Short, focal, “apple core” lesion < 10 cm in length
More likely to cause colonic obstruction than submucosal lymphoma or mets
• Colonic Kaposi sarcoma
• Ileocolic tuberculosis
• Gastrointestinal stromal tumor
PATHOLOGY
• Metastatic spread from melanoma or primary tumor of stomach, lung, or breast (rarely, other cancers)
Gastric cancer may directly invade transverse colon along gastrocolic ligament
• Lymphoma may arise from and be limited to colon
CLINICAL ISSUES
• Most common signs/symptoms: Rectal bleeding, symptoms of obstruction, especially if intussusception is present
• 50% 5-year survival rate for patients with primary colonic lymphoma
• Prognosis is poor for patients with metastases to colon from melanoma, breast, lung, or gastric cancer
DIAGNOSTIC CHECKLIST
• Consider lymphoma for bulky mass with aneurysmal dilatation of lumen and no colonic obstruction
• “Serrated” edge of transverse colon (on barium enema) may indicate gastric cancer invading gastrocolic ligament
(Left) Axial CECT in a 67-year-old man presenting with 3 months of intermittent rectal bleeding and clinical symptoms of obstipation shows a bulky enhancing mass involving the rectosigmoid colon, with no evidence of colonic obstruction.
(Right) Axial CECT in the same patient reveals an enhancing perirectal nodal metastasis . The patient had a subsequent endoscopic biopsy of the mass, which identified a non-Hodgkin lymphoma.
(Left) Axial CECT in a 71-year-old man with known lung carcinoma presenting with LLQ pain and a palpable mass demonstrates a large heterogeneously enhancing mass involving the descending colon . This was a colonic metastasis.
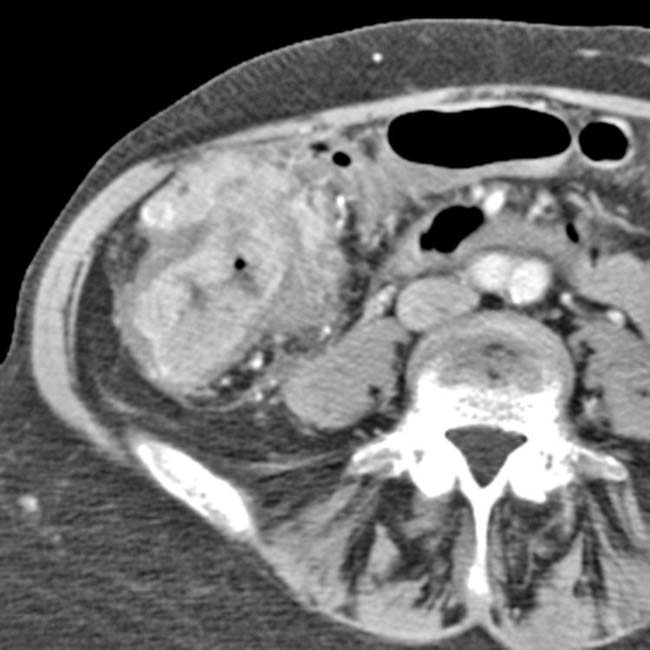
(Right) Axial CECT in a 68-year-old man with weight loss and RLQ pain demonstrates a bulky ileocecal mass with smooth margins . Note the oral contrast filling the lumen of the cecum , indicating the lack of obstruction. Endoscopic biopsy revealed a high-grade B-cell lymphoma.
Axial CECT in a 55-year-old male presenting with RLQ pain and a palpable mass demonstrates a hypervascular mass intussuscepting into the ascending colon.
Coronal CECT in the same patient again illustrates the intussuscepting mass. This patient underwent surgery, which revealed the mass to be a B-cell non-Hodgkin lymphoma.





 involving the rectosigmoid colon, with no evidence of colonic obstruction.
involving the rectosigmoid colon, with no evidence of colonic obstruction.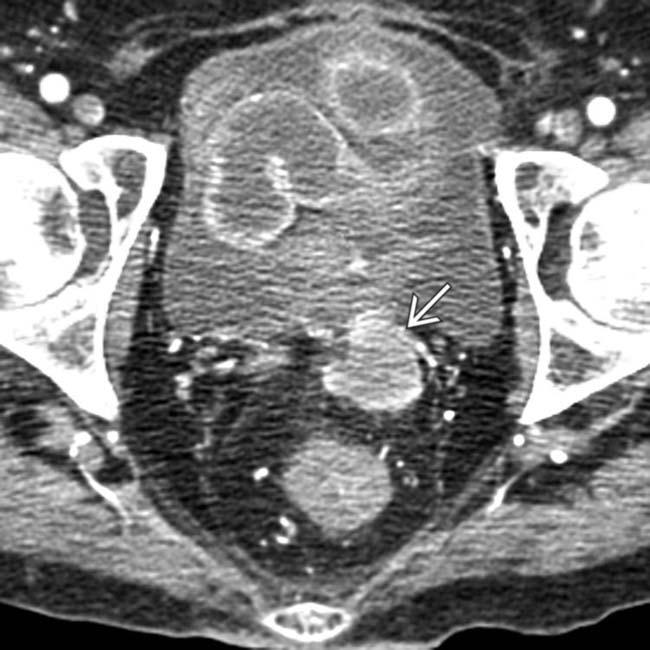
 . The patient had a subsequent endoscopic biopsy of the mass, which identified a non-Hodgkin lymphoma.
. The patient had a subsequent endoscopic biopsy of the mass, which identified a non-Hodgkin lymphoma.
 . This was a colonic metastasis.
. This was a colonic metastasis.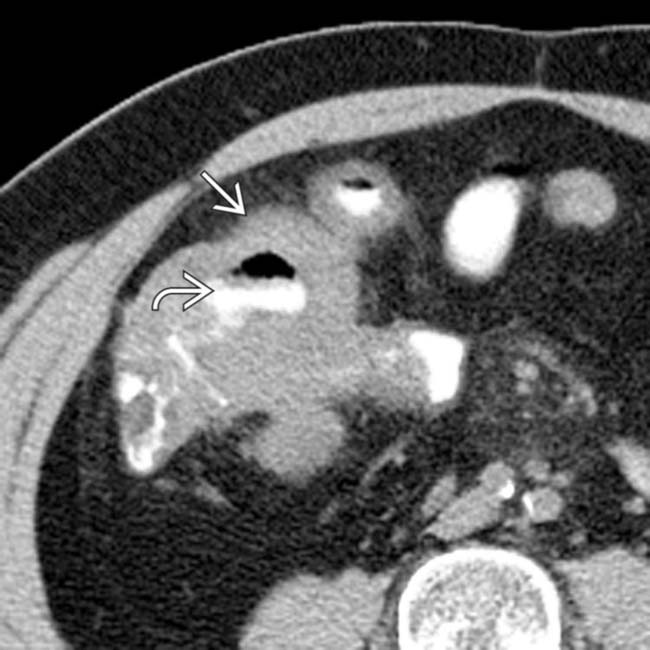
 . Note the oral contrast filling the lumen of the cecum
. Note the oral contrast filling the lumen of the cecum  , indicating the lack of obstruction. Endoscopic biopsy revealed a high-grade B-cell lymphoma.
, indicating the lack of obstruction. Endoscopic biopsy revealed a high-grade B-cell lymphoma.