218 Clubbing
Salient features
History
• Lung conditions (bronchogenic carcinoma; fibrosing alveolitis; mesothelioma; suppurative lung disease such as bronchiectasis, lung abscess and empyema)
• Cardiac conditions (infective endocarditis, cyanotic heart disease)
• GI tract conditions (cirrhosis, ulcerative colitis, Crohn’s disease)
Examination
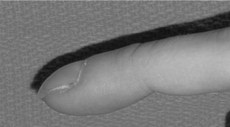
• Increased curvature of the nails, obliteration of the angle of the nail. A positive Schamroth test is the absence of the normal diamond-shaped window created when the dorsal surfaces of the terminal phalanges of similar fingers are opposed (Fig. 218.1). (When in doubt, approximate the dorsal aspects of terminal phalanges of the fingers of both hands flexed at the interphalangeal joints. Normally, the angle between the nails does not extend more than halfway up the nail bed. In clubbing there is a wide and deep angle, Schamroth’s sign.)
• Loss of Lovibond’s angle (Fig. 218.2)
• The nails may have a drumstick appearance (see Fig. 106.1).

• Look for the following signs:
• Palpate the wrist joints for tenderness: hypertrophic pulmonary osteoarthropathy (HPOA); rapid painful clubbing is nearly always caused by bronchogenic carcinoma.
• Tell the examiner that you would like to examine the following systems:
Questions
How is clubbing graded?
I: increased glossiness and cyanosis of the skin at the root of the nail associated with increased fluctuation at the base of the nail bed
II: the normal angle between the base of the nail and the skin is obliterated (Lovibond’s sign) and may even be reversed
III: hypertrophy of the soft tissue of the nail pulp and the nail curves excessively longitudinally to give a ‘drum-stick’ or ‘parrot-beak’ appearance (’doigts Hippocratique’)
IV: bony changes involving the wrists and ankles, sometimes the elbows and knees (HPOA).
Advanced-level questions
What are the mechanisms for clubbing?
• Increased blood flow in clubbed fingers caused by vasodilatation rather than hyperplasia of vessels in the nail bed. The nature of the vasodilator is unclear and many contenders, such as ferritin, bradykinin, prostaglandin and serotonin (5-hydroxytryptamine (5-HT)), have been implicated. The vasodilator is probably inactivated in the lung in normal persons but when this inactivation is defective, or there is a right-to-left shunt, clubbing occurs.
• Increased growth hormone in disease states causes excessive cellular tissue in the nail bed.
• Clubbing occurs whenever organs supplied by the vagus are affected. It has been shown that, in bronchogenic carcinoma, vagotomy causes reversal of clubbing.
• Tumour necrosis factor has been implicated.
• Megakaryocytes and clumps of platelets may preferentially stream into blood vessels of the digits and release platelet-derived growth factor, vascular end growth factor (vascular endothelial growth factor). The resulting increased capillary permeability, fibroblastic activity and arterial smooth muscle hyperplasia could cause clubbing.
Adams F. Hippocrates. The Book of Prognostics. The Genuine Works of Hippocrates, Vol. 1. London: Sydenham Society. 1849.
Burton MD, Wain JC. Clubbing and hypertrophic osteoarthropathy. N Engl J Med. 1993;329:1862. (classical pictures of these conditions)
Dickinson CJ. The aetiology of clubbing and hypertrophic osteopathy. Eur J Clin Invest. 1993;23:330-338.
Schamroth L. Clubbing of fingers: a method of assessment. S Afr Med J. 1976;50:297.





