31 Combination Cosmetic Treatments
Facial aging is a complex process of static and dynamic wrinkling, loss of soft tissue volume with formation of folds and contour defects, and vascular and dyschromic changes. Addressing these different issues often requires the use of multiple aesthetic procedures. Many of the minimally invasive aesthetic procedures in use today are complementary, and may be combined to achieve optimal treatment outcomes and high patient satisfaction.1,2
Treatments typically combined with one another include botulinum toxin, dermal fillers, lasers and intense pulsed light (collectively referred to as lasers* in this chapter), microdermabrasion, chemical peels, and skin care products.3 These procedures can be incorporated into treatment plans over several visits, or some may be combined on the same day in multimodality visits. This chapter demonstrates common treatment combinations of procedures discussed in the aesthetic section of this book.
Botulinum Toxin and Dermal Fillers
Wrinkles (also called rhytids) usually have both a dynamic and a static component. In many regions of the face, enhanced rhytid reduction can be achieved by addressing both dynamic muscle contraction with botulinum toxin and static lines and volume loss with dermal fillers.4,5 Botulinum toxin is commonly used in the upper face6 and may be combined with dermal filler treatments, particularly in the glabellar frown area (Figure 31-1).7–9
Botulinum toxin may also be combined with dermal fillers in the lower face, which is a more advanced application for botulinum toxin. Figure 31-2 shows a patient (the author) with radial upper lip lines elicited with active contraction of the orbicularis oris muscle (A) before, (B) 2 weeks after treatment with botulinum toxin, followed by dermal filler treatment 2 weeks later (C). Figure 31-3 shows a patient with volume loss in the oral commissure and marionette line areas, with downturned corners of the mouth, (A) before and (B) after treatment with dermal filler in these areas and botulinum toxin in the depressor anguli oris muscle which were performed in the same visit.

Dermal filler and botulinum toxin combination treatments may be performed on separate days or during the same visit. If performed on separate days, it is recommended that treatment with botulinum toxin be performed first, a few weeks prior to dermal filler treatment, to reduce muscular activity in the treatment area and allow for evaluation of the static appearance of the treatment area. If performed on the same day, the botulinum toxin injection should be performed last, to reduce tissue distortion that may occur from swelling with botulinum toxin injections. If excessive edema is present after dermal filler treatment it is advisable to postpone, botulinum toxin injection and perform treatment 1 week later.2
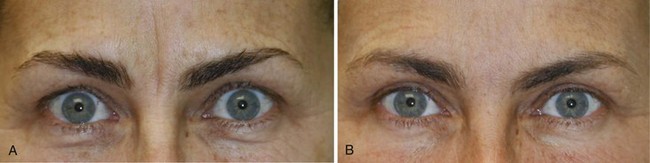
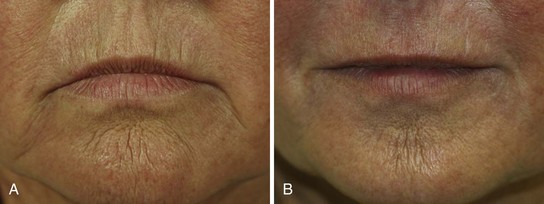
Figure 31-4 shows a patient (A) before and (B) after treatment with dermal fillers and botulinum toxin to several facial areas. Upper lip radial lip lines were treated using dermal filler and botulinum toxin, and crow’s feet and glabellar complex muscles were treated using botulinum toxin. She demonstrates a typical softened appearance overall after treatment (Figure 31-4B) that is very natural looking and is the desired goal of combination aesthetic treatments.

Botulinum Toxin and Skin Resurfacing
Skin resurfacing is a global, full-face treatment that can address rhytids and irregular texture, as well as dyschromia. Methods of resurfacing range from mild treatments with superficial chemical peels and/or microdermabrasion, to nonablative fractional laser treatments (e.g., 1550 nm) to more aggressive fractional ablative laser resurfacing (e.g., 2940 nm). Botulinum toxin treatments are often performed on the same day, following mild resurfacing treatments,10,11 and are usually performed at least 1 week prior to laser resurfacing.
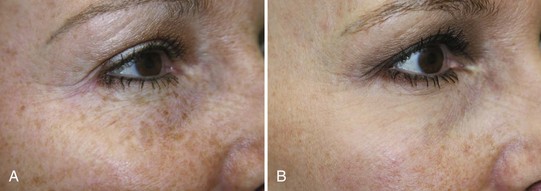
The periocular area is a common region for combination therapy with botulinum toxin and laser resurfacing.12,13 Figure 31-5 shows a patient (A) before and (B) after receiving botulinum toxin to the crow’s feet muscles and ablative laser resurfacing, demonstrating reduction of crow’s feet lines and dyschromia.
In addition, different methods of superficial skin resurfacing can be combined in the same visit for enhanced results. For example, microdermabrasion, which removes the stratum corneum barrier, may immediately precede chemical peel application in the same visit to allow for more even and deeper acid penetration into the skin.14
Combining Treatments with Lasers
Nonablative laser treatments for dyschromia (e.g., IPL and 532 nm lasers) may also be combined with superficial skin resurfacing procedures.15 Following laser treatment of pigmented lesions, such as lentigines, there is microcrust formation and clinical darkening of the lesions. Resolution of these darkened lesions occurs spontaneously through exfoliation. However, improvements can be achieved more rapidly by combining superficial skin resurfacing using microdermabrasion at least 2 weeks after laser treatments for dyschromia.
When treating dyschromia, it can be useful to combine nonablative lasers that target pigmentation at different depths in the skin. Figure 31-6 shows a patient with dyschromia (A) prior to and (B) after three IPL treatments, which can target deeper pigmented lesions (based on the settings used), followed by treatment with a Q-switched 532 nm laser, which targets very superficial pigment in the skin.

Advanced facial aging changes include moderate to severe dyschromia and rhytids. These changes can be addressed by combining the more aggressive ablative resurfacing lasers (e.g., erbium and carbon dioxide lasers) for rhytid reduction with nonablative lasers that target pigmentation. Figure 31-7 shows a patient (A) before and (B) after IPL treatment for dyschromia, followed by fractional ablative laser resurfacing for textural improvement in severely photodamaged skin.

1. Small R. Aesthetic procedures introduction. In: Mayeaux E, editor. The Essential Guide to Primary Care Procedures. Philadelphia: Lippincott Williams & Wilkins; 2009:195-199.
2. Fedok FG. Advances in minimally invasive facial rejuvenation. Curr Opin Otolaryngol Head Neck Surg. 2008;16(4):359-368.
3. Small R. Aesthetic procedures in office practice. Am Fam Physician. 2009;80(11):1231-1237.
4. Carruthers JD, Glogau RG, Blitzer A. Advances in facial rejuvenation: botulinum toxin type A, hyaluronic acid dermal fillers, and combination therapies—consensus recommendations. Plast Reconstr Surg. 2008;121(5 Suppl):5S-30S.
5. Coleman KR, Carruthers J. Combination therapy with Botox and fillers: the new rejuvenation paradigm. Dermatol Ther. 2006;19(3):177-188.
6. Small R. Botulinum toxin type A for facial rejuvenation. In: Mayeaux E, editor. The Essential Guide to Primary Care Procedures. Philadelphia: Lippincott Williams & Wilkins; 2009:200-213.
7. Carruthers JD, Carruthers A. A prospective, randomized, parallel group study analyzing the effect of BTX-A (Botox) and nonanimal sourced hyaluronic acid (NASHA, Restylane) in combination compared with NASHA (Restylane) alone in severe glabellar rhytides in adult female subjects: treatment of severe glabellar rhytides with a hyaluronic acid derivative compared with the derivative and BTX-A. Dermatol Surg. 2003;29(8):802-809.
8. Carruthers J, Carruthers A, Maberley D. Deep resting glabellar rhytides respond to BTX-A and Hylan B. Dermatol Surg. 2003;29(5):539-544.
9. Maas CS. Botulinum neurotoxins and injectable fillers: minimally invasive management of the aging upper face. Facial Plast Surg Clin North Am. 2006;14(3):241-245.
10. Rendon MI, Effron C, Edison BL. The use of fillers and botulinum toxin type A in combination with superficial glycolic acid (alpha-hydroxy acid) peels: optimizing injection therapy with the skin-smoothing properties of peels. Cutis. 2007;79(1 Suppl Combining):9-12.
11. Small R. Microdermabrasion. In: Mayeaux E, editor. The Essential Guide to Primary Care Procedures. Philadelphia: Lippincott Williams & Wilkins; 2009:265-277.
12. Yamauchi PS, Lask GP, Lowe NJ. Botulinum toxin type A gives adjunctive benefit to periorbital laser resurfacing. J Cosmet Laser Ther. 2004;6(3):145-148.
13. Zimbler MS, Holds JB, Kokoska MS, et al. Effect of botulinum toxin pretreatment on laser resurfacing results: a prospective, randomized, blinded trial. Arch Facial Plast Surg. 2001;3(3):165-169.
14. Briden ME, Jacobsen E, Johnson C. Combining superficial glycolic acid (alpha-hydroxy acid) peels with microdermabrasion to maximize treatment results and patient satisfaction. Cutis. 2007;79(1 Suppl Combining):13-16.
15. Effron C, Briden ME, Green BA. Enhancing cosmetic outcomes by combining superficial glycolic acid (alpha-hydroxy acid) peels with nonablative lasers, intense pulsed light, and trichloroacetic acid peels. Cutis. 2007;79(1 Suppl Combining):4-8.
Small R, Hoang D. Botulinum toxin introduction and foundation concepts. In: Small R, Hoang D, editors. A Practical Guide to Botulinum Toxin Procedures. Philadelphia: Lippincott Williams & Wilkins, 2011.
Small R, Hoang D. Dermal filler introduction and foundation concepts. In: Small R, Hoang D, editors. A Practical Guide to Dermal Filler Procedures. Philadelphia: Lippincott Williams & Wilkins, 2011.
Small R, Linder J. Combining therapies. In: Small R, Linder J, editors. A Practical Guide to Skin Care Procedures and Products. Philadelphia: Lippincott Williams & Wilkins, 2011.
Small R. Combining therapies. In: Small R, editor. A Practical Guide to Cosmetic Lasers. Philadelphia: Lippincott Williams & Wilkins, 2012.






