosis. These patients often request accompanying breast augmentation and we believe the combined procedure of breast augmentation via an abdominoplasty incision is a favorable approach in terms of minimizing incisions and can be safely performed without general anesthesia, thereby limiting postoperative nausea and vomiting.14–18 The senior surgeon, R.J.Z., has the largest series to date of this technique and his procedure and management are illustrated here and elsewhere.19
Surgical Technique
A conventional abdominoplasty flap dissection is performed. Tunnels are created to reach the inframammary fold, at which point blunt finger dissection is used to create a subpectoral pocket. The pocket is further defined using a Snowden Pencer™ balloon dissector (Fig. 11.5). A hockey stick dissector is frequently used for further pocket definition.

The patient shown in Fig. 11.6 demonstrates significant preoperative rectus diastasis after two large pregnancies. The patient in Fig. 11.7 underwent a floating abdominal technique; note her involutional loss of breast volume preoperatively.




The patient shown in Fig. 11.8 had significant preoperative lower abdominal adiposity which is improved significantly after TABA with a pleasing feminine hourglass shape.


Box 11.2 gives hints for optimizing outcomes.
1 Baroudi R, Keppke EM, Carvalho CG. Mammary reduction combined with reverse abdominoplasty. Ann Plast Surg. 1979;2:368–373.
2 Berrino P, Campora E, Leone S, et al. Correction of type II breast deformities following conservative cancer surgery. Plast Reconstr Surg. 1992;90:846–853.
3 Dagregorio G, Darsonval V. Aesthetic surgery techniques after excision of dermatofibrosarcoma protuberans: A case report. Br J Plast Surg. 2005;58:556–560.
4 Hurwitz DJ, Agha-Mohammadi S. Postbariatric surgery breast shaping the spiral flap. Ann Plast Surg. 2006;56:481–486.
5 Zienowicz RJ, Karacaoglu E. Augmentation mammaplasty by reverse abdominoplasty (AMBRA). Plast Reconstr Surg. 2009;124(5):1662–1672.
6 Lockwood T. Reduction mammaplasty and mastopexy with superficial fascial suspension. Plast Reconstr Surg. 1999;103:1411–1420.
7 Moon HK, Taylor GI. The vascular anatomy of rectus abdominis musculocutaneous flaps based on the deep superior epigastric system. Plast Reconstr Surg. 1988;2:815–832.
8 Lai YL, Yu YL, Centeno RF, et al. Breast augmentation with bilateral de-epithelialized TRAM flaps: An alternative approach to breast augmentation with autologous tissue. Plast Reconstr Surg. 2003;112:302–308. discussion 309–11
9 Landuyt KL, Hamdi M, Blondeel P, et al. Autologous breast augmentation by pedicled perforator flaps. Ann Plast Surg. 2004;53:322–327.
10 Kwei S, Borud LJ, Lee BT. Mastopexy with augmentation after massive weight loss. Ann Plast Surg. 2006;57:361–365.
11 Hamdi M, Landuyt KV, Frene BD, et al. The versatility of the inter-costal artery perforator (ICAP) flaps. J Plast Recontstr Aesth Surg. 2006;59:644–652.
12 Pulagam SR, Poulton T, Mamounas EP. Long-term clinical and radiologic results with autologous fat transplantation for breast augmentation: Case reports and review of the literature. Breast J. 2006;12:63–65.
13 Zenn MR, Heitmann C. Extended TRAM flap: Feasibility study on fresh human cadavers. Ann Plast Surg. 2003;50:256–262.
14 Hinderer UT. The dermolipectomy approach for augmentation mammaplasty. Clin Plast Surg. 1975;2:359–369.
15 Planas J. Introduction of breast implants through the abdominal route. Plast Reconstr Surg. 1976;57:431–437.
16 Barrett BM, Kelly RV. Combined abdominoplasty and augmentation mammaplasty through a transverse suprapubic incision. Ann Plast Surg. 1980;4:286–291.
17 Wallach SG. Maximizing the use of the abdominoplasty incision. Plast Reconstr Surg. 2004;113:411–417.
18 Rinker B, Jack JM. Subpectoral breast augmentation through the abdominoplasty incision. Ann Plast Surg. 2007;58:241–245.
19 Bhatt RA, Sullivan R, Zienowicz RJ. Transabdominal breast augmentation (TABA). Submitted for publication.
[/level-membership-for-plastic-reconstructive-surgery-category][not-level-membership-for-plastic-reconstructive-surgery-category]
Chapter 11 Combined abdominoplasty and breast enlargement by autologous tissue transfer or transabdominal implant placement
A Augmentation Mammaplasty by Reverse Abdominoplasty
Key Points
• Augmentation mammaplasty by reverse abdominoplasty (AMBRA) may be a viable option for patients with upper abdominal skin laxity and adiposity who desire autologous tissue breast augmentation and/or mastopexy combined with reverse abdominoplasty.
• Patients with epigastric or subcostal incisional scars that exclude them as candidates for conventional abdominoplasty, can safely undergo AMBRA.
Introduction
Relative to conventional abdominoplasty, reverse abdominoplasty has been less frequently studied.1–4 This is in part due to the fact that the reverse abdominoplasty technique necessitates an upper abdominal scar, and that most patients present with lower, rather than upper, abdominal laxity. In patients with relatively normal infraumbilical abdomen tissues who request that the lax epigastric tissues be addressed, or patients who are not candidates for conventional abdominoplasty because of previous subcostal incisional scars, reverse abdominoplasty may be the safer, better, or sole option.5
Preoperative Planning/Patient Selection
The key steps in determining a patient’s suitability for the AMBRA procedure are a careful evaluation of the soft tissues of the upper epigastrum and performing a “breast suspension” test (Fig. 11.1). The patient is asked to lift each breast with a cupped hand. This should restore an esthetic result to the upper abdomen and umbilicus. Some patients benefit from suction-assisted lipectomy to the lower abdomen for contouring. Other patients would be better served by a mini-abdominoplasty to address moderate skin laxity of the lower abdomen. These adjuncts can help optimize the final result of AMBRA, without undue added risk.
Surgical Technique
These preoperative markings are conducted while the patient is standing upright, to delineate the inframammary folds, and breast markings for mastopexy are performed concurrently. Then the patient is placed supine to allow the surgeon to retract the excess upper abdominal tissues cephalad, which is an adaptation of the Lockwood technique.6 The redundant soft tissues of the upper abdomen are then folded over to mark the “safe” zone of skin excision that permits tension-free closure with the inframammary fold. This area can be de-epithelialized without sacrificing a tension-free closure of the upper abdominal–IMF wound (Fig. 11.2). This de-epithelialized tissue provides the bulk for each breast’s augmentation.
Superiorly Based Augmentation Mammaplasty by Reverse Abdominoplasty
The patient is returned to a fully supine position, and with cephalic tension on the flap, the de-epithelialized border of the skin apron is anchored to the perichondrium, periosteum, and deep fascia along the lower border of the breast. A nipple–areola complex located slightly lower on the breast mound (1 to 2 cm) than ideal, to allow for lower pole descent, is preferred. The edge of the abdominal skin flap is then reinforced along its entire length with sutures to the periosteum. The central midline supraumbilical abdominal area is then liposuctioned to emphasize the median raphe. The closure of upper and lower wounds is the same except that Scarpa’s fascia is approximated in the lower abdominal closure, followed by dermal closure (Box 11.1).
Box 11.1
Optimizing outcomes pearls
1. AMBRA is a forgiving technique, if the surgeon preserves the dominant central abdominal perforators and avoids venous and lymphatic compromise.
2. In patients undergoing AMBRA with concomitant lower abdominal adiposity, a mini-abdominoplasty or panniculectomy can treat persistent lower abdominal skin and tissue redundancy without compromising central abdominal vascularity.
