[level-membership-for-obstetrics-gynecology-category]CHAPTER 95
Closure of a Simple Transmural Injury to the Small Intestine
An injury to the wall of the small intestine incurred during a pelvic dissection can be managed without resorting to an intestinal resection if the blood supply to the bowel segment has not been interrupted. Observation of the intestine will show the bowel to maintain a healthy pink color (Fig. 95–1). Next, the edges of the wound should be trimmed with a fine scissors (Fig. 95–2A, B). The cut edges should bleed to further indicate healthy intestinal tissue. Next, a through-and-through closure utilizing 2-0 or 3-0 chromic catgut is placed as interrupted sutures (Fig. 95–2C). A second imbricating layer of 2-0 interrupted silk is sutured into the muscularis and serosa (Fig. 95–2D through F). The suture line is irrigated and the bowel lumen is checked for adequacy between the surgeon’s thumb and fingers.
Alternatively, contemporary surgical techniques utilize a simple single-layer closure consisting of 2-0 silk sutures. The needle and suture penetrate serosa, muscularis, and mucosa on one side of the defect, and mucosa, muscularis, and serosa on the other. Each extreme is tied first, followed then by the remaining ligatures. The wound is irrigated with normal saline, then the lumen is checked for adequacy (Fig. 95–3A through C).
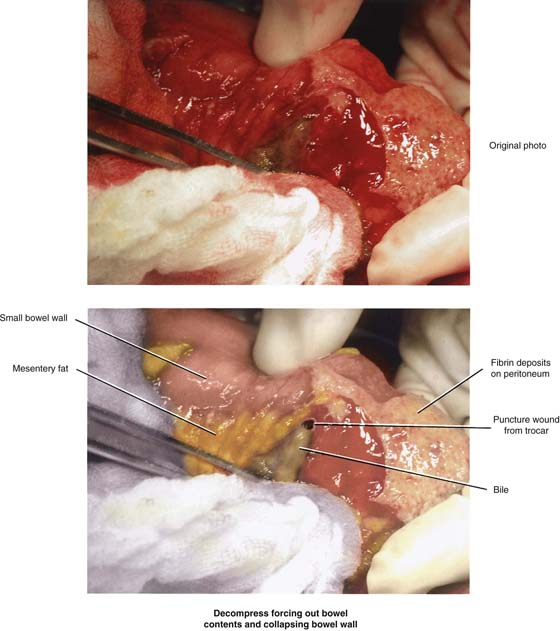
FIGURE 95–1 The original actual photograph shows a bowel perforation just above the mesenteric border of the small intestine. Blood and fibrin are present on the bowel. Above the forceps, bile-stained intestinal contents spill from the wound. Note the bubbles of air. Below, the artist has drawn the same injury for emphasis.
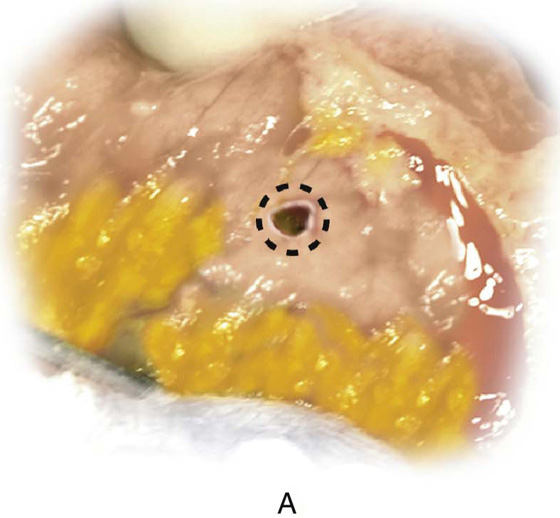
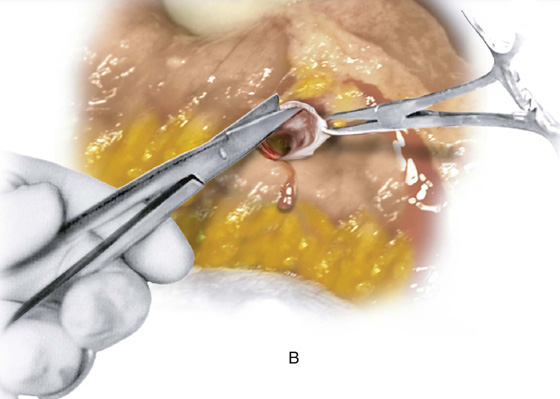
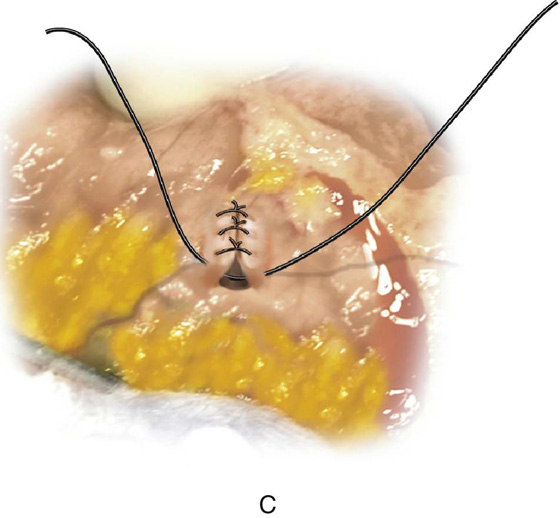
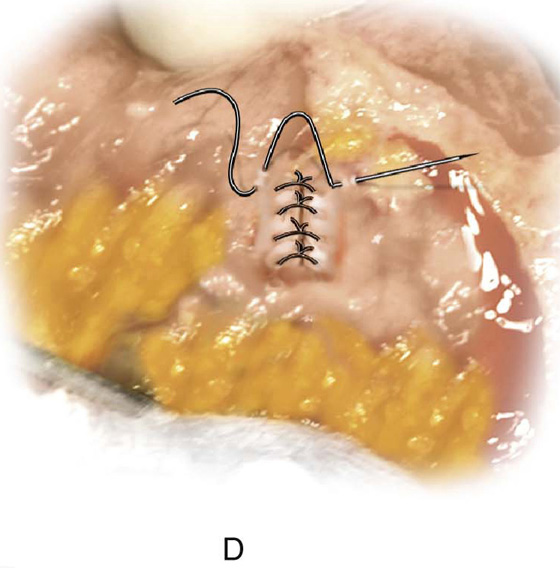
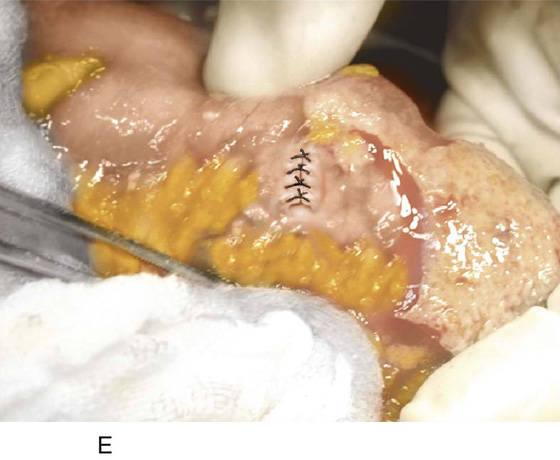
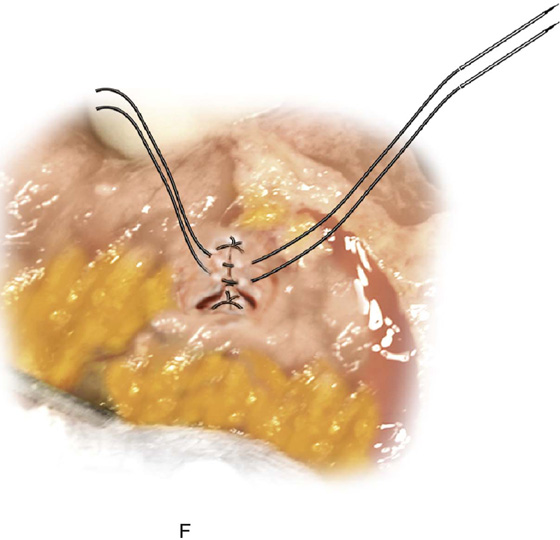
FIGURE 95–2 A. An outline of the portion of intestinal wall to be debrided. B. The surgeon cuts away devitalized tissue around the margin of the perforation. Good blood flow from the incision edges ensures viability. C. Chromic catgut sutures placed through serosa, muscularis, submucosa, and mucosa (through-and-through), and then vice versa in interrupted fashion, close the defect. D. A second layer of 2-0 silk is placed only through the serosa and muscularis via fine intestinal needles. E. The second line of silk sutures covers the first through-and-through layer. F. The wound is completely closed and is strongly sealed.
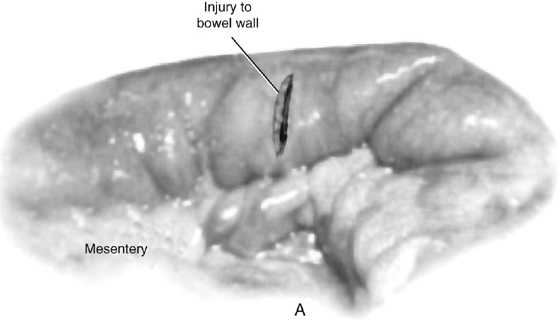
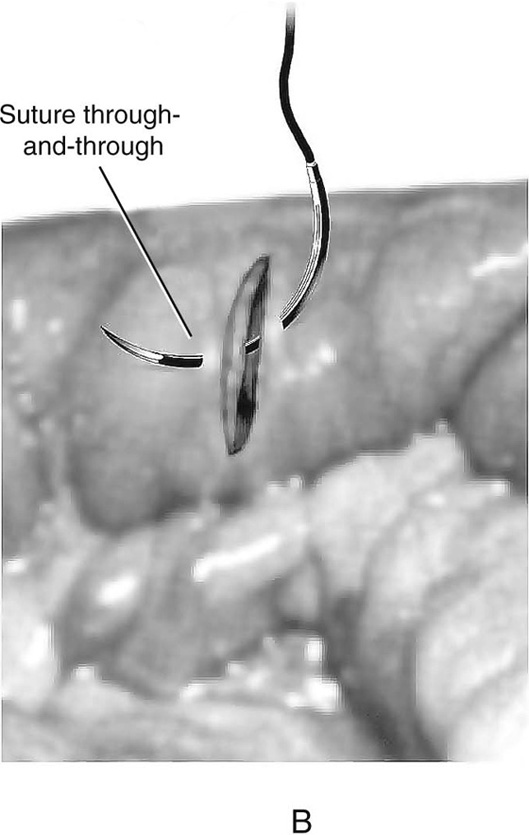
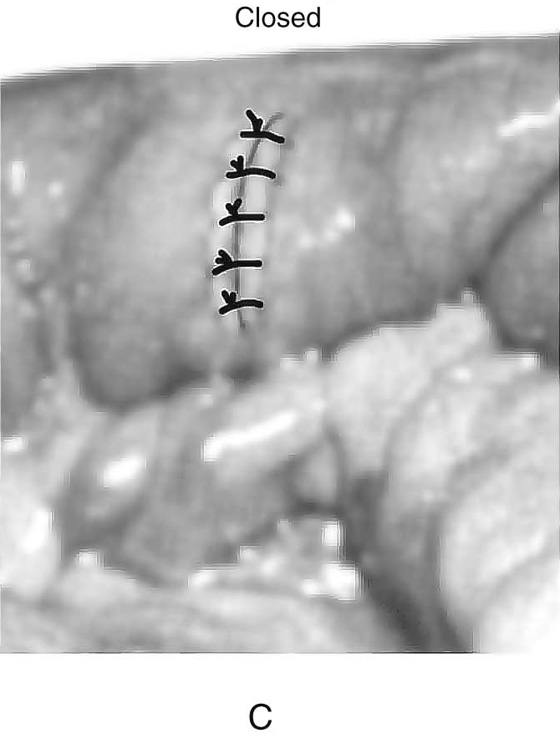
FIGURE 95–3 A. An opening has been made in the small intestine. Investigation reveals that the mucosa has been entered. B. The defect is closed by a series of simple (single-layer) 2-0 silk or polydioxanone (PDS) sutures. C. The completed closure is irrigated and checked for fluid tightness. The lumen is also examined to determine its adequacy.
[/level-membership-for-obstetrics-gynecology-category][not-level-membership-for-obstetrics-gynecology-category]CHAPTER 95
Closure of a Simple Transmural Injury to the Small Intestine
An injury to the wall of the small intestine incurred during a pelvic dissection can be managed without resorting to an intestinal resection if the blood supply to the bowel segment has not been interrupted. Observation of the intestine will show the bowel to maintain a healthy pink color (Fig. 95–1). Next, the edges of the wound should be trimmed with a fine scissors (Fig. 95–2A, B). The cut edges should bleed to further indicate healthy intestinal tissue. Next, a through-and-through closure utilizing 2-0 or 3-0 chromic catgut is placed as interrupted sutures (Fig. 95–2C). A second imbricating layer of 2-0 interrupted silk is sutured into the muscularis and serosa (Fig. 95–2D through F). The suture line is irrigated and the bowel lumen is checked for adequacy between the surgeon’s thumb and fingers.
[/not-level-membership-for-obstetrics-gynecology-category]
