[level-membership-for-dermatology-category]
CHAPTER 9 Clinical Methods for Sclerotherapy of Varicose Veins
‘We feel from our three and one-half years’ experience that the surgeon who believes that there is nothing more required than a syringe, some solution, and a patient to effect permanent obliteration of varicose veins, still has much to learn.’1
Varicose veins represent tortuous dilations of existing superficial veins. They arise because of multiple factors but are always associated with a relatively elevated venous pressure.2 Therefore, it has been considered for decades that treatment initially consists of cutting off the point of high-pressure inflow to the veins (through either surgical or sclerotherapeutic methods) before treating the varicose veins themselves.3,4
This approach has been recently questioned, since, in certain cases, the importance of the ‘siphon’ effect generated by the underlying varicose reservoir is strong enough to generate a reflux in saphenous trunks. It has been observed that suppression of the varicose network reduces reflux in the saphenous trunks. The development of varicose veins in the reticular network and centripetal progression of the disease, as advocated by Hébrant and Collignon, is a hypothesis which could explain a number of varicose patterns, and an increasing number of specialists are currently applying a more distal and conservative approach, whether surgical or sclerotherapeutic.5
Historical Review of Techniques
Tournay (French) technique
The Tournay procedure encompasses the basic principle of ‘French phlebology’ developed by Tournay et al:6 treating varicose veins ‘from high to low’ (‘de haut en bas’). The rationale for this technique is in first eliminating high-pressure reflux blood flow at the point of occurrence. Treating from proximal to distal sites also eliminates the weight of the column of blood on the sclerosed point. This has the advantage of minimizing thrombosis and the extravasation of red blood cells (RBCs) from a sclerosed vein segment. The French school advocates placement of very few injections at this ‘high (proximal)’ point before treating more distal veins or sections of the same vein at a later date. This same philosophy toward treatment was also reported from the Mayo Clinic in 1941 by Heyerdale and Stalker.7 The principle of eliminating reflux from the saphenofemoral junction (SFJ) was espoused even earlier by Moszkowicz8 in Germany in 1927 and by de Takats and Quint9 in the United States in 1930. Thus the ‘French technique’ is multicultural in its origin.
In addition to developing a treatment regimen with the tenet just mentioned in mind, it is critical to obliterate the SFJ accurately because its location and anatomy are so variable (see Chapter 1). To determine the origin of high pressure in the varicose vein, a noninvasive diagnostic evaluation of the patient should be performed first (see Chapter 5). The handheld Doppler device helps detect points of reflux from the deep to the superficial veins, through either incompetent saphenofemoral or saphenopopliteal junctions or perforating veins. In certain circumstances, additional testing is required. If any points of reflux are detected, they should be treated first. After the high-pressure flow has been eliminated, treatment should proceed first with injection of the largest varicose veins, then injection of the reticular feeding veins, and finally treatment of the remaining ‘spider’ veins.
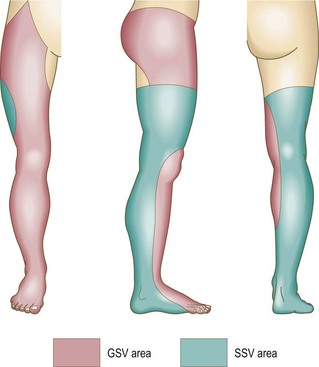
In defense of the logic of the French technique, de Groot4 pointed out that any vein in the leg belongs to either the greater saphenous system or the lesser saphenous system (Fig. 9.1). This concept implies that a vein within the defined area of the great saphenous vein (GSV) eventually drains into the GSV. Therefore, reflux in that vein is derived from reflux at the SFJ. This concept directs treatment toward the reflux point. Unfortunately, clinical examination of the location of a vein does not always correctly determine the point of reflux. Therefore the clinical examination must be correlated with a noninvasive examination to establish the optimal order of therapy.
Sigg (Swiss) technique
In contrast to the French technique, the Swiss technique of Sigg10 and the modification by Dodd and Cockett11 advocate total sclerosation of the entire varicose vein, including incompetent perforator veins (IPVs) and the SFJ. This technique has also been adopted by some physicians who modify Fegan’s technique of sclerotherapy of the IPVs (described in the following section). Included in this school are Reid and Rothnie,12 who treated 1358 legs of 974 patients and found that selective injection of perforator veins was ineffective, requiring multiple additional treatments of the entire vein. They evolved a technique of placing multiple injections at intervals along the varicose veins to produce diffuse sclerosis and have reported very favorable results. This latter technique is called the total-vein sclerotherapy technique.
Fegan technique
Fegan et al13 proposed a view opposite to the previously mentioned one, namely that saphenofemoral incompetence could occur as a result of perforator incompetence alone. They reached this conclusion by demonstrating that the calf muscle pump is more powerful than the abdominal or femoral muscles regarding venous flow in the leg. They proposed that sclerotherapy of the IPVs should be performed first, to restore normal function. Fegan’s examination of the SFJ and GSV with phlebography after sclerotherapy of IPVs showed narrowing of the vessel lumen in 9 of 11 patients.14 However, surgical exploration of clinically diagnosed areas of perforator vein incompetence has found at best a 60% incidence of perforator veins being correctly identified clinically.15 In addition, phlebographic examination performed on 112 patients with clinically suspected incompetent perforators showed that the clinical examination correctly identified only 38% of perforator veins below the knee and only 17% of thigh perforators.16 An additional study of 180 limbs with primary varicose veins studied with clinical examination, ascending deep-to-superficial venography, Doppler ultrasound, and ambulatory venous pressure measurements showed that only 40% of these patients had evidence of perforator incompetence. Of them, 30% had no hemodynamic significance to the perforator veins.17 Thus, the rationale for Fegan’s technique is open to dispute.
Despite the lack of accuracy of clinical diagnosis of IPVs, many authors have found Fegan’s technique gives excellent results. Tolins18 reported favorable results using Fegan’s technique; he injected varicose veins in areas of fascial defects with 0.5 mL of sodium tetradecyl sulfate (STS) solution at up to 23 sites per leg. Although this many injections may seem similar to the number with total vein sclerotherapy, three-quarters of the patients had two to five injections. Doran and White19 concluded after 2 years of follow-up that there was no difference between the results from Fegan’s technique and ligation and stripping procedures for varicose veins. Hobbs20 concluded from his comparative study of sclerotherapy with Fegan’s technique versus traditional surgery that sclerotherapy is the best treatment of nontruncal varicose veins and IPVs of the lower leg. Tretbar and Pattisson21 have found in their follow-up examinations of 264 patients treated with Fegan’s technique that treatment failures usually occurred in patients with very large or fat legs with varicosities originating above the knee. They believed this failure was caused by the difficulty of placing injections accurately within the veins of these patients and maintaining adequate compression. Sladen22 analyzed 263 limbs with up to 7 years of follow-up and found that more than 95% of his patients were satisfied with the treatment and said they would have it repeated. He estimated a retreatment rate of approximately 5% per year. His patients averaged 3.6 to 5.25 injections per treatment session, and 46% to 74% required one treatment session only. Sladen, in agreement with Hobbs, found that all patients with saphenofemoral reflux eventually required surgery. Therefore, although varicose veins treated with Fegan’s technique respond well to treatment, the supposition of Fegan’s technique – that sclerosis of the IPVs is of primary importance and may reverse the remaining pathology in the GSV system – may not be correct universally.
Hobbs23 provided evidence that when saphenofemoral and perforator incompetence occur together, both abnormalities should be corrected. Kerner and Schultz-Ehrenburg24,25 studied the functional effects of sclerotherapy with photoplethysmography (PPG) and concluded that the greatest functional improvement occurred with obliteration of the SFJ. Obliteration of the IPVs of the lower legs was of variable importance. Treatment of perforator veins of the upper leg had no functional significance that could be ascertained with PPG.
Treatment of reflux from the saphenofemoral junction
There are at least three schools of thought regarding which type of therapy is appropriate for initial treatment of the junctional points of reflux: surgical ligation (with or without limited stripping) of the SFJ versus sclerotherapy of the SFJ versus sclerotherapy of IPVs alone. Bergan (see Chapter 10), Goldman,26 Hobbs,20,27 and others argue that surgical treatment of the junctions is the most appropriate and successful mode of treatment, but this was before the use of endovenous ablation techniques. Neglen,28 in a comprehensive review, determined that with proper follow-up, including functional testing at 5 years, surgical therapy of the GSV in a patient with incompetence of the SFJ, is significantly better than sclerotherapy.28 Color-flow duplex evaluation, from 3 to 55 months after treatment (mean of 27.5 months) of 89 limbs in 55 patients with an incompetent SFJ treated with the Sigg technique, found that only 6% of veins remained sclerosed despite improvement in symptoms in 50%.29 Butie30 has shown that sclerotherapy of the SFJ is difficult and unreliable with the use of liquid STS 3%, which is the strongest sclerosing agent approved for use by the US Food and Drug Administration (FDA). This has been confirmed even when sclerotherapy was performed at the SFJ under angioscopic guidance (see ‘Endoscopic injection’ section).31 In this case, 12 GSVs were occluded at the SFJ through angioscopically guided sclerotherapy with STS 3% liquid (prior to the use of foamed detergent sclerosants). A total of 2 to 5 mL was injected into the GSV just below the junction, which was occluded by manual pressure. Nine veins were evaluated at follow-up, and all were reopened and incompetent between 1 and 12 months. Although these carefully performed, unbiased studies have been carried out only recently, this opinion is not new. As far back as 1934, Cooper,32 in a series of more than 85,000 injections in more than 3000 patients, documented that the number of sclerosing injections required to produce obliteration of the varicose vein was markedly decreased after ligation of the SFJ.
In addition to its lack of consistent success, sclerotherapy of the SFJ has the inherent risk of damaging the deep venous system and the femoral vein when sclerosing solution is injected in the upper thigh region. This has been demonstrated by radiologic examination showing the rapid flow of contrast media from a varicose GSV into the femoral vein when injections are performed in the upper thigh.33 With incompetence of the SFJ, it is recommended that sclerotherapy be used for treating residual varicosities after surgery.
Despite the information in the preceding paragraph, multiple phlebologists have demonstrated that the junctions can be successfully closed with sclerotherapy alone in 50% to 91% of patients.34–40 A comprehensive illustrated discussion of the technique is presented in other sources.41 The difficulty in properly evaluating these conclusions is due to the natural evolution of varicose veins, which obscures the results of both surgical and sclerotherapy treatment. It is sometimes difficult to distinguish between a recanalized vein and a new vein. Results also depend on the type of follow-up examinations (i.e. clinical or objective with duplex or Doppler ultrasound) of patients. One study with clinical 6-year follow-up demonstrated a nearly 90% success rate with sclerotherapy.34 By whatever method, closure of the SFJ has been shown in pressure studies to prevent retrograde flow in the saphenous and perforator systems.42 This suggests that incompetence of the perforator veins occurs as a result of a primary development of saphenofemoral reflux. Therefore, when the GSV or its tributaries are involved, the SFJ, when incompetent, should be the first area to be treated.
Treating incompetence of the SFJ may differ from treating an incompetent saphenopopliteal junction (SPJ). The small saphenous vein (SSV) has a variable termination (see Chapter 1) that is often difficult to approach surgically, but can be approached with modern endovenous ablation techniques. Ligation alone at the SPJ has a 95% failure rate at 1 year.43 Sclerotherapy is much more effective, perhaps because of the larger extent of destruction of abnormal feeding veins into this region.43
A comparison of three independent observers regarding treatment outcome of varicose vein surgery shows 60% agreement in assessing visual improvement, with 30% agreement between observers when symptomatic response and visual impression are compared.44 It is my opinion that no one ‘school’ is absolute but that the correct order of treatment should be individualized for each patient. Some patients have only perforator incompetence and a normal SFJ; thus, Fegan’s technique would be adequate. Patients with saphenofemoral incompetence require treatment of that junction before treatment is initiated elsewhere. Still other patients have no obvious hemodynamic cause for the origin of their varicose veins, thus directing treatment toward the entire varicosity, as described by Sigg.45 A careful workup of all patients is necessary before therapy is begun. In addition to deciding on the sequence of treatment, the physician must consider the various modifications of the injection procedure that some physicians profess have various benefits. As before, comparative and objective studies of these treatment modifications have not been reported. This chapter discusses sclerotherapy treatment of varicose veins, perforator veins, and the SFJ and reviews the available literature. Variations in treatment are addressed, and illustrative cases are presented. A summary of the three schools of sclerotherapy is found in Table 9.1.

Injection Technique
Patient position
Standing
Although the previous description of the treatment of varicose veins seems simplistic, the actual treatment methods for achieving effective sclerotherapy are numerous. Until the 1950s, sclerotherapy was performed with the patient standing throughout the procedure. The purpose was both to distend the varicose vein, allowing easier needle insertion, and to produce firm thrombosis of the treated vein.46 Multiple disadvantages of varicose thrombosis were realized (see Chapter 8), and various methods were devised to limit postsclerotherapy thrombosis. Additionally, injecting sclerosing solution while the patient is standing forces the injection to occur against the hydrostatic pressure of a large column of blood. This may cause the solution to seep along the needle into the perivenous tissues, possibly leading to a chemical phlebitis or tissue necrosis.47
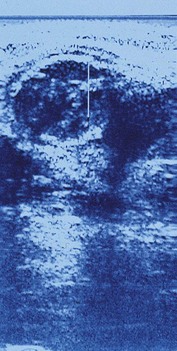
Another disadvantage of the total standing technique is the sclerosing solution may escape through a perforator vein and damage the deep veins, especially if more than 1.5 mL of sclerosing solution is injected in a single site.48 Another radiographic study has shown that an injection of 0.5 mL of contrast media travels rapidly (in 5 seconds) 8 cm distal to the injection site.49 Also, this amount of contrast does not completely fill the vein. An additional radiographic study of the standing position, using metrizamide (Amipaque) 150 as the contrast media (diluted to an isomolarity and specific gravity similar to that of polidocanol (POL)), showed that the injection of 1.5 mL remained in contact with a convoluted varicosity for approximately 10 seconds before flowing rapidly into the deep venous system through a presumed perforator vein (Fig. 9.2, A and B).50 In contrast, when the patient was supine, the contrast media extended proximally along the varicosity and remained relatively undiluted for more than 18 seconds (Fig. 9.2, C and D).50 However, injections in some patients, when using the latter technique, also resulted in the contrast media’s remaining in contact with the varicosity for a longer period with the patient in the standing position (Fig. 9.3). Therefore, multiple variables, including the type of varicosity, its location, the location of associated perforator veins, and the movements of the patient (with associated calf and foot muscle contraction) while standing, may all affect the distribution of the sclerosing solution. For these reasons, the standing technique is not recommended.
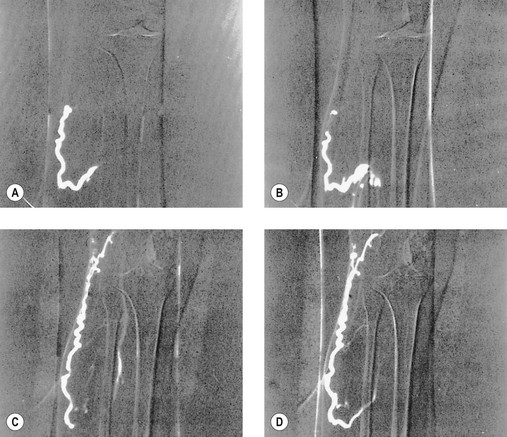
 seconds and, B,
seconds and, B,  seconds after injection into a varicose vein while the patient was standing. Injected contrast media, 1.5 mL, shown, C,
seconds after injection into a varicose vein while the patient was standing. Injected contrast media, 1.5 mL, shown, C,  seconds and, D, 18 seconds after injection into a varicose vein while the patient was supine.
seconds and, D, 18 seconds after injection into a varicose vein while the patient was supine.
Standing and reclining
A modification of the standing technique, the standing and reclining technique, was described in 1926 by Meisen.51 In the standing position, the needle was inserted while the vein was distended. With the needle still in the vein, the patient reclined on a table and the leg was elevated. This produced a relative emptying of blood from the vein. The sclerosing solution was then injected into an ‘empty’ vein that was immediately compressed to prevent or minimize thrombosis.
One of the earliest methods used to limit thrombosis was that of isolating the injected vein segment with pressure placed above and below the needle insertion site after first milking the blood out of the vein.52 One of the first books on sclerotherapy treatment of varicose veins is Varicose Veins and Their Treatment by ‘Empty Vein’ Injection.53 In this book, Ronald Thornhill of London detailed his success with injection of a quinine solution into the elevated leg. He massaged the solution throughout the vein, injecting from distal to proximal. He even sclerosed ‘hair veins’ with a dilute solution. Unfortunately, he did not use compression except when ulcers were present, and his patients had to endure weeks of tender veins until they resolved in approximately 12 months.
Lufkin and McPheeters54 emphasized the importance of empty vein injections in a histologic evaluation of treated veins in 1932. Orbach55 has stressed the significance of compressing the vein to minimize thrombosis since 1943. Thus, these modifications are not new. They result both in improved efficacy and in a decreased incidence of complications when the treatment is directed at the SFJ.19 The improved efficacy may be the result of a longer length of sclerosis of the varicose vein, caused by gravitational flow of the sclerosing solution. However, recent evaluations comparing standing and reclining methods of treating varicose veins below the SFJ have not been performed.
Leg elevation (Fegan)
Another obvious disadvantage of the standing technique is the vasovagal reaction (see Chapter 8). To prevent the sequelae of a vasovagal reaction, Fegan56 recommended that patients sit at the end of the examining table with their legs hanging down while the physician, sitting in front on a low stool, inserts the needle. The leg is then raised while the patient fully reclines for 1 to 2 minutes to empty it of blood. The physician stands to support the raised leg, which is rested on the shoulder or against the chest, and the varicose veins are injected. With this or any technique that moves the patient after the needle is inserted, it is important to ensure that the needle is not displaced from the vein, either by fixing it to the skin with tape (if butterfly catheters or needles attached to syringes are used) or by holding the needle while the leg is raised. Since the varicose veins will collapse when the leg is raised, blood withdrawal must be checked as soon as possible after the leg is raised to ensure that the needle has not slipped out of the vein. The lack of spontaneous pulsatile flow from the needle without an attached syringe is proof of nonarterial placement of the needle.
To ensure that the sclerosing solution acts on the intended vein segment during injection, Fegan56 recommended applying pressure with fingers a few centimeters proximal and distal to the injection point. Finger pressure is maintained for 30 to 60 seconds, and the leg is then bandaged from the toes to the injection site. With this method, injections are made only at the points of fascial defects (which are thought to represent sites of IPVs). Injections proceed from distal to proximal sites, with each vein segment or fascial defect treated.
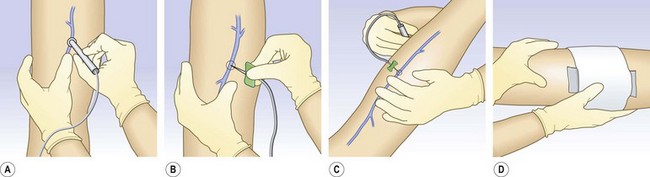
After injection of varicose veins in the elevated leg, compression should be applied immediately to prevent the vein’s filling with blood. This can be performed easily with the use of the following method. Before insertion of the needle, a compression stocking is placed over the foot and heel and allowed to bunch up at the ankle. After the needle is inserted into the varicosity, the leg is raised. Proper placement is then confirmed through blood withdrawal, and the sclerosing solution is injected. A foam pad is placed over the injection site and secured in place with foam or elastic tape. The compression bandage then can be advanced over the injection site and foam pad in a distal to proximal manner (Fig. 9.4). With this technique, radiographic studies after injection of 0.5 mL of contrast medium show that when the leg is raised above the horizontal plane, the contrast medium travels rapidly for 30 cm before reaching the deep venous system.49 The sclerosing solution is diluted and probably inactivated by the time it reaches the deep venous system (see Chapter 7). With this technique it may not be necessary to repeat injections every few centimeters in the varicose vein.
With the leg-raising technique the varicose vein would be presumed empty of blood, but this is not the case. Duplex examination demonstrates that the GSV is not totally emptied of blood, even with an 80-degree incline, although tributaries to the GSV are emptied at 45 degrees.57 In ‘huge’ varicosities, as much as 18 mL of blood can be withdrawn when the leg is raised 45 degrees above the horizontal.58 Therefore, Perchuk58 developed a method for ensuring an ‘empty’ vein. His method consists of inserting the needle into the varicose vein, elevating the leg 45 degrees, and then withdrawing blood through that needle into a syringe until further blood withdrawal is impossible. Then, a syringe with sclerosing solution is attached to the needle and the injection is made, followed by application of local pressure for 5 minutes. The use of compression bandages or stockings after treatment was not mentioned. A two-way stopcock may also be used for this technique. Perchuk, in an evaluation of 84 patients, found that this technique produced excellent results and limited all complications.58 Pigmentation, thrombophlebitis, and recurrence were very rare. Fegan,59 however, disagreed with Perchuk’s conclusions and stated that the vein would empty of blood if raised for a longer time and at a more acute angle.
Two-phase (Sigg) technique
A variation on the method described previously is the two-phase technique of Sigg.10 This variation involves the way the needle is inserted into the vein. Sigg recommended the needle be passed through the vein with the syringe unattached or with a finger placed over the hub and then slowly drawn back until the escape of blood indicates proper placement. The needle is left open and unobstructed while an assistant places a basin beneath it to catch the dripping blood. The leg is then raised above the horizontal plane, and bleeding stops. A syringe is then attached, and blood is withdrawn. After proper placement is confirmed by withdrawal of venous blood and the vein is emptied of blood, the sclerosing solution is injected and the vein compressed, as described above, with a stocking, bandage, or both. Since Sigg uses mainly iodinated iodine solutions, he developed this technique to ensure continual intravascular placement of the sclerosing solution (see Chapters 7 and 8).
Reclining
Another method for injection advocated since the 1920s is that of having the patient remain horizontal throughout the procedure.60 If the varicose veins easily collapse in this position, they can be marked with indelible ink before the procedure, while the patient is standing. A radiologic study has shown a 0.5-mL bolus of contrast medium injected into a varicose tributary of the GSV travels proximally 8 cm and remains within the vessel for approximately 2 minutes before being drawn into the deep venous system.49 The relaxation of the calf muscles permits the injected fluid to stay within the vein, since blood flow in this position is slow. Thus, this position produces the longest lasting and most uniform contact between the injected solution and the vein wall.
To produce a relatively bloodless vein during injection in the horizontal position, some authors advocate rubbing along the vein in both a proximal and distal direction away from the injection site.60 Manual compression is then maintained at the proximal and distal sites along the vein to prevent the vein segment from refilling with blood. After the injection, a compression pad and bandage are immediately applied to the treated vein segment.
Foam sclerotherapy
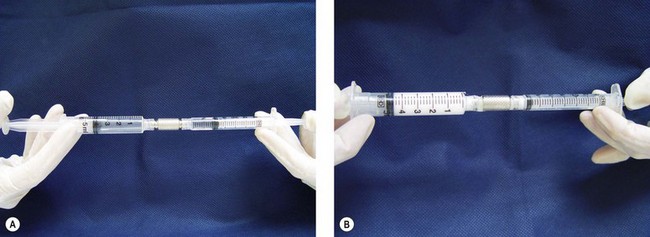
Since the earlier editions of this textbook, the use of foam sclerosants has increased dramatically. Far from the primitive techniques described by so many authors and well detailed in Wollmann’s history of sclerosing foams,61 it is now considered as a completely new treatment for varicose veins.62,63 Shaking the syringe60 or aspirating in a closed glass syringe,64 to quote only two of the well-known historic methods, are now obsolete. Three main options remain: high-speed beating in a carbon dioxide-rich atmosphere (Cabrera’s technique65), specific gas mixture combined with POL and passed through a patented sieve in an aerosol canister (Varisolve, Provensis Ltd., UK), and Tessari’s method, using the transfer between two syringes of sclerosant and room air. The latter technique offers different variations: a three-way stopcock as initially described66 (Fig. 9.5), a two-way female connector like in the DSS technique67 (Fig. 9.6), or an automated foaming device, Turbofoam (KreusslerPharma, France), described in Chapter 7, which has the ability to mix the sclerosant with different types of gases through the use of a three-way connector. The Tessari technique is the most common means for foam creation.68

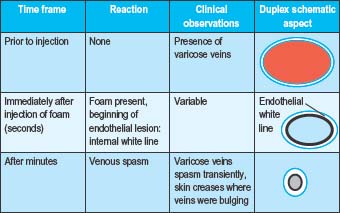
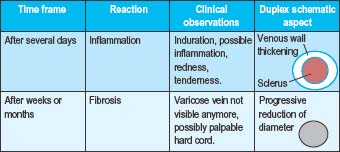
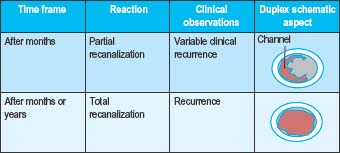
Immediately following the injection of foam sclerosant, the bubbles displace blood and contact with the sclerosant and endothelium begins. Clinically, this is apparent as vasospasm within seconds or minutes, erythema of the feeding telangiectasias, or no immediate visible change (Table 9.2a Pt1). After several days, venous inflammation is present with thickening of the venous wall and presence of a sclerus. This is evidenced clinically by induration, erythema, and tenderness. Weeks to months later, fibrosis results in a progressive decrease in the diameter of the treated vein and clinically by the absence of the varicosity. Occasionally, a fibrous cord may be palpated (Table 9.2b Pt2). At times, complete clearance of the varicose veins does not take place, owing to either partial or total recanalization of the treated vein (Table 9.2c Pt3).
Table 9.2 A-C Pathophysiologic and clinical effects from foam sclerotherapy
 |
 |
 |
Foam sclerotherapy is now regarded as far more efficaceous than liquid sclerotherapy for larger veins due to an increased time of contact between the sclerosant and the vein wall.68 The temporal relationship between foam bubbles and the endovenous wall is related to patient position, injection technique, foam viscosity, and the number of bubbles per milliliter.69 Hamel-Desnos et al67 investigated efficacy rates of a single treatment session of foam or liquid ultrasound guided sclerotherapy of GSVs. The induction of venous spasm was more common following foam sclerotherapy. At 3 weeks follow-up, reflux was absent in 84% of foam sclerotherapy treated veins and 40% of liquid sclerotherapy treated veins. A similar study was performed by Yamaki et al70 to investigate single treatment foam versus liquid sclerotherapy in GSVs and tributary veins. At 12 months, complete occlusion rates were 67.6% and 17.5% in the foam and liquid groups, respectively. Statistically significant increased rates of recurrent varicose veins and recanalization with reflux were identified in the liquid sclerotherapy cohort. A 2009 meta-analysis revealed a 76.8% efficacy of ultrasound-guided foam sclerotherapy (UGFS) as compared to a 39.5% efficacy rate for ultrasound-guided liquid sclerotherapy.71 An additional benefit from foam is its appearance on ultrasound as an intravenous contrast agent. Multiple randomized controlled studies comparing the incidence of adverse events with foam and liquid ultrasound-guided sclerotherapy of the saphenous veins have shown no statistical difference between these techniques.67,71,72
A metanalysis by Van den Bos and colleagues73 compared occlusion rates following endovenous laser ablation (all wavelengths included), radiofrequency (RF) ablation, UGFS, and high ligation with stripping from 64 studies and 12,320 limbs. At 3 years, success rates were 94.5% for laser ablation, 84.2% for RF, 77.4% for UGFS, and 77.8% for high ligation with stripping. After 5 years, the respective treatment success rates were 95.4%, 79.9%, 73.5%, and 75.7%. The authors found efficacy for high ligation and stripping, RF ablation, and UGFS were equal, but endovenous laser ablation therapy (EVLT) was more effective than the other three regimens.
All foams are not the same, as explained by Wollmann.61 Even if prepared with the same agent (foams can be produced only with detergents – namely, STS and POL and, rarely, sodium morrhuate), foams can have different properties depending on the mode of preparation and the gas to air ratio (dilution factor). Foams are wet or dry, accordingly. This difference is thought to have some impact on efficacy. Drier foams tend to break down on passage through a needle while wet foams act more like liquids. Between these extremes, foam is relatively stable and will displace blood from the vein. Liquid sclerosant to gas dilution ratios of 1 : 4 (1 part liquid to 3 parts gas) or 1 : 5 (1 part liquid to 4 parts gas), have been found to produce the most stable foams.74 Currently, most physicians use a foam prepared just prior to injection with a method derived from Tessari and a ratio of solution to air varying from 3 to 5 mL of air to 1 mL of solution (we recommend 4 mL). Some standardization has happened spontaneously.
Foam stability
Foam stability is affected by foam composition, foam volume, and injection technique.75 Composition variables, including the homogeneity of bubble size, viscosity, and temperature, all influence the ‘quality’ and longevity of foam (Table 9.3).76 Heat increases the stability of foam.77
Bubble size is inversely related to the difference in density between a liquid and gas, as represented in the equation below.76
where
Carbon dioxide is 1.5 times denser than room air; therefore, foam bubbles prepared from carbon dioxide are smaller than those of air. Foam bubbles produced via turbulent flow in the Tessari technique and the double syringe system are smaller (less than 100 µm) in size as compared to the larger bubbles produced in the Monfreux technique. This smaller bubble size is associated with an increased surface area of sclerosant, increased displacement of blood inside the vessel, and decreased likelihood of mixing with blood following the initial injection. Therefore, an increased amount of sclerosant can be delivered to the endothelial cells.78,79 Interestingly, the Monfreux method of foam creation has been associated with an increased incidence of side effects. It is speculated that the larger bubbles produced in this method advance more readily in the venous system.78
The majority of phlebologists utilize readily available room air for foam creation in sclerotherapy; however, carbon dioxide is becoming increasingly popular.80 Carbon dioxide foam bubbles quickly disintegrate; this effect is more pronounced as the sclerosant to gas ratio is increased.61 The following equation describes foam stability in vivo:

Carbon dioxide has a much greater diffusibility into blood as compared to nitrogen (the dominant gas in room air), and as a result, the foam-half life is reduced for carbon dioxide. When carbon dioxide is mixed with oxygen for foam creation, the foam-half life is increased due to the decreased diffusibility of this mixture.81
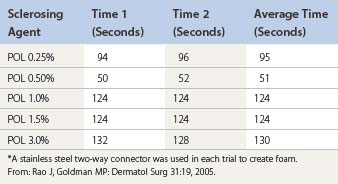
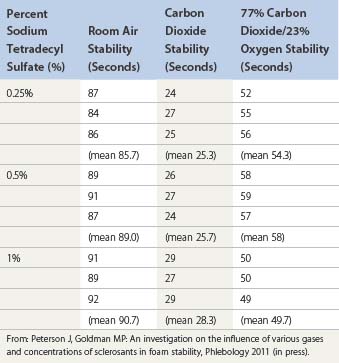
Room air foam half-life varies according to the percent of sclerosant solution. In the study by Rao and Goldman,82 they found a 1% concentration of STS or POL had the maximal foam half-life (90 and 120 seconds, respectively) (Tables 9.4 and 9.5). We recently discovered carbon dioxide foam half-life did not vary according to the concentration of sclerosant solution; however, a mixture of 77% carbon dioxide/23% oxygen did. We also found that foam half-life for room air is over three times longer than carbon dioxide half-life and 1.5 times longer than a combination of 70% carbon dioxide/30% oxygen (see Table 9.3).83
Table 9.4 Times for 0.5 mL of sodium tetradecyl sulfate (STS) to settle from a foam mixture containing 1.0 mL of various STS concentrations*
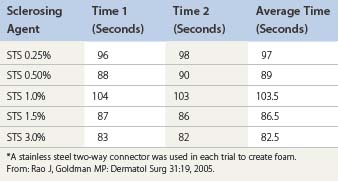
Table 9.5 Times for 0.5 mL of polidocanol (POL) to settle from a foam mixture containing 1.0 mL of various POL concentrations*
Silicone coating is present in syringes and syringe connectors to provide lubrication, but silicone is also an anti-foaming agent. Prior studies by Rao et al and Lai et al, have shown the amount of silicone in syringe connectors does not affect foam stability; however, foam stability varies between syringe manufacturers due to variances in the silicone content of their syringes.82,84 Hill85 investigated the effect of a 5 µm syringe filter on carbon dioxide foam half-life. In the absence of the filter, foam half-life was 22.7 and 30.1 seconds for STS 2% and POL 2%, respectively. Half-life was prolonged to 35.9 and 48.9 seconds, respectively, with the addition of a 5 µm filter. Of note, carbon dioxide foam stability was greater in POL versus STS throughout the study.
Foam has a spontaneous evolution before and after being injected in varicose veins. Before injection, small bubbles tend to group as bigger units (known as LaPlace’s law) and after some time foam is replaced by large bubbles whose effect will be what was observed with Orbach’s air-block. Stability of the foam can be evaluated by several techniques,82 and one should not talk about foam when prepared more than 90 seconds in advance. The preparation of foam does not change the concentration of sclerosing agent. This is completely different from what happens to the foam when injected. If injected into an isolated segment, a plug of foam is created and behaves as in a syringe, remaining in contact with the endothelium long enough to destroy it and induce venospasm. As the foam is forced from the contracting segment of vein, it mixes at the expanding interface with blood. This is responsible for dilution of foam and the scattering of bubbles, and surface sclerosing agent is rapidly deactivated by attachment to plasma protein and cell membranes. This explains why bubbles, when found far from the injection site for example, in the lung, heart, or brain consist of air and do not carry detectable amounts of sclerosing agent or have any sclerosing properties.86
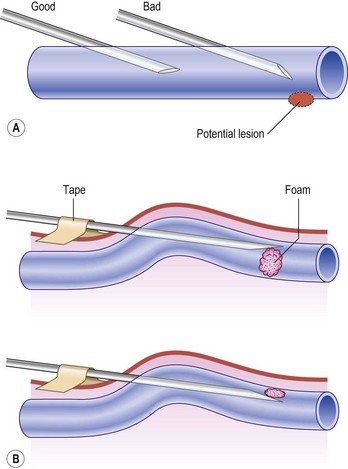
Regarding the use of foam, the trend in Europe is to develop a consensus for volumes and concentrations.80,87 At the 2nd European Consensus Meeting on Foam Sclerotherapy, experts agreed than no more than 10 mL of foam per injection should be injected into a GSV. The range of volume injected into the GSV varied between less than 2 mL up to 10 mL per injection. The maximum recommended volume of foam per leg and per session was felt to be 10 mL. The Monfreux technique of foam creation was no longer recommended for any subtype of vein.80 In France, there appears to be a reduction in concentrations,88 with vessel spasm used as an indicator for the correct amount of foam injected. However, this option is true only for a proximal and direct injection of terminal parts of the saphenous veins. We have previously advocated for a more distal approach62 with placement of an open vein access (‘butterfly’ needle or catheter; Figs 9.7 and 9.8), filling the vein with relatively low volume concentrations, and massaging to the desired area under duplex control (Fig. 9.9). With several years of experience this is no longer deemed necessary. The necessary volume can be estimated from the diameter and the length of vein, as indicated in Table 9.6. In our practice, however, we do not currently use volumes above 10–12 mL in a single vein. It should not be forgotten that although foam is not air and usually occupies the entire vessel lumen, foam floats, so that in large-diameter veins it will principally be in contact with the upper part of the vein, where gravity leads it (Fig. 9.10). The only solution to this problem is a reduction in the diameter, which can be obtained by compression, leg elevation, or induction of venous spasm. Ten to thirty milliliters of normal saline can be injected perivenously, in a technique similar to tumescent anesthesia for endovenous laser or RF ablation, to cause venous compression and decrease recurrence rates.89



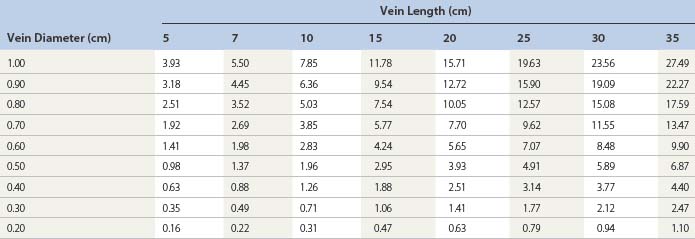
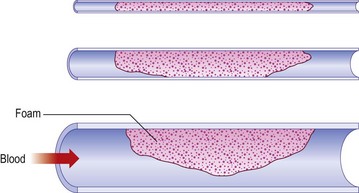
Figure 9.10 Effects of Archimedes’ law on foam contact with venous wall in veins of various diameters.
The most common technique for foam sclerotherapy is via ultrasound guidance81 and using the direct puncture technique.80 While many authors employ short catheters, long catheters with balloon tips have become more prevalent due to a possible increased efficacy. However, long catheters may cause an increased incidence of deep venous thrombosis81 due to a passage through perforators, even if foam is re-aspirated at the end of the procedure. The recommendations from the 2nd European Consensus Meeting on Foam Sclerotherapy is to inject the GSV at the proximal thigh if using the direct puncture technique and distal to the knee if using long catheters. For the SSV, injection should be at the level of the mid calf in order to minimize adverse events including canulization of the popliteal artery.80
Even if every phlebologist using foam sclerotherapy has been impressed by results (see Case Study 13 later in this chapter), evidence-based medicine applies to phlebology too and controlled trials are needed to demonstrate the validity of the technique. Efficacy of foam sclerosants is more substantially documented today than it was when writing the previous editions of this textbook and evidence is now available.67,70,90–92 Cabrera et al93 have followed 500 lower limbs treated with their unique carbon dioxide-foam mixture, with no greater than 81% of the GSV and 96.5% of the superficial branches remaining closed at over 3 years. Results have not been as impressive when room-air-generated foam is used. Fruillini and Cavezzi78 found an 88% success rate when the foam was generated with the glass syringe/Monfreux technique versus 93% when generated with the Tessari technique. Although their follow-up was 20 to 180 days, it is clear that the method for generating foam is important regarding treatment efficacy. Even Tessari reports a 74% efficacy of complete obliteration in a 2-year evaluation of 38 GSVs and SSVs and 194 collateral branches treated.94 In a randomized controlled trial, proprietary pharmaceutical polidocanol microfoam (PPPM; Varisolve) was compared with superficial vein surgery or sclerotherapy in 654 patients with moderate to severe saphenous vein (GSV or SSV) incompetence. The overall success rates were 83.4% for PPPM and 88.1% for control at 3 months, and 78.9% and 80.4%, respectively, at 12 months; at neither time point was the difference significant.95
A 3-year follow-up study in UGFS using either STS or POL for the GSVs, SSVs, and their tributaries revealed a 52.4% success rate. Veins that failed the primary treatment session were re-treated. The 3-year success rate for this group was increased to 76.8%.96 A 5-year 56% efficacy rate was found in a prospective study investigating UGFS prepared from STS of the GSVs. This protocol consisted of weekly foam sclerotherapy treatments until reflux was no longer detected by ultrasound. Additional treatments were performed if recanalization was detected. Currently, this study contains the longest follow-up duration of all published studies on foam sclerotherapy.97 In a recent meta-analysis that included 9000 patients, the median efficacy of foam sclerotherapy was 87% with a median recurrence rate of 8%.68
Darke and Baker98 investigated the number of UGFS treatment sessions required for clinical evidence of complete occlusion of varicose veins. Clinical complete occlusion rates at 6 weeks following the last treatment were as follows: 74.1% with a single treatment, 89.1% with two treatments, and 89.5% with three treatments. O’Hare et al99 found no difference in efficacy rates at 6 month in veins of less than or greater than 7 mm in diameter that were treated with UGFS. However, Myers et al96 found that treatment success was decreased in veins greater than 6 mm as compared to veins of less than 5 mm. This report also concluded success rates were higher in GSVs versus SSVs.
Multiple studies have investigated the influence of various sclerosant concentrations in relation to the efficacy rate of foam sclerotherapy. Efficacy rates were highest for POL 1.5% or STS as compared to 3% or more dilute concentrations in a study investigating saphenous veins and their tributaries.96 A similar study investigating POL for UGFS of GSVs less then 8 mm found short term (3 week) success rates of 96% and 88% in subjects receiving POL 3% foam and POL 1% foam, respectively (difference was not statistically different). After 2 years, the success rates were 69% in patients treated with POL 3% foam and 68% in those treated with POL 1% foam.88 Ceulen et al100 initially found a significant difference in efficacy rates of UGFS between 1% and 3% POL foam at 1-year follow-up (69.5% and 80.1%, respectively). However, when these subjects were followed for 2.5 years, there was no difference in efficacy between the two concentrations of POL (66.7% and 66.8%, respectively).101 No exclusion criteria were made in this study with regards to the diameter of the GSV.100,101
Side effects
A foam bolus can even occur when a small quantity of foam is injected. Hill et al75 showed that leg elevation, but not manual pressure of the SFJ, decreased the migration of foam in sclerotherapy in UGFS of the great saphenous vein. At least this could ensure that bubbles will be washed of their sclerosing molecules, but will release much bigger bubbles. Other methods to decrease foam migration include multiple, sequential injections of foam sclerosant volumes less than 0.5 mL.102 A meta-analysis investigating side effects in over 9000 patients by Jia et al68 found the median rates of deep venous thrombosis and pulmonary embolus were less than 1% each. The median values of visual changes and headache were 1.4% and 4.2%, respectively. Chest tightness and coughing occurred in less than 1%. In a large, prospective, multicenter study of foam sclerotherapy in 1025 patients the incidence of migraine was 0.78% (with aura 0.59%;.19% without aura), visual disturbance 0.68%, chest tightness 0.68%, chest tightness with visual disturbance 0.49%, deep venous thrombosis 0.98%, pulmonary embolism 0.1%, and transient ischemic attack 0.1%.103
A recent study of patients with incompetent GSVs treated with UGFS created from either carbon dioxide or room air, in a 1 : 4 sclerosant to gas dilution ratio, demonstrated decreased incidences of foam-bubble-related side effects including chest tightness (3.1% to 18%), cough (1.6% to 16%), and dizziness (3.1% to 12 %). There was a trend towards decreased visual disturbances in the carbon dioxide versus room air group (3.1% to 8.2%), though this difference was not found to be statistically significant. There were no differences in vital signs or echocardiogram (ECG) changes between the two cohorts. An overall 71.79% decrease in bubble-related side effects (as compared to room air) was attributed to the carbon dioxide foam.104 When cerebral emboli were monitored via transcranial Doppler ultrasound in patients treated with foam created from either room air or a 70% carbon dioxide/30% oxygen mixture, no statistical differences were found between these two cohorts with regard to the rate of high intensity transient signals in the middle cerebral artery.105
One can speculate that the decreased upstream foam-related side effects are attributable to the short carbon dioxide foam half-life83 and the increased diffusibility of this gas into blood in comparison to nitrogen and oxygen.81,83 In a study of 116 patients with stasis ulcers, the incidence of visual changes and cough occurred in less than 2% of patients treated with carbon dioxide created UGFS.106 In a large multicenter prospective study by Guex et al, visual disturbances occurred in 0.28% of patients treated with foam sclerotherapy created using room air.107
Intravenously injected bubbles of less than 10 µm do not produce symptoms in patients, regardless of the presence of a patent foramen ovale.108 Ceulen et al109 noted foam microbubbles created from room air appeared in the right atrium and ventricle 0.75 to 15 minutes following injection. In the small study by Morrison et al,110 foam bubbles were identified in the deep venous system and the right atrium within 10 seconds of the initial injection of foam sclerotherapy into a 1-mm telangiectatic vein. This finding was reproducible in all 15 subjects. In a related study, these bubble emboli ‘showers’ could last minutes and were present in the left side of the heart in 33% of subjects, indicating a shunt. Of interest, 57% of this group of patients showed transcranial Doppler evidence of bubble emboli.111
Four cases of transient ischemic attacks and cerebrovascular events have been reported in the literature. All patients had examples of right to left cardiac shunting, such as patent foramen ovale and atrial septal defects, discovered on further workup.103,112,113 These bubbles can appear in the middle cerebral artery in under 35 seconds.114 Treatment for foam-induced neurological events includes administration of 100% oxygen followed by immediate transfer to an emergency department and the initiation of hyperbaric oxygen therapy.113 As the dominant gas in room-air bubbles is nitrogen, foam bubble half-life is decreased as the concentration of oxygen increases and the nitrogen decreases.115 Theoretically, in the event of cerebral emboli, the osmotic diffusion of oxygen and nutrients should be able to compensate for small bubbles but not larger bubbles.116
Deep venous thrombosis is a rare occurrence in foam sclerotherapy with an incidence of 0.015%.107 Shadid et al117 recommends maintaining a high index of suspicion for the development of deep venous thrombosis when superficial thrombophlebitis occurs distant from the treatment area. Pulmonary embolus have been reported following UGFS.103,118 Infection is a rare event following foam sclerotherapy, but cases of cellulitis and Klebsiella sepsis have been reported.119
Our technique for the treatment of reticular and telangiectatic leg veins
Our classification for veins are as follows: varicose veins are torturous and larger than 4 mm, reticular veins range from 1 to 4 mm, and telangiectactic veins are less than 1 mm. For the most successful outcome of foam sclerotherapy of telangiectatic leg veins, the feeding incompetent reticular veins must be treated simultaneously. At our clinic, we initiate with treatment of refluxing veins, the largest veins, and proceed in a proximal to distal fashion. The double syringe system with room air in a 1 : 5 dilution (1 part sclerosant solution: 4 parts gas) is our preferred method for foam creation. For reticular veins between 1 and 3 mm, we prefer STS 0.25% or, alternatively, POL 0.25% to 0.5%. We increase the concentration of STS to 0.5%, and POL up to 1%, for veins 3 to 5 mm in diameter. Telangiectatic leg veins are treated with liquid STS 0.25%, liquid POL 0.5%, or glycerin 72% with lidocaine 1% or without epinephrine (adrenaline). Our patients remain in the supine position without leg elevation for the duration of the treatment. Following treatment, the patient remains supine as nursing staff apply 30 to 40 mmHg compression stockings. Immediate ambulation for 15 to 30 minutes is required. For the next week, 24 hours a day (for one author RAW, only during waking hours), the patient remains in their compression stockings.120,121
Other applications of foam sclerotherapy
Ulcers
Foam sclerotherapy is also effective in the treatment of venous ulcers. Cabrera et al106 investigated carbon dioxide-POL foam in 116 patients with venous stasis ulcers and found complete resolution at 6 months in 83% of patients. Either the saphenous veins, perforator veins, or a combination were injected under ultrasound guidance. The mean time for complete resolution of an ulcer was 2.7 months. Long-standing ulcers (over 24 months), size greater than 2 cm, patient age over 65 years old, a history of venous surgery, and incompetence of the deep venous system were negative prognostic indicators.
Venous Malformations
Foam sclerotherapy can decrease the progression and size of venous malformations, including Klippel-Trénaunay syndrome.79 In a study by Yamaki et al,122 subjects with symptomatic venous malformations, including limited, infiltrating, and complex-combined variants, received ultrasound guided foam or liquid sclerotherapy. The sclerosants investigated were 1% POL foam or liquid for treatment of the superficial component and 10% ethanolamine oleate for the deep components of the venous malformation. As complete resolution of venous malformations would not be realistic in all patients in this study, patients received enough sessions until patient-perceived cosmetic satisfaction was obtained or when no further benefit was anticipated. A significant decrease in volumes of sclerosants (both POL and ethanolamine oleate) were found in the foam cohort. On 6-month follow-up duplex evaluation, increased rates of disappearance (defined as occluded and shrunken venous space) and partial recanalization (defined as partially recanalized and partially shrunken venous space) were greater in the foam group versus the liquid group (45% and 45% versus 25% and 15%).
Combination therapy
Foam sclerotherapy with saphenofemoral ligation versus high ligation, stripping, and multiple phlebectomies was evaluated by Kalodiki et al.123 With 3-year follow-up, there was no statistical difference in the recurrence rates between these two treatment regimens on Doppler ultrasound evaluation.
Foam sclerotherapy can be combined with endovenous laser ablation at the time of surgery or can be performed at follow-up visits. In a study by King, UGFS was combined with either the 980 nm or 1320 nm endovenous laser for the treatment of incompetent saphenous veins. At 1-month follow-up, treatment success was seen in 97% of patients.124 Further long-term data and controlled clinical trials will be necessary to evaluate whether combined endovenous laser ablation combined with foam sclerotherapy is superior to endovenous laser ablation alone. Any varicosities remaining at 6 weeks post procedure and distal to the site of endovenous ablation should, in our experience, be treated by foam sclerotherapy.
Contraindications
Patent Foramen Ovale
Patent foramen ovale (PFO) is present in 27% of the general population,111,112,125 and decreases in prevalence with increasing age. Transesophageal echocardiogram with contrast is the recommended screening test for the detection of PFO, but transcranial Doppler ultrasound is almost as sensitive.126 Right to left cardiac shunting can occur in the presence of a PFO, atrial septal aneurysm, or any opening between the atria, ventricles or the great vessels.127 Pulmonary arteriovenous malformations can lead to extracardiac shunting and occur in 10% of the population.111 All of the previously listed forms of shunting can result in cerebral vascular system emboli. The incidence of cryptogenic stroke is greater in patients of all ages with PFO127 as compared to the general population.128 Two prospective studies found migraines associated with an aura occur more commonly in patients with PFO.129,130
In a report by Morrison et al,110 15 patients were screened for a PFO with an ECG prior to foam sclerotherapy. Allthough echocardiogram screening revealed no PFO, intraoperative transthoracic ECG monitoring revealed the presence of four PFOs which were accentuated because of the increased visibility of foam. A 2010 study by Wright et al126 found 58.8% of patients with varicose veins (CEAP C3-5) had a right to left cardiac shunt as evidenced by the appearance of bubbles in the middle cerebral artery on transcranial Doppler (at rest or with a Valsalva maneuver) using agitated saline. Next, 61 patients with a right to left heart shunt were treated with UGFS with 1% POL foam created from a 70% carbon dioxide/30% oxygen mixture; 89% had evidence of bubble emboli in their cerebral vascular system. No patients were symptomatic throughout this study. In a study of 3259 patients treated with UGFS, 7 patients (0.21%) experienced foam-related side effects including visual disturbances, chest tightness, and migraine with aura. Of these seven patients, five tested positive on transcranial Doppler examination, indicating the presence of right to left cardiac shunting such as with a PFO.131
A known symptomatic PFO is considered an absolute contraindication for foam sclerotherapy by the 2nd European Consensus Meeting on Foam Sclerotherapy. However, the committee agreed that it is not necessary to screen for a PFO in an asymptomatic patient prior to foam sclerotherapy treatment.80
Thromboembolism and Thrombophilia
An absolute contraindication for foam sclerotherapy is the presence of an acute deep or superficial venous thrombosis. If a patient has a prior history of a deep venous thrombosus or thrombophilia, it is considered a relative contraindication. These patients should undergo a full workup to determine the etiology of thrombophilia, treatment for 7 days with prophylactic low molecular weight heparin, and be administered limited volumes and decreased concentrations of foam sclerotherapy.80 In the study by Wright el al,95 the incidence of deep venous thrombosis decreased when small volumes were utilized per injection and the injection was ceased and compression applied when foam was present 5 cm from the saphenofemoral or saphenopopliteal junction.
Migraine
A straightforward migraine is not considered a contraindication to foam sclerotherapy.80 However, we found that patients with history of ophthalmic migraine (see Chapter 8) where likely to have more frequently visual disturbances after foam sclerotherapy; this must be explained at the time of informed consent.
Other injection techniques
Air bolus
The air-bolus technique was first advocated by Orbach60 to ensure that sclerotherapy treatment of varicose veins occurred with minimal thrombosis. The rationale for instilling air before injecting the sclerosing solution is that clearing the vessel of blood allows undiluted contact to occur between the solution and the vessel wall. This procedure was thought to minimize the concentration and quantity of solution required to produce endothelial injury. A comparative evaluation of this technique demonstrated enhanced efficacy of treatment regardless of the type of sclerosing agent used.132 In reality, the potential complications of air embolism, as addressed in Chapter 8, are nil. A disadvantage of this technique is that air proximal to the sclerosing solution in the syringe causes compression of the solution, producing leakage of solution from the needle after depression of the plunger has stopped. This may cause extravasation of solution on needle withdrawal.
Radiologic studies have shown air-bolus injections into large varicose veins in the area of the GSV are ineffective in clearing the vessel of blood, even when 0.5 mL of air is injected immediately before the injection of contrast medium.49 In addition, the air inhibits complete and even filling of the varix both proximal and distal to the injection site. In smaller varicosities, injected air forms several bubbles and does not act as a bolus. It also moves independently of the position of the patient and is not totally under the influence of gravity. Therefore, the air-bolus technique may not be advantageous for use in treating varicose veins.
Ultrasound-guided injection
Ultrasound is a useful tool to help visualize injection of a varicose vein in patients who have deeply situated perforator veins, in the obese patient in whom the varicose vein is not easily palpable, in patients with recurrent varicose veins, and in patients with an unusual or complex anatomy that makes finding the point of maximum reflux difficult. Ultrasonic guidance alone does not compensate for lack of dexterity or experience. In fact, injection may be riskier, because of the complex reasons that necessitate its use. Earlier experience with less detailed ultrasound imaging demonstrated multiple complications, with the most severe being arterial injection with loss of significant amounts of tissue (see Chapter 8).133 The use of foamed sclerosant has also decreased the risks.
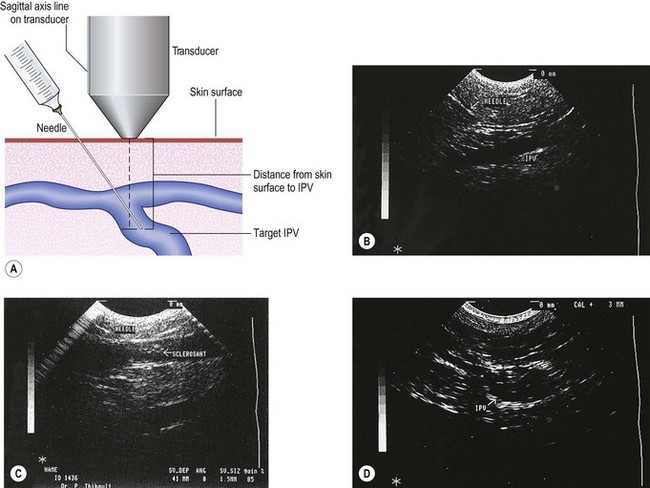
Ultrasound-guided injection was first described in 1989 and is a natural extension of the use of ultrasound in patient evaluation.134–138 The technique for injection is similar to that for standard sclerotherapy except that the needle used is usually longer and of larger a diameter. The author generally uses a 1.5-inch, 22-gauge needle, which is sufficiently large to be echogenic. Smaller needles (25-gauge) could not be easily seen with earlier Duplex ultrasound devices, but with newer high resolution devices even needles of 30-gauge diameter can be visualized.
The needle is introduced into the vein open (not attached to a syringe) to ensure venous placement, because arterial injection must be avoided (Fig. 9.11A) (see Chapter 8). Injection of the foamed sclerosing solution is seen as echogenic flow (Fig. 9.11C). The injection continues until the vein goes into spasm, thrombosis occurs or foam is seen filling the vein (see Fig 9.11D, Figs 9.12 and 9.13).
To provide an even safer method for injection, Grondin and Soriano139 advocate the use of a 20-gauge, 44-mm Teflon or radiopaque catheter to cannulize the vein under ultrasound guidance to further enhance accurate visualization of proper needle placement. Their reported rate of complications in 500 patients is 19.4% postinjection pain, 6.4% superficial phlebitis, and no cases of intra-arterial injection, pulmonary emboli (PE), deep vein thrombosis (DVT), or extravasation necrosis. Parsi and Lim140 also advocate this ‘long line’ echosclerotherapy and comment on the lack of any arterial injection using this technique in their 3-year experience.
Kanter and Thibault141 reported their 2-year experience in treating 202 limbs with ultrasound-guided sclerotherapy. Of these limbs, 23.7% had recanalized at 1 year with no additional veins recurring at 2 years. No complications were reported in their patients. They injected 3% STS in 1-ml increments beginning 3 to 4 cm distal to the SFJ and continued with distal injections every 30 to 90 seconds until persistent vessel spasm occurred or a maximum of 15 mL was injected. This is not possible with foam as the vein will spasm too quickly. Compression with a class II stocking was maintained for 1 week. Two weeks after treatment, any additional nonsclerosed veins were again treated in this manner. For liquid sclerotherapy, the best results were seen in patients treated with larger volumes of STS. Thibault142 followed 35 of his patients for 5 years and noted 25.7% with recurrent veins and 40% with persistent reflux. Thus, duplex-guided GSV sclerotherapy with liquid sclerosing solution is only moderately effective.
Finally, a Doppler ultrasound-guided 18- or 20-gauge (2.75-inch or 1.5-inch, respectively) introducer needle (SmartNeedle, Advanced Cardiovascular Systems, Temecula, Calif.) is commercially available. This device has the proposed benefit of allowing distinction of arterial from venous flow before treatment and has been used to prevent erroneous arterial puncture during placement of a central venous catheter.143
Foam is the best contrast medium for ultrasound-guided injections. Microbubbles are perfect reflectors and when injected into a vein, foam appears as a white cloud responsible for a subjacent black shadow cone (see Fig. 9.9). Being completely opaque to ultrasound it does not allow control on the deeper part of the injection, and in large veins, where foam floats along the more superficial venous wall, some doubt remains regarding appropriate contact of the whole venous wall.
Duplex ultrasound is also useful in assessing the response to initial treatment. When patients return for follow-up examination, duplex evaluation can guide subsequent injections to sections of the vein that have not sclerosed fully or to a previously unrecognized area of reflux. When sclerotherapy is successful, the venous wall appears thickened, particularly at the intimal layer, with ultrasound (Fig. 9.14). The vein is noncompressible. When endofibrosis is subtherapeutic, the lumen is open with partial intravascular thrombosis. These findings indicate the need for a further sclerotherapy injection. Incomplete sclerosis appears as a series of multiple echoes represented as intraluminal white dots.134 Superficial thrombophlebitis appears as an enlarged luminal diameter with minimal parietal changes, partial compressibility, echogenic blood flow, and a lumen partially filled with echogenic material.144
Thibault and Lewis145 found that IPVs are the most common site of reflux from deep to superficial veins in patients with recurrent postsurgical varicose veins. In their series of 122 limbs in 76 patients, after ligation and stripping of the SFJ or SPJ, 71.3% of patients had recurrent incompetent superficial thigh veins in the distribution of the GSV. Thirty-two percent of patients had incompetent veins in the distribution of the SSV. These veins can then be injected with sclerosing solution.138 In this setting, ultrasound-guided injection is particularly helpful, since an obvious varicosity does not always occur over an incompetent perforator.146 In addition, surgical exploration for the perforator in this setting is often difficult.147 Thirty-six patients (38 limbs) with IPVs after surgical stripping were injected with 0.5 to 1 mL of STS 3% under ultrasound guidance.138 Repeat injections were required at 6 to 8 weeks in six patients. Thirty-six of 38 limbs were successfully closed at 6- and 12-month follow-up without notable complications.
Rapid healing of persistent venous leg ulcers with an underlying perforating vein treated with duplex UGFS appears to be effective in producing rapid healing of the ulcers.148 Cabrera et al106 reported that, at 6-month follow-up, 83% of their patients’ ulcers healed after a single ultrasound-guided sclerotherapy treatment with their proprietary foam (Variglobin).
Treatment of a proximal perforating vein with UGFS has also been shown to cause resolution of the associated varicose vein.149
Ultrasound-guided sclerotherapy may also be particularly effective in treating the incompetent SSV. Schadeck150 injected the SSV an average of 3.17 times over 5 years in 74 patients to maintain closure of the vein. Bullens-Goessens et al151 found an enhancement in functional improvement after ultrasound-guided sclerotherapy of the SSV in 11 patients evaluated with air plethysmography.
Doppler-guided injection
Cornu-Thenard152 found that approximately 20% of varicose veins change their position by 1 cm or more when patients move from a standing to a supine position. Therefore, preinjection markings of varicose veins with the patient standing to localize veins that may disappear when the patient lies down are not reliable. Doppler evaluation is important when the patient is supine to ensure accurate needle placement. A multicenter study of this technique in 220 patients with approximately 1400 injections demonstrated successful cannulation in all but 18 injections.153
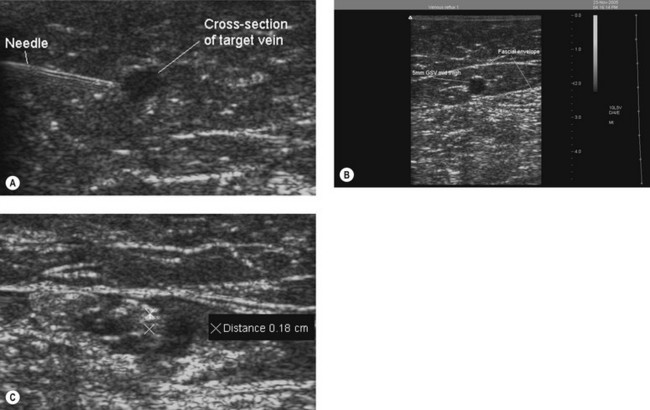
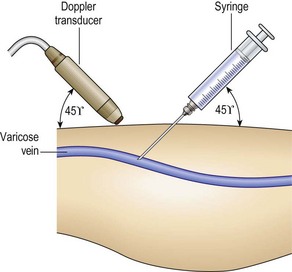
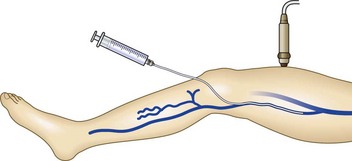
The advantage of Doppler-guided injection is its simplicity. A single operator with practice may perform this technique with one hand holding the needle and the other hand holding the Doppler probe (Fig. 9.15). The ideal vein to treat with this method is palpable standing, measuring 4 to 5 mm in diameter, and impalpable supine.
Endoscopic injection
Venous endoscopy has been reported as being useful when injecting the SFJ or perforator veins but, given the availability of superior duplex ultrasound technology, it is rarely performed.31,154 Van Cleef155 first presented this technique in 1989 for treatment of the GSV at the SFJ. This technique uses an angioscope inserted through an 11-French Seldinger introducing set (USCI-Bard, Billerica, Mass.) while the patient is either standing or in a reverse Trendelenburg position. Endoscopes should have a diameter of 0.85 mm. Irreversible spasm may occur if the introduction occurs with the patient supine.31
Intravascular ultrasound-controlled injection
Intravascular ultrasound (IVUS) provides a unique perspective for evaluating vessel walls before, during, and after therapeutic interventions. Echographic data processing and computerized image manipulation can produce accurate luminal and transmural images of blood vessels. Electronically switched array devices use frequencies of 12 to 25 MHz in 4- to 12-French catheters to produce cross-sectional images of vascular segments. However, with present probes, a bright circumferential artifact known as a ‘ring down’ surrounds the catheter and prevents imaging of structures in the area immediately surrounding the catheter.156
Determining the luminal and vessel wall morphology of normal and minimally diseased vessels, using IVUS produces a dimensional accuracy of 0.05 mm.157–159 This device can visualize calcified and noncalcified arterial lesions and intimal tears or flaps and can distinguish between the media, intima, and adventitial layers of the vessel wall. This technology has primarily been used in evaluating arterial lesions. Future devices may one day combine the benefits of angiography, angioscopy, and IVUS in a single compact unit.
Raymond-Martimbeau160,161 have reported injection through an IVUS probe. This technique allows injection to continue while the vein wall is resonated by the ultrasound probe until sclerosis is visualized by whitening of the entire vein wall (Fig. 9.16). The advantage of this technique is the assurance of complete destruction of the vein wall. The concentration or quantity of solution can be varied until effective endosclerosis is seen. This is rendered unnecessary by foam sclerotherapy.
Raymond-Martimbeau160 performed a study of 25 incompetent sites diagnosed with IVUS and treated with sclerotherapy using liquid iodine sodium iodide in concentrations of 1% to 3% and volumes of 0.25 to 1 ml. In 21 cases (84%), partial echogenic intimal thickening was observed within 1 to 6 minutes (mean, 2.7 minutes). Circumferential intimal thickening became evident within 3 to 26 minutes (mean, 6.2 minutes). The lumen then filled with echogenic material and decreased in diameter. Within 1 week, the treated segment was transformed into a fibrous cord that disappeared completely between 2 and 12 weeks. In four cases (16%), weak or no intimal thickening occurred and the vein recanalized within 2 to 12 weeks. These patients were then treated successfully in a second session. With the use of foam sclerotherapy the advantages of IVUS are diminished, although in the age of liquid sclerosants it was only useful in defining the success of treatment and in ensuring accurate placement of sclerosing solution.
Transcatheter duplex ultrasound-guided sclerotherapy
When liquid sclerosant ultrasound-guided sclerotherapy was challenging for treating GSV reflux at the SFJ junction, a technique of transcatheter duplex ultrasound-guided sclerotherapy was developed by Min and Navarro, who used endovenous transcatheter techniques of vessel occlusion under image guidance (Fig. 9.17).162 Fifty-one GSVs in 50 patients were treated with this technique. With the use of ultrasound guidance and local anesthesia, the GSV was entered 15 to 45 cm (mean, 35 cm) below the SFJ. A 5-French infusion catheter was placed over a 0.035-inch diameter guidewire and positioned under ultrasound guidance 2 to 3 cm below the SFJ. An injection of 2 mL of STS 3% was made in this location, with additional 0.3-mL injections given at 3- to 5-cm intervals as the catheter was withdrawn. The treated leg was then compressed with a class II (30- to 40-mmHg) graduated compression stocking that was worn for a minimum of 7 days, and the patient was instructed to walk immediately. A mean of 4.5 mL (2 to 5 mL) of STS 3% was given in each vein. All veins remained closed at 3- to 12-month (mean, 8 months) follow-up.
Transcatheter duplex ultrasound-guided sclerotherapy represents the use of Seldinger principles in cannulating the GSV for the safe delivery of concentrated sclerosant. This important step helped minimze inadvertent arterial injection with liquid sclerosant. The insertion of a catheter to deliver sclerosing solution is not a new procedure and was described by Rose in 1941.163 Here, the catheter was introduced into the GSV intraoperatively to sclerose the distal GSV after ligation at the SFJ. Use of the ureteric catheter was discontinued in 1945, and the practice of simultaneous sclerotherapy was ended in 1946 with the introduction of a simplified method for ligation of the GSV proximally and distally.
VeinRx infusion catheter
As illustrated in Figure 9.18, the infusion catheter comprises a distal occlusion balloon, fixed infusion length catheter body with infusion holes, and trifurcated hub. Figure 9.19 is a line drawing that further illustrates the catheter design. The FloLock trifurcated hub is designed to connect the following three main systems of the device (Fig. 9.20). A tubing extension incorporating a stopcock on one side of the hub is the port used to inflate and deflate the occlusion balloon. The Luer connection in the center of the hub is used to mount the syringe loaded with the desired sclerosant. Opposite the balloon port and nearest the blue button is a port for controlling the FloLock channel. The FloLock channel allows the physician to determine accurately whether the infusion ports are open or closed (Fig. 9.21), a feature previously unavailable in standard infusion catheters. This channel uses an inflatable elastomeric bladder to either close or open the infusion ports.
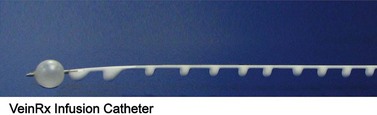
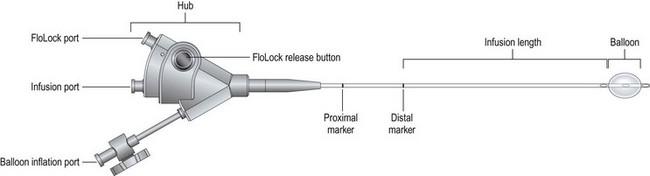
Figure 9.19 Diagrammatic representation of the VeinRx catheter.
(Courtesy VeinRx, Inc., Miami, Fla.)

Figure 9.20 Photograph of the proximal end of the VeinRx catheter showing the infusion ports.
(Courtesy VeinRx, Inc., Miami, Fla.)
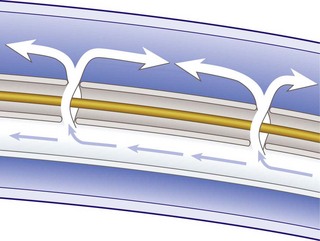
Figure 9.21 Diagram illustrating the effusion of solution from the distal ports on the VeinRx catheter.
(Courtesy VeinRx, Inc., Miami, Fla.)
Treatment of specific problems
Treatment of large-diameter great saphenous veins
The treatment of the GSV with foam sclerotherapy has been discussed and found to be effective depending on the method of foam injection and the concentration and volume of solution. However, almost all of the previously cited studies set an upper limit for the diameter of the GSV to be no more than 8 mm.164 One study used Variglobin 8%–12% (non-foamed since non-detergent) to inject 500 GSVs with diameters of between 6 and 12 mm measured 3 cm distal to the SFJ.165 The authors reported a 22% failure rate irrespective of vein diameter. Barrett et al90 reported outstanding efficacy in GSV with diameters greater than 10 mm injected with foamed STS. This was also found by Valsamis.166 Therefore, proper technique and the use of an appropriate concentration and/or type of sclerosing solution can allow successful treatment of large-diameter GSVs, although length of follow-up must be a critical factors in all of these studies.
Thibault 89 has described a technique for compressing the cannulated GSV with tumescent anesthesia placed in the surrounding facial sheath which may also lead to improved efficacy and reduce recurrences (Fig. 13).
Treatment of vulvar varicosities
A pelvic support device has been developed to compress the vulvar veins (V2-supporter, Prenatal Cradle Inc, Hamburg, Mich.). This device is worn until veins have resolved. Five patients treated in this manner showed no evidence of recurrence in a 1-year follow-up.167 Adverse sequelae have not been noted. A 2-year follow-up of these five patients (and two others) also demonstrated no adverse sequelae and resolution of the varicose veins.168
Treatment of venous malformations (liquid sclerosant)
Venous malformations (VM), as described in Chapter 4, consist of variably sized vessels. Sclerotherapy has proven to be very useful in their treatment. In a study by Yamaki et al,169 28 patients with a variety of VM on the face, neck, extremity, and elsewhere were treated with duplex-guided sclerotherapy with POL 3%. Eighty-two percent of the patients had effective resolution. Pain on injection in 82%, marked swelling in 75%, hemoglobinuria in 14%, and superficial epidermal necrosis in 10.7% were the reported adverse sequelae.
Lee et al170 reported a 92% efficacy in treating 30 patients with a variety of VM with absolute ethanol. Multiple sessions were required and 24 total adverse effects occurred in the 92 sessions given. Adverse effects consisted of nerve palsy in five, ischemic bullae in nine, tissue necrosis in two, tissue fibrosis in two, and DVT in one. The authors proposed that this treatment helps to debulk and stabilize the VM, permitting simpler surgical correction. An additional report on 399 sessions in 87 patients by Lee and colleagues171 showed similar results with long-term efficacy.
Foam sclerotherapy using the Cabrera foam on 50 patients with VM was beneficial in 92% after an average of 12 sessions with a mean of 30 months’ follow-up.172 Of the 46 responders, 18 showed complete disappearance of the VM and 15 showed a reduction of over 50% in size of the VM. Of the 39 patients who reported pain, it disappeared in 25 and was reduced in 14. Three cases of skin ulceration occurred. For more information on foam sclerotherapy in venous malformations, please see the above foam sclerotherapy section.
Treatment of other venous conditions
A variety of other venous conditions have been reported to resolve with sclerotherapy. A report of complete resolution of a venous lake of the lip after two treatments with POL 1%, without adverse effects, has been reported.173
Hemangioma showing late involution was successfully shrunk with an injection of 5% ethanolamine oleate, allowing surgical excision.174
Multiple hereditary glomangiomas were treated with 0.2% to 3% STS, depending on the size of the lesion.175 An average of two treatments where the lesions were injected with 0.5 to 1 mL of solution was required for lesion improvement.
Treatment of pyogenic granuloma with 5% monoethanolamine oleate in nine patients, who were all injected once, resulted in complete resolution of the lesion within 2 weeks.176 An additional study on 15 lesions in 14 patients treated with 0.5% STS (0.15–2 mL) one to five times (mean, 2.2) showed complete resolution in 12 lesions.177 No adverse effects were seen in any patient.
Treatment of recurrences
When unsuccessful or in case of recurrence, sclerotherapy does not modify the initial, pretherapeutic varicose pattern, which reappears as it was before or smaller. This is not the case with surgery, and, very often, recurrent varices after surgery (REVAS) are extremely difficult to manage.178 Therefore, if surgery can be, in certain selected cases, considered as an alternative treatment after sclerotherapy failure, sclerotherapy is the usual and most appropriate recourse for recurrence after surgery of varicose veins. The progress in ultrasound guidance and, most of all, the use of foam sclerosing agents have revolutionized the approach to this difficult problem.
As stated in the REVAS consensus document,178 all recurrences must be completely assessed by duplex in order to map all leaks and refluxes. After surgery of junctions, two types of recurrence can be observed:
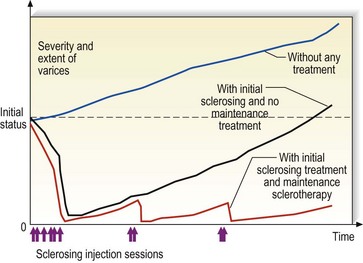
For most patients, the difference between ‘new veins’ and ‘recurrent veins’ is not obvious at all and this misunderstanding is likely to create some difficulties in doctor–patient relationships. A simple diagram explaining evolution of varicose veins with or without treatment can be extremely useful (Fig. 9.22; also see Case Study 13 later in this chapter).
Does the Menstrual Cycle Influence Sclerotherapy?
The actions of estrogens and progestins on venous distensibility were discussed previously (see Chapters 3 and 4). Theoretically, sclerotherapy should be performed when the venous system is in its most contracted state so that post-treatment thrombosis is minimized. Since limb volume and venous distensibility are at their least during and just after menses and at their highest during ovulation, the optimal window for sclerotherapy treatment is when estrogen levels are lowest.179 However, until appropriate studies are performed to test this hypothesis, no absolute recommendation can be made.
Recommended Sclerosing Solution Amounts and Concentrations for Non-Foam Sclerotherapy
The first principle of determining solution amounts and concentrations is that the concentrations should be strongest at the highest point of reflux. With saphenofemoral reflux, the concentration should be strongest at the upper thigh and weakest at the ankle. With ankle or calf perforating veins, the concentration should be highest at the perforator. For example, Vin180 recommends that 1 mL of STS 1.0% be used at the proximal thigh, 0.5 mL of STS 1.0% be used at the medial thigh, and 0.3 mL of STS 0.5% be used at the medial knee to treat a moderately sized varicose vein.
The second principle, as described by Tournay in 1949, is: ‘It is not the concentration of the sclerosing agent in the syringe that matters, but the concentration within the vein.’181 The importance of this statement was discussed in Chapter 7. In short, for sclerotherapy to be effective, the entire vein wall must be damaged and the entire intraluminal volume of the segment of the vein must be destroyed. This is important because the smooth muscle portion of the vein wall theoretically can regenerate endothelium, and endothelial cells can migrate long distances to re-establish a functional conduit. Sackmann182 expanded on this principle by demonstrating in polyvinyl tubes the local conditions of ‘time and space’ regarding contact of the sclerosing solution with the vessel wall were also important. He showed the zone of contact diminishes as the caliber of the vessel increases. In tubes with a diameter of less than or equal to 4 mm, the liquid flowed in a laminar fashion. In tubes with a diameter of greater than or equal to 8 mm, turbulent flow was produced. In tubes 6 mm in diameter, a mixed flow occurred, with a transition between a laminar and turbulent appearance (Fig. 9.23). In contrast, the caliber and position of the needle, the speed of injection, and the viscosity of the solution did not seem to influence the time of contact of the sclerosing solution with the tube.

Green183 used Poiseuille’s formula to describe resistance to fluid flow in a varicose vein:
where
From this formula it is apparent that the most important factor in determining resistance of flow is the vessel diameter (radius). At the point of injection into an empty vein, expected flow of sclerosing solution would be nonlaminar (Fig. 9.23). This may account (along with increased localized concentration; see the following paragraph) for a greater incidence of vessel damage and blowout at the point of injection (see Chapter 8). Nonlaminar flow also occurs downstream of injection in an empty vein in which resistance is still high, since the pressure generated by the physician on the syringe plunger is much greater than intravascular pressure, which would approach zero in an empty vein, especially if the limb were elevated (Fig. 9.24).184
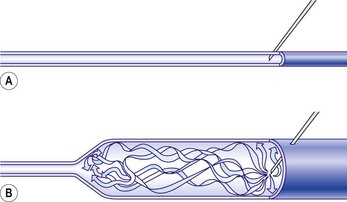
Guex184 has worked out that the concentration of sclerosing solution can be calculated based on the diameter of the vein by the following formula:

where
Thus, if 0.5 mL is injected into a varicose vein 2 mm in diameter, the sclerosing solution will fill a 16-cm length of vein. In reality, the concentration of sclerosing solution at the injection site is maximal and decreases with distance from each point when small volumes of solution are injected (Fig. 9.25). The concentration of sclerosing solution along the entire course of the vein can be equalized either by injecting a larger volume in a single site or by injecting small volumes in multiple sites (Figs 9.26 and 9.27).
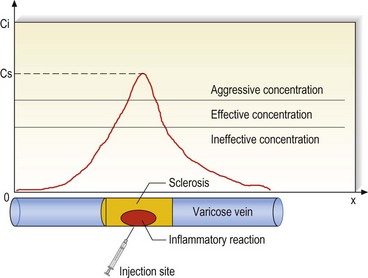
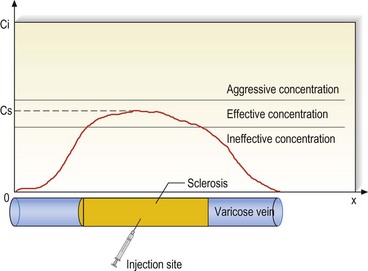
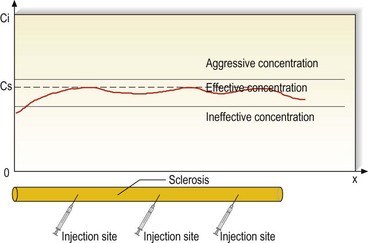
A study by Cornu-Thenard185 suggests the following sclerosing concentrations for varicosities of various diameters:
He recommends 0.5-ml injections be placed every 6 to 10 cm along the varicose vein. Additional recommended concentrations for injection of other sclerosing solutions into various types and diameters of vein can be found in Chapter 7.
The third principle is the amount of sclerosing solution injected into a single site should not be more than 1.0 mL (usually 0.5 mL). Venographic studies of direct injections into varicosities of the leg have demonstrated that if more than 1.5 mL of solution is injected at a single site, it is likely to spill over into the deep veins.49,186 In addition, the patient should not move the leg for a few minutes so that the sclerosing solution can remain in contact with the varicose vein, because any movement of the leg will rapidly move the sclerosing solution into the deep venous system.
Some physicians do not limit the volume of sclerosing solution at a single site.187 Green187 reports infusing from 3 to 12 mL of STS into each injection site. Concentrations ranged from 0.75% to 3.0% depending on vein size. He reports treating more than 3000 patients in this manner without encountering a single case of DVT. He also reports enhanced efficacy with this technique, having near 100% efficacy with follow-ups of up to 5 years. He uses class II compression for 2 to 8 weeks. Other details of his technique are not specified. Green claims that ‘the widely varying success rates reported in the literature are usually a reflection of the technique of the practitioner and not any inherent limitation of the procedure.’ The authors believe that this statement is somewhat correct but still caution against the use of excessive volumes of sclerosing solution in a single site, since many cases of DVT have been reported by other reputable physicians (see Chapter 8).
Histologic examination of peripheral veins may provide assistance in determining the optimal concentration of sclerosing solution. Corcos et al188 have determined through biopsy of the dorsal pedal vein that the degree of intimal thickening, ectasia, muscular hyperplasia, medial fibrosis, fragmentation, and dissociation of the internal elastic membrane and intimal fibrous plaques correlate with the concentration of sclerosing solution necessary to effect endosclerosis of varicose veins. This finding is supported by the theory that varicosis is a systemic disease (see Chapter 3).
The use of foam has very much simplified the approach of concentration and the current trend is to decrease the concentration in half when using foam as opposed to liquid sclerosing solution. Guex62 has suggested the values shown in Table 9.7, which remain open to adaptation and discussion.
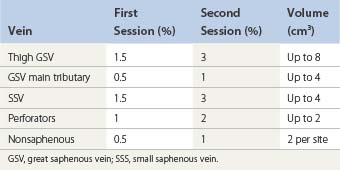
Postsclerotherapy Compression
Postsclerosis compression is perhaps the most important advance in sclerotherapy treatment of varicose veins since the introduction of relatively safe synthetic sclerosing agents in the 1940s. Primarily, compression eliminates a thrombophlebitic reaction and substitutes a ‘sclerophlebitis’ with the production of a firm fibrous cord.12 The advantages of postsclerotherapy compression are discussed in detail in Chapter 6.
In addition to providing external compression to the treated vessel, one should try to minimize forces that act to distend the vessel. Since taking hot baths or saunas dilates the cutaneous venous network, they should be avoided for 2 to 6 weeks after sclerotherapy or until such time as the treated vessel is fully sclerosed. In addition, any activity that increases abdominal pressure may act to force blood in a retrograde manner through the SFJ or IPVs, producing venous dilation. Heavy weight lifting therefore must be discouraged, along with any exercises that use the abdominal musculature, unless the legs are elevated during abdominal exercise. One such activity that increases abdominal pressure by approximately 22 mmHg is running, with pressure apparently being produced to splint the trunk and pelvis.189 Therefore, aerobic exercises, jogging, and running should be limited for 1 to 2 weeks.
Patients should be examined 2 weeks after injection so any area of thrombosis can be evacuated early.190 Each individual area should not be treated again sooner than 6 to 8 weeks after initial injection in order to allow adequate healing between treatments.
Contraindications to Treatment
Knowing and applying contraindications to sclerotherapy is an important part of phlebological practice. The principle of precaution is increasingly applied when using a treatment or a drug – when its use has not been specifically determined, registered, and officially approved, its use is unlawful. Official contraindications are very often unclear, false or inaccurate, outdated, or worse. Contraindications should remain under medical control and managed by specialists.191
Pregnancy
Besides the risk of absorption of the sclerosing solution by the fetus, pregnancy is associated with dilation of the entire venous system through multiple mechanisms that do not normalize until 3 months postpartum (see Chapter 3).192,193 Therefore, although sclerotherapy can be and has been performed successfully by many physicians on pregnant women,194–198 the increase in venous distensibility counteracts the desired contraction of the treated varicose vein (see Chapters 3, 4, and 8). Finally, varicose veins may decrease in size and disappear after delivery (see Chapters 3 and 4).199 Thus, waiting may eliminate the need for the procedure.
One situation that may justify sclerotherapy during pregnancy is the presence of significant and painful vulvar varicosities, which develop in approximately 2% of pregnant women.200 They usually occur by the second trimester and are more likely in multiparous women. Although they rarely thrombose, they are painful, especially with walking. Bed rest, leg elevation, and localized compression are usually effective in alleviating symptoms, but sclerotherapy may be necessary in severe cases.
Venography has shown that vulvar varices arise from any combination of the following: obturator vein; internal pudendal vein; inferior gluteal vein; external iliac, uterine, and ovarian veins; obturator vein; presacral veins; common femoral vein; and the GSV.201,202 Because of this variable and extensive system of reflux and the thin-walled, fragile nature of these veins, sclerotherapy is preferred over surgical excision or avulsion (see Case Study 7 later in this chapter).
Inability to ambulate
A corollary to the contraindication just mentioned is the performance of sclerotherapy during surgical ligation. Although this procedure has been performed by many surgeons and was advocated by de Takats in 1930,203 it was usually limited to a point distal to the SFJ on the GSV and therefore was performed on an ambulatory basis. In 1934, Faxon204 modified this technique to include ligation at the SFJ with retrograde injection of the GSV. He achieved good results (although follow-up was poor) in his series of 117 cases except for one case of fatal PE, which was attributed to faulty technique by a resident surgeon. In more recent times, Conrad205 reports great success with this technique when used in conjunction with ligation at the SFJ. Hubner206 reported similar success without mention of complications in 413 patients followed for more than 1 year. Patients treated with POL 4% had an 83% success rate, whereas patients treated with Variglobin 4% had a 94% success rate. However, Hubner separates the two procedures by a few hours to a day because his patients had the ligation performed by a surgeon in a separate office and return to him for sclerotherapy. This latter scenario ensures that the patient is ambulatory for both procedures.
In spite of the above-mentioned successful results, there are potential complications that call for separating the two procedures. First, many varicose veins will resolve after surgical treatment of the high-pressure reflux points, so subsequent sclerotherapy is minimized or not necessary.207 Secondly, the surgical period is often one of minimal ambulation because of postoperative pain and the use of general or regional anesthesia. The delay in adequate ambulation may allow the sclerosing solution to migrate to the deep venous system where unwanted damage could occur (see Chapter 8).200 The authors recommend postoperative sclerotherapy be delayed for 2 to 3 weeks.
History of thrombophlebitis and deep vein thrombosis
Patients with a history of certain venous diseases may be predisposed to the development of excessive thrombosis with injection of a sclerosing agent (that is, development of an excessive phlebitic reaction; see Chapter 8).
Patients with low-risk thrombophilia (activated protein C resistance, hyperhomocysteinemia especially, factor II, factor V Leiden) can be treated with sclerotherapy. A prospective study in progress will determine the best prophylaxis (see Chapter 8).
Another simple test to determine if the varicosity resulting from DVT is a necessary conduit is a modification of the Perthes’ test (see Chapter 5). A tensiometer cuff is inflated to 110 mmHg, and the patient is asked to walk quickly for 5 minutes. If the patient complains of heavy pain, or if the leg becomes livid, or both, the varicosity is necessary as a collateral channel. This test has allowed, without complication, surgery on 53 limbs with varicose veins in 52 patients with prior DVT.208
Allergic reaction
Patients are rarely allergic to a sclerosing solution, but a different solution can usually be substituted. If the allergic reaction consists of generalized urticaria, with or without an erythematous papulosquamous appearance, French authors advocate continuing treatment with the offending sclerosing solution with the addition of antihistamines before and after treatment (see Chapter 8).209
Infrequently, patients develop periorbital edema and a maculopapular cutaneous eruption even with the use of unadulterated hypertonic saline solutions. In this case, ‘allergic reaction’ may be the result of histamine release by intravascular basophils or perivascular mast cells that are directly damaged by the sclerosing solution (see Chapter 7).210 Under this circumstance, administration of antihistamines before and after the procedure appears safe while therapy is continued.
Patients taking tamoxifen
As described in Chapter 8, tamoxifen is often responsible for extensive superficial phlebitis in patients treated by sclerotherapy, even of reticular or spider veins. We consider it to be a relative contraindication.
Case Histories
The following case histories demonstrate the authors’ technique of sclerotherapy for different varicose veins (Box 9.1).
Case Study 1 Incompetent perforator veins treated with Fegan’s technique
A 35-year-old woman developed varicose veins during the second trimester of her second pregnancy and wore an over-the-counter light compression stocking during the remainder of her pregnancy. At delivery she developed thrombophlebitis that was treated with hot packs only. She came for evaluation and treatment 6 months after delivery. Physical examination showed a 4- to 6-mm varicose tributary of the GSV originating at the medial midthigh and extending to the medial calf with continuation across the anterior tibia (Fig. 9.28A and B). Venous Doppler examination revealed a continuous venous sound with distal augmentation at the level of the posterior tibial vein at the left ankle. There was no evidence of saphenofemoral reflux or other abnormalities. Photoplethysmography revealed a normal venous refilling time in the right leg and an abnormal refilling time in the left leg (20 seconds). The venous refilling time normalized with placement of a tourniquet at the level of the left upper calf and left lower thigh. Therefore, the physical and noninvasive examinations were consistent, showing incompetence of the midthigh (Hunterian) perforator.
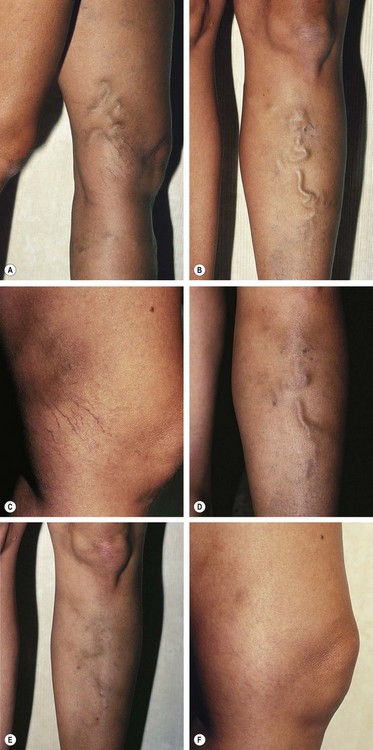
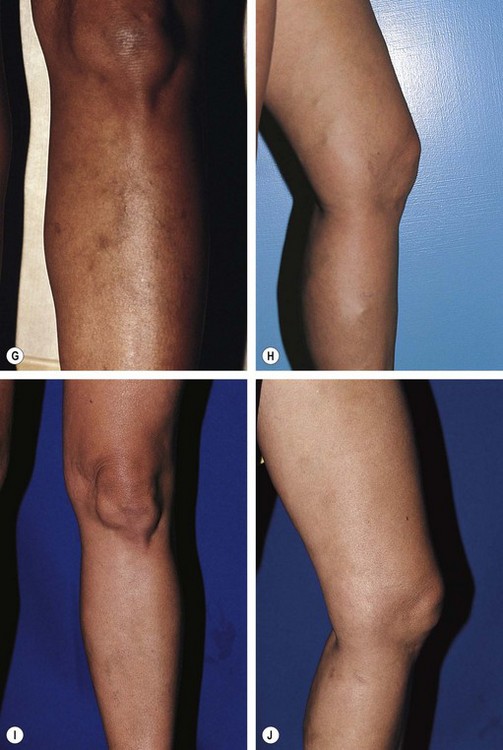
The patient was seen 2 weeks later, at which time physical examination revealed total resolution of the varicosity at the midthigh (Fig. 9.28C) and persistence of a thrombosed varicosity at the anterior tibial level (Fig. 9.28D). It was drained, and the pressure stocking was prescribed for use while the patient was ambulatory for another week. On follow-up examination 6 weeks later, the vessel had resolved (Fig. 9.28E). One-year follow-up demonstrated total obliteration of the varicosity and post-treatment hyperpigmentation (Fig. 9.28F and G). This case illustrates Fegan’s principle that interruption of the IPVs alone causes normalization of the entire varicose vein.
One year later (2 years after her initial sclerotherapy), the patient became pregnant with her third child and noted the development of new varicose and telangiectatic leg veins during her first trimester. Despite wearing 30- to 40-mmHg graduated support stockings for much of her pregnancy, she developed incompetence of the SFJ bilaterally, with new incompetent GSV bilaterally and new vulvar varicosities. Interestingly, the previously sclerosed veins just above the medial knee and on the anterior tibial surface did not reappear (Fig. 9.28H and I). Ligation and stripping were performed 18 months postpartum when breastfeeding was discontinued, followed 2 weeks later with sclerotherapy of reticular veins, with excellent results (Fig. 9.28J).
Case Study 2 Incompetent perforator vein at the midcalf treated with modified Fegan technique
A 40-year-old woman noticed the gradual development of a varicose vein over 4 years without any predisposing factors. Physical examination showed a varicose tributary of the GSV 3 to 5 mm in diameter extending from the midanterior tibial surface to the medial calf and thigh and ending in the lower anterior thigh (Fig. 9.29A and B). Venous Doppler xamination was remarkable only for an IPV at the right midmedial calf.
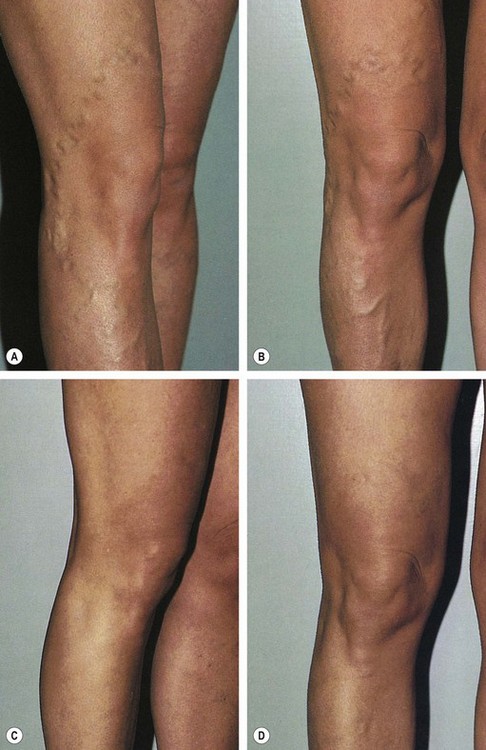
Since fascial depressions could not be felt, the classic Fegan technique could not be performed. Therefore, 25-gauge butterfly catheters were placed randomly into the varicosity at the level of the anterior midtibia, medial superior tibia, and the lateral knee with the patient standing. After the patient assumed the supine position, STS 0.5% was injected into these sites after proper needle placement was confirmed with blood aspiration. A total of 0.5 mL was injected at the anterior midtibia, 1 mL at the medial superior tibia, and 2 mL at the lateral knee while pressure was maintained on the vein proximally. STD E-foam pads were placed over the entire vessel and were secured with Coban tape applied with moderate pressure. A 30- to 40-mmHg graduated compression stocking was applied, with two stockings worn on top of each other while the patient was ambulatory and one stocking worn at night for 1 week. During the second week, the dressing was removed, and the graduated support stocking was worn for another week only while the patient was ambulatory. The varicosity was completely resolved on follow-up examination at 2 weeks, and a few thrombi were drained. The photographs in Figuse 9.29C and D were taken 11 months after treatment.
Case Study 3 Reticular varicosities without perforator vein reflux treated with total-vein sclerotherapy (Sigg’s technique)
A 34-year-old woman first noticed the appearance of varicose veins with her second pregnancy, 3 years before treatment. The veins were symptomatic after prolonged standing and were thought to have enlarged over the past year. Physical examination showed a set of 3- to 4-mm varicose reticular veins coursing from the posterior midthigh to the posterior midcalf bilaterally (Fig. 9.30A and B). There was no evidence of incompetence in either the perforator veins or the SFJs on venous Doppler examination.

While the patient was lying horizontal on her abdomen, multiple injections of STS 0.5% were made into the varicose veins. Approximately 0.5 mL was injected into each site every 4 to 6 cm for a total of 8 mL of solution per leg. Continuous compression was maintained for 7 days only with 30- to 40-mmHg graduated compression stockings overlying STD E-foam pads over the varicose veins. Follow-up examination did not disclose excessive bruising or pigmentation. No thrombosis occurred. Figure 9.30C and D, shows the appearance of the treated vessels at 1-year follow-up.
Case Study 4 Posterior thigh varicose GSV tributary associated with an incompetent SFJ treated with sclerotherapy alone using the air-bolus technique
A 36-year-old woman developed a varicose vein during her second pregnancy, 3 years before evaluation and treatment. The vein was symptomatic during prolonged standing, and she reported associated ankle edema. Physical examination showed a 5- to 8-mm diameter varicose vein coursing from the midposterior thigh to the midcalf (Fig. 9.31A). Venous Doppler examination demonstrated gross incompetence of the right SFJ and a positive Trendelenburg test in the lower thigh. The remainder of the examination was normal.
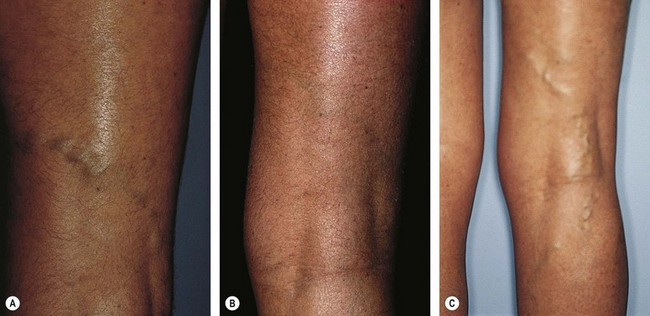
Surgical ligation and limited stripping were recommended, but refused by the patient. Therefore, sclerotherapy of the involved varicose vein was performed using an air-block technique. The air block was used in an attempt to concentrate the sclerosing solution in the injection site without dilution or inactivation of blood. Butterfly needles, 25-gauge, were placed in the vein at areas of fascial depression – two sites on the thigh and one site on the calf – while the patient was standing. These areas were found by venous Doppler ultrasound not to represent IPVs. With the patient lying horizontal with the leg elevated to 45 degrees, 1 mL of STS 1.0% was injected into each site after injection of 0.5 mL of air. STD E-pads were immediately placed and secured with Microfoam tape, and a single 30- to 40-mmHg graduated compression stocking was worn continuously for 2 weeks. Follow-up examinations at 2 and 6 weeks showed persistent resolution of the vein with a slightly palpable cord. A small amount of coagula was drained at 6 weeks. The vein remained fibrosed 2 years after treatment (Fig. 9.31B).
Treatment in the patient consisted of a modified Fegan and Sigg technique. The entire varicosity was obliterated using fascial depression areas as injection sites. The French technique with injection of sclerosing solution into the SFJ could have been used. However, this procedure was not performed because of the unavailability of Variglobin. Alternatively, STS 3% could have been injected under duplex control at the SFJ. Refer to the articles by Raymond-Martimbeau34 and Schultz-Ehrenburg et al40 for a description of these latter techniques.
The patient returned 8 years later (10 years after initial treatment) with recurrence of the varicose vein as well as new distal extensions to it (Fig. 9.31C). The vein had slowly recurred over the past year. Venous Doppler examination demonstrated Valsalva-positive reflux into the GSV through the SFJ. The patient will now undergo endovenous RF closure of the GSV with distal ambulatory phlebectomy.
Case Study 5 Incompetent GSV varicose tributaries treated with total-vein sclerotherapy alone
A 31-year-old woman noted the onset of varicose veins over the right lower leg at 10 years of age. With each of her succeeding three pregnancies, the veins enlarged and became more painful while she was standing. Physical examination showed a clustered varicose vein 5 to 10 mm in diameter over the right anterior and medial calf (Fig. 9.32A). Venous Doppler examination demonstrated marked reflux of the right GSV throughout the varicosity.
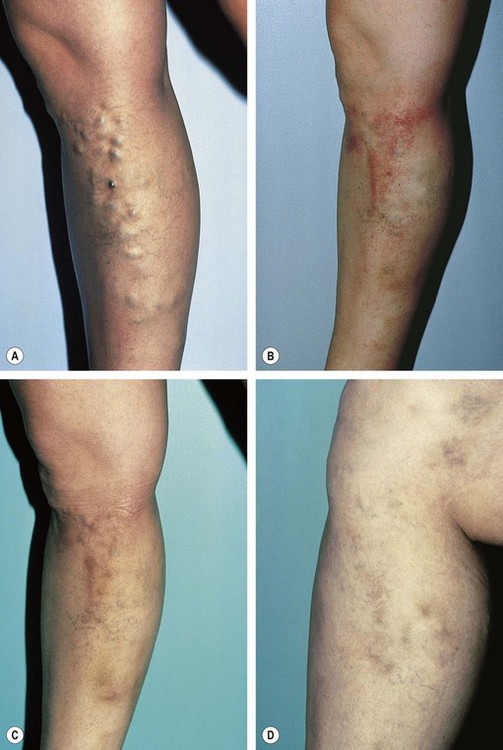
The patient refused surgical ligation and limited stripping. Therefore, sclerotherapy with STS 1.0% was performed while the patient was horizontal. One milliliter of solution was slowly injected at each of nine separate locations, followed by application of STD foam pads and a double layer of 30- to 40-mmHg graduated compression stockings, which were worn continuously for 2 weeks while the patient was ambulatory. One stocking was removed while she was sleeping. A mild phlebitic reaction was clinically apparent 2 weeks after injection (Fig. 9.32B), and compression was maintained for another 2 weeks. Four weeks after the first injection, multiple thrombi were drained from the medial calf, and two more injections of STS 1% (1 mL each) were made into persistent varicose dilations on the medial and anterior superior calf (Fig. 9.32C). At 1-year follow-up the leg remained pain free and showed persistent resolution of the treated veins (Fig. 9.32D). Venous Doppler examination disclosed an incompetent, 4-mm-diameter varicose vein just below the right anterior tibia and another incompetent varicosis over the inferior midposterior calf. These veins were successfully sclerosed with STS 1%. At 2 years follow-up, multiple new varicosities became apparent after resolution of sclerotherapy-induced hyperpigmentation. The patient has remained pain free and is very happy with the results of treatment. Her wish is to continue sclerotherapy treatment, even with the understanding that new or recurrent varicose veins may occur later.
Case Study 6 Incompetent perforator vein underlying ankle ulceration
A 27-year-old woman sought treatment after a 3-year history of cutaneous ulceration over the right medial mallear region (Fig. 9.33A). The patient had been seen previously by a physician from the infectious disease service and was prescribed multiple courses of systemic antibiotic treatments that did not produce significant change in the appearance of the ulceration. She was also evaluated by a physician in the plastic surgery department and had been treated with the placement of full-thickness pinch grafts, which did not heal. Physical examination was remarkable for pedal edema extending to the midcalf and associated truncal varicosities. Venous Doppler examination demonstrated a normal deep venous system and saphenofemoral and popliteal junctions and an IPV at the base of the ulcer (marked X in Fig. 9.33A). The perforator vein was injected through the ulcer. A 23-gauge butterfly needle was inserted into the perforator vein while the patient was standing, and the leg was elevated while the patient reclined. STS 1.0%, 1 ml, was slowly injected while the leg was blocked proximally and distally with hand pressure 3 cm in either direction. Immediately afterward, compression was applied with an STD foam pad under Microfoam tape and two 30- to 40-mmHg graduated compression stockings. The stockings were worn for 2 weeks. Double stockings were worn during the day, and the outer stocking was removed when the patient was supine.
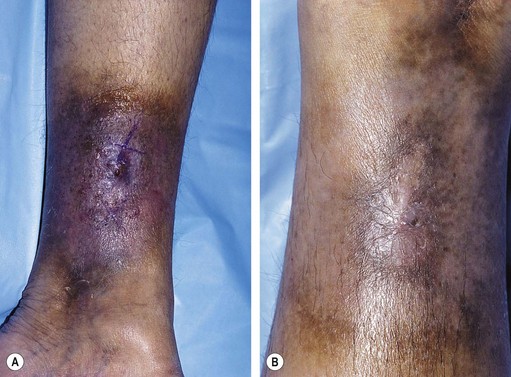
Follow-up examination at 3 months showed complete healing of the ulceration and resolution of associated venous stasis changes (Fig. 9.33B). The patient remained free of ulceration 2 years after treatment.
Case Study 7 Sclerotherapy of vulvar varicosities
A 40-year-old woman developed vulvar varices with her first pregnancy at age 18. She noted aching and pelvic fullness during her menstrual period and when standing for prolonged periods of time. Physical examination showed a prominent varicose vein 6 to 8 mm in diameter extending from the vulvar region into the GSV. The vein was incompetent throughout its entire length from the midposterior calf to the most superior aspect of the vulva, according to venous Doppler examination. Two IPVs underlying fascial defects were present at the medial knee and midposterior calf. There was no evidence of incompetence with the Valsalva maneuver. Her SFJ was competent according to venous Doppler examination. Scattered reticular veins 3 mm in diameter were noted on the anterior thigh. Scattered venules 0.4 mm in diameter were present on the anterior and lateral calf. The opposite leg was free of varicose or telangiectatic veins (Fig. 9.34A).
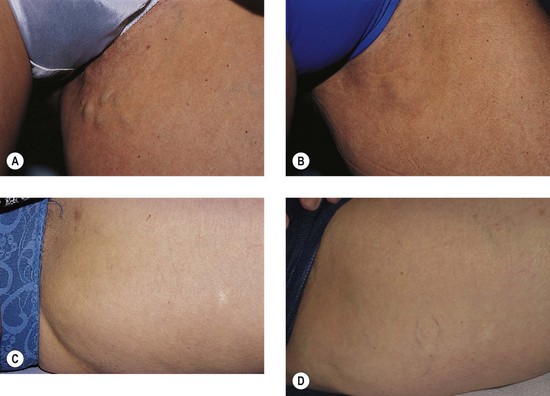
With the patient lying in a slight reverse Trendelenburg position, a total of 2 mL of STS 1.5% was injected into the two perforator veins at the medial knee and posterior calf. These areas were immediately compressed with an STD E-foam pad and Microfoam tape. A total of 4 mL of STS 1.0% was injected into the network of vulvar and superior thigh varicosities, and a figure-of-eight wrapover foam pad was used to compress the vulvar varices. This was followed by injection of 4 mL of STS 0.5% into the remaining reticular veins and venulectases. A 30- to 40-mmHg graduated thigh-high compression stocking was worn continuously for 7 days. When the patient returned 1 month later, all veins were sclerosed and without audible flow during venous Doppler examination. Multiple coagula were drained through 22-gauge needle punctures. Clinical appearance 2 months after treatment was excellent (Fig. 9.34B). Clinical appearance 3 and 19 years after treatment was still excellent, with the patient showing no evidence of recurrence in any of the treated veins (Fig. 9.34C and D).
Case Study 8 Large varicose vein from incompetent perforator veins
After her second pregnancy, a 40-year-old woman developed varicose veins in the left lower leg, which increased in severity with her third pregnancy. Six years after her second pregnancy she developed pain in the left calf with associated leg swelling. The pain increased with exercising and resolved with leg elevation. She also complained of resting pain and a generalized tired feeling in the leg. There was a positive history of varicose veins in her mother. Photoplethysmography was normal, with a venous refilling time of 43 seconds and good calf muscle pump function. Venous Doppler examination demonstrated two IPVs at the left lateral knee and left medial posterior thigh without reflux from the SFJ. The vein measured 8 to 10 mm in diameter (Fig. 9.35A).

 years after sclerotherapy treatment. D, No evidence of recurrence 8 years after initial treatment.
years after sclerotherapy treatment. D, No evidence of recurrence 8 years after initial treatment.The patient was treated with a Fegan–Sigg technique. A 25-gauge butterfly needle was placed just distal to each of the two perforator veins, and the leg was elevated 45 degrees. A total of 2 mL of STS 1% solution was injected, with the perforator points rapidly compressed with STD foam pads and Microfoam tape. An additional 1.5 mL of STS 1% was injected into distal aspects of the varicose vein in three separate sites. A double layer of 30- to 40-mmHg compression stockings was worn while she was ambulatory for 1 week, with the outer stocking removed when she was supine. A single 30- to 40-mmHg stocking was worn for an additional 2 weeks only while she was ambulatory. Thrombus was drained 2 weeks later, and an additional 1 mL of STS 1% was given to a nonsclerosed segment of the vein. Six weeks after the first injection session, the vein was entirely sclerosed and additional coagula were drained (Fig. 9.35B). She remained symptom free without evidence of recurrence  years after the first injection session (Fig. 9.35C) and continues to remain symptom free without evidence of recurrence 8 years after the initial treatment (Fig. 9.35D).
years after the first injection session (Fig. 9.35C) and continues to remain symptom free without evidence of recurrence 8 years after the initial treatment (Fig. 9.35D).
Case Study 9 Extensive varicosities of GSV and GSV tributaries
A 56-year-old woman noted the development of varicose veins during her second pregnancy at age 30. They were entirely asymptomatic, and she was seen initially for cosmetic treatment. There was a family history of varicose veins in her father. Physical examination showed a dilated GSV 6 mm in diameter with vulvar varices 4 mm in diameter and an anterior saphenous varicosity 6 mm in diameter. All varicose veins were incompetent throughout their length as demonstrated by venous Doppler examination but without Valsalva-induced reflux and without reflux across the SFJ (Fig. 9.36A and B).
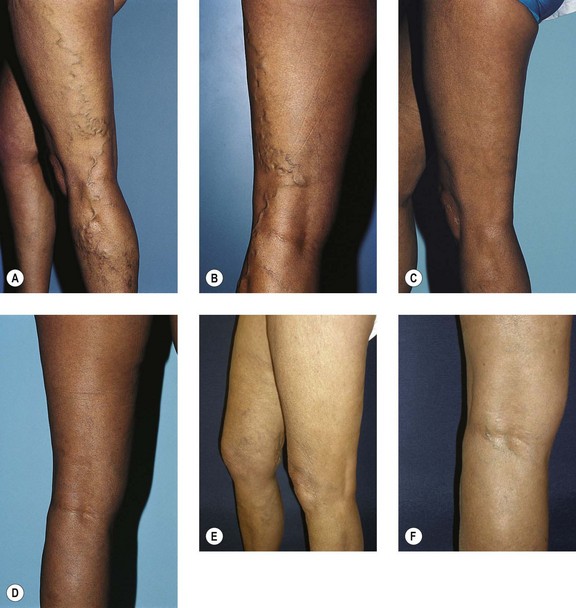
With the patient supine, the entire varicose system was treated using a total of 11 mL of STS 1%. A double layer of 30- to 40-mmHg graduated compression stockings was worn during the day, with the outer stocking removed at night, for 1 week. A single 30- to 40-mmHg stocking was worn during the day for the second week. Six weeks later, reticular veins 2 to 3 mm in diameter were treated with a total of 4 mL of POL 0.75% and telangiectasia was treated with a total of 10 mL POL 0.5%. One year later, additional reticular veins were treated with 8 mL of POL 0.75% and telangiectasia was treated with 4 mL of POL 0.5%. Figure 9.36C and D shows the clinical appearance 2 years after initial treatment, with resolution of all varicose, reticular, and telangiectatic leg veins. Appearance 8 years post sclerotherapy (Figure 9.36E, F).
Case Study 10 Development of SFJ incompetence after initial successful treatment of varicose GSV and tributaries
A 34-year-old woman was seen initially at age 27 years with the development of painful varicose veins during her first of four term pregnancies. The varicosities increased in size during each pregnancy, with the largest increase during her second pregnancy. The leg pain was throbbing, especially just before menses, with resolution 3 days into her menstrual period. Throbbing was relieved with leg elevation or by wearing graduated compression stockings. The family history included varicose veins in her mother, aunt, and sister. Physical examination showed a 6-mm-diameter incompetent GSV with an incompetent midthigh (Hunterian) perforator vein without Valsalva-induced incompetence. The SFJ was competent (Fig. 9.37A and B).
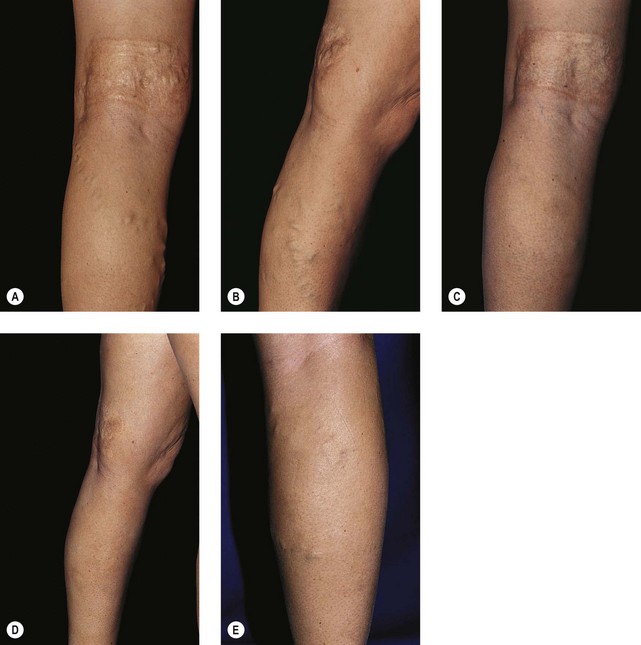
With the patient supine, the varicose veins were injected with 2 mL of STS 1% just distal to the midthigh (Hunterian) perforator vein, followed by a total of 16 mL of STS 0.5% to the remaining varicosities, with approximately 0.5 mL injected every 5 cm or so. A double layer of 30- to 40-mmHg graduated compression stockings was worn for 1 week while the patient was ambulatory, with the outer stocking removed when she was supine; a single stocking was worn for a second week when she was ambulatory. The patient became completely asymptomatic 1 month after the first sclerotherapy treatment (and remained so 3 years later). Nine months later, an additional 16 mL of STS 0.5% was injected into multiple varicose and reticular veins that had not resolved or were newly present, followed by an identical post-treatment compression regimen. One year after the second sclerotherapy treatment, all visible varicose and reticular leg veins resolved completely (Fig. 9.37C and D). Despite no new predisposing factors, new varicose veins were noted 3 years after the first sclerotherapy session. At this time, the SFJ was incompetent bilaterally to venous Doppler examination and the patient was referred for ligation and stripping of the GSV at the SFJ bilaterally (Fig. 9.37E and F).
Case Study 11 Symptomatic clinically inapparent varicose vein treated with duplex-controlled sclerotherapy
A 60-year-old woman was seen initially with a complaint of pain in the medial knee and calf area for the last 6 months. She had undergone ligation and stripping of the GSV from the SFJ 30 years previously for treatment of varicose veins that occurred during her only pregnancy. Clinical examination did not disclose visible varicose or reticular veins. A color-flow duplex Doppler examination showed normal common femoral and superficial femoral and popliteal veins without evidence of acute or chronic DVT. The deep venous system was without evidence of reflux. An atypical vein was present 5 to 6 cm distal to the area of the SFJ as a remnant or duplicate GSV that coursed down the medial aspect of the thigh, terminating in the area of symptomatology. The vein was markedly incompetent to Valsalva maneuver and thigh and calf compression, and communicated with numerous perforator veins along its course (Fig. 9.38A and B).
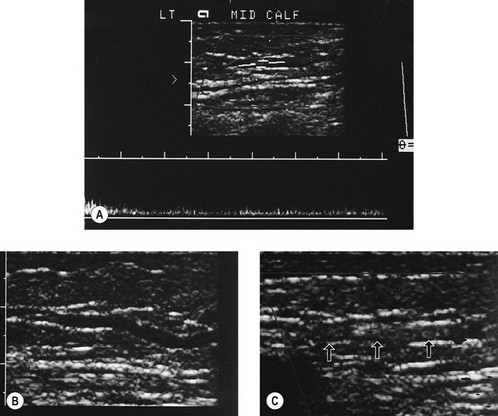
Under duplex guidance, 1 mL of STS 3% was injected into the medial thigh varicosity through a 22-gauge needle. Correct position was verified by open-needle insertion. The injection was given slowly until the vein thrombosed (Fig. 9.38C). An STD E-foam pad was placed with Microfoam compression, and additional injections were given to two additional perforator veins present in the area of greatest symptomatology. The entire procedure was performed with the patient supine. A double layer of 30- to 40-mmHg graduated compression stocking was worn while the patient was ambulatory for 2 weeks, with the outer stocking removed when the patient was supine. Four weeks later, examination showed complete fibrosis and resolution of all symptoms.
Case Study 12 Treatment of dorsal hand veins
A 42-year-old woman complained of unsightly veins on the dorsal hands (Fig. 9.39A). She was advised of the normality of this appearance and the possible necessity for preserving these veins for insertion of intravenous catheters. Nevertheless, she insisted on their removal. Experience has demonstrated that strong sclerosing solutions of high concentration are necessary to eliminate these normal veins.211 However, when the entire superficial venous network is sclerosed in a single session, hand edema is common and has been reported to occur in up to 82% of patients, resolving over 7 to 10 days.211 To minimize edema, the author’s method of treatment involves injecting half of the dorsal veins with STS 2% in one session (usually 2 to 4 mL). Three to four weeks later, the author injects the remaining veins with another 2 to 4 mL of STS 2%. Injections are performed with a 27- or 30-gauge needle with a nurse providing a tourniquet on the midforearm until the injection is completed. The hand is then elevated, the dorsal aspect is padded with cotton balls, and an Ace bandage is wrapped from the distal hand to the proximal forearm. The Ace wrap is left in place for 2 days, during which time the patient may vary the compression to avoid numbness of the fingers. Patients usually have near total resolution of the visible veins with this technique (Fig. 9.39B). Hand edema occurs in 20% of patients. To date, no episodes of pigmentation or telangiectatic matting have been seen. Although Duffy has reported superficial necrosis with probable extravasation of solution in one patient,212 and numbness and paresthesia persisting for 2 weeks in another patient,211 this procedure is remarkably free from adverse sequelae.
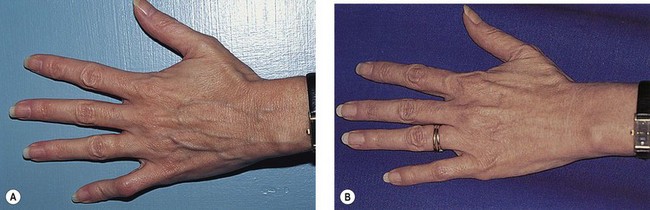
Case Study 13 Duplex-guided injection
This 35-year-old male presented with a painful isolated varicose cluster of the left popliteal fossa and medial upper third of the lower leg (C2s Ep As Pr). Varicose veins were fed by a popliteal fossa perforating vein and drained into a GSV tributary (Fig. 9.40A).

The vein was treated with one injection of 4 cm3 of POL 0.5% through a butterfly needle (Fig. 9.40B), and massage with the ultrasound probe to fill up the whole varicose network. Compression was realized with knee-high class II medical stockings and a popliteal foam pad.
At 1 month, no visible varicose veins remained; several small indurations (3–4 mm, not visible on pictures) were palpable and were punctured (Fig. 9.40C).
Case Study 14 VeinRx catheter foam sclerotherapy of the GSV
Rodrigo González Zeh, MD, Santiago, Chile
A 99-kg, 1.62-m, 49-year-old male presented with a varicose vein on the left lower leg, pain in the left leg, night cramps, and ankle edema (Fig. 9.41A). His CEAP classification was C3 Ep As Pr; the venous clinical severity score (VCSS) was 5.
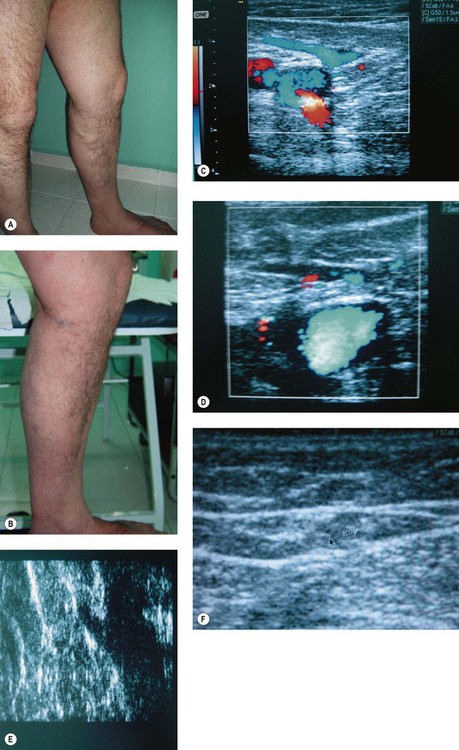
Ultrasound examination showed a normal deep venous system. The GSV was incompetent from the SFJ to the midthigh. The GSV diameter at 2 cm from the SFJ was 11 mm, with a mean diameter of 14 mm. The length of the refluxing segment measured 28 cm (Fig. 9.41B).
The procedure was performed under local anesthesia with 2 mL of lidocaine placed at the vein access site. Access to the GSV was made 34 cm from the SFJ. The VeinRx catheter was placed 1.5 cm distal to the SFJ. The leg was elevated 30 degrees for 2 minutes to allow for drainage of venous blood. The VeinRx catheter balloon was inflated with 2.6 cm3 of saline 2 cm distal to the SFJ. Ten milliliters of 3% foam (made with the Tessari technique, 2 mL of 3% STS + 8 cm3 of air) was infused into the catheter and allowed to stay in the GSV for 4 minutes. The intravascular balloon was deflated and a foam pad was placed over the treated GSV. A class II graduated compression stocking was then applied. One day after the procedure a duplex examination was performed and no evidence of thrombosis extension into the SFJ or deep venous system was noted (Fig. 9.41C). The GSV was noncompressible. Foam pads were removed and the compression stocking was worn for another 6 days and nights, then for 7 days only during daytime. The patient was evaluated with duplex ultrasound at days 1 and 7 and at months 1, 3, 6, and 12. No complications occurred. Minor ecchymosis at the access site for 1 week resolved spontaneously. Complete sclerosis of the desired segment occurred. Vein size was 1.2 mm (almost not visible) at 12 months (Fig. 9.41D).
The ultrasound images are from 12 months post treatment: you may see the epigastric vein patent (Fig. 9.41E) and the GSV with firm sclerosis and echogenicity similar to surrounding tissue (a little more dense) (Fig. 9.41F). The femoral vein is patent.
Case Study 15 Varicose veins and venous ulcers treated with sclerosant microfoam
A 64-year-old woman presented with bilateral leg ulcers open for 1 and 2 years (right and left, respectively). She had bilateral varicose veins which had been severe for in excess of 20 years (Fig. 9.42A). Previous treatment was confined to compression and local antiseptics.
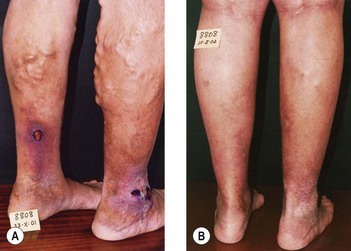
Photographs taken 3 months later show the healed ulcers and greatly reduced varicose veins (Fig. 9.42B). Two years later, recanalization of both GSV with narrow lumens was detected, but the ulcers remained healed. A further 12 mL of 1% POL mf was injected into recanalized segments. There were no complications following any of the treatments. At last review 43 months after the first treatment, the ulcers remained healed, no varicosities were visible, and there was no reflux.
Case Study 16 Microfoam sclerotherapy in Klippel-Trenaunay Syndrome (KTS) and a patent foramen ovale (PFO)
P Redondo, G Bastarrika, A Sierra, A Martinez-Cuesta, J Cabrera
A 25-year-old women presented with KTS manifested as widespread venous varicosities and a segmental port wine stain affecting the left leg with associated intralesional pain. Multidectector-row computed tomography (MDCT) revealed that the aberrant vessels originated from the superficial venous system with a normal deep venous system. Duplex ultrasound demonstrated incompetence in the superficial system. She was then treated with polidocanol microfoam (POL mf) injected into the marginal, great saphenous, and peripheral small veins via 20, 23, and 25-guage needles, respectively, under ultrasound guidance with limb elevation for 15–20 minutes followed by graduated compression with a Struva 23-mmHg stocking for 7 to 15 days (Medi-Bayreuth, Bayreuth, Germany). Eight separate treatment sessions over 12 months with injection of 20 to 80 mL of POL mf at 0.25 to 2% concentration was required. A migraine headache after the second session resulted in a work-up which demonstrated bubbles in the middle cerebral artery. Magnetic resonance imaging at 24 hours showed no evidence of cerebral damage and all subsequent treatments were without incident. Examinations 6 months after the final sclerotherapy session with MDCT revealed significant clinical improvement and reduction in the number and size of the percutaneously treated aberrant veins (Fig. 9.43).
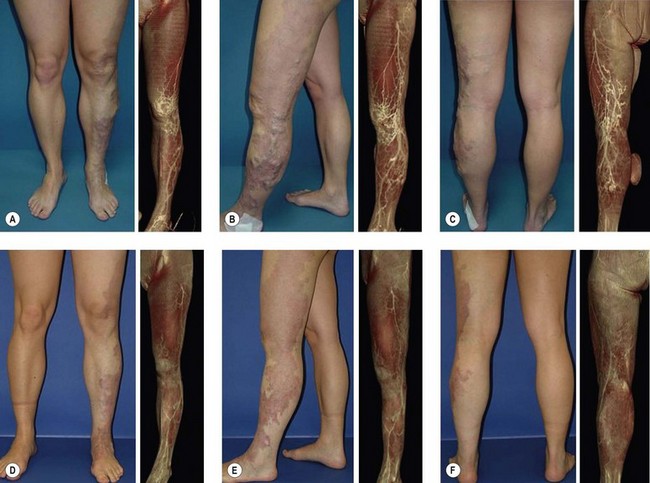
1 Faxon HH. End results in the injection treatment of varicose veins. N Engl J Med. 1934;208:357.
2 Goldman MP, Fronek A. Anatomy and pathophysiology of varicose veins. J Dermatol Surg Oncol. 1989;15:138.
3 Goldman MP, Bennett RG. Treatment of telangiectasia: a review. J Am Acad Dermatol. 1987;17:167.
4 De Groot WP. Treatment of varicose veins: modern concepts and methods. J Dermatol Surg Oncol. 1989;15:191.
5 Pittaluga P, Rea B, Barbe R. Méthode ASVAL (ablation selective des varices sous anesthesia locale): principes et resultants preliminaires. Phlebologie. 2005;58:175.
6 Tournay R, et al. La sclerose des varices, 4th ed. Paris: Expansion Scientifique Francaise; 1985.
7 Heyerdale WW, Stalker LK. Management of varicose veins of the lower extremities. Ann Surg. 1941;114:1042.
8 Moszkowicz L. Behandlung der Krampfadern mit Zuckerinjektionen kombinurt mit Venenligatur. Zentralbl Chir. 1927;54:1732.
9 De Takats G, Quint H. The injection treatment of varicose veins. Surg Gynecol Obstet. 1930;50:545.
10 Sigg K. Neure Gesichtspunkte zur Technik der Varizenbehandlung. Ther Umsch. 1949;6:127.
11 Dodd H, Cockett FB. The pathology and surgery of the veins of the lower limbs. London: ES Livingstone; 1956.
12 Reid RG, Rothnie NG. Treatment of varicose veins by compression sclerotherapy. Br J Surg. 1968;55:889.
13 Fegan WC, Fitzgerald DE, Milliken JC. The results of simultaneous pressure recordings from the superficial and deep veins of the leg. Ir J Med Sci. 1964;6:363.
14 Quill RD, Fegan WG. Reversibility of femorosaphenous reflux. Br J Surg. 1971;55:389.
15 Schalin L. Arteriovenous communication localized by thermography and identified by operative microscopy. Acta Chir Scand. 1981;147:109.
16 Kakkar VV, Howe CT, Flanc C. Compression sclerotherapy for varicose veins – a phlebographic study. Br J Surg. 1969;56:620.
17 Zukowski AJ, Nicolaides AN, Szendro G, et al. Haemodynamic significance of incompetent calf perforating veins. Br J Surg. 1991;78:625.
18 Tolins SH. Treatment of varicose veins: an update. Am J Surg. 1983;145:248.
19 Doran FSA, White M. A clinical trial designed to discover if the primary treatment of varicose veins should be by Fegan’s method or by operation. Br J Surg. 1975;62:72.
20 Hobbs JT. Surgery and sclerotherapy in the treatment of varicose veins: a random trial. Arch Surg. 1974;109:793.
21 Tretbar LL, Pattisson PH. Injection-compression treatment of varicose veins. Am J Surg. 1970;120:539.
22 Sladen JG. Compression sclerotherapy: preparation, technique, complications, and results. Am J Surg. 1983;146:228.
23 Hobbs JT. A random trial of the treatment of varicose veins by surgery and sclerotherapy. In: Hobbs JT, editor. The treatment of venous thrombosis. Philadelphia: JB Lippincott, 1977.
24 Kerner J, Schultz-Ehrenburg U. Funktionele auswirkungen unterschiedlicher angriffspunkte bei der Sklerosierungstherapie. Phlebol Proktol. 1988;17:101.
25 Kerner J, Schultz-Ehrenburg U. Functional meaning of different injection levels in the course of sclerotherapy. Phlebology. 1989;4:123.
26 Goldman MP. Rational treatment of varicose and spider leg veins. In: Robins P, editor. Surgical gems in dermatology, vol 2. New York: Igaku-Shoin Medical; 1991.
27 Hobbs JT. Surgery or sclerotherapy for varicose veins. In: Superficial and deep venous diseases of the lower limbs. Turin: Minerva Medica; 1984.
28 Neglen P. Treatment of varicosities of saphenous origin: comparison of ligation, selective excision, and sclerotherapy. In Goldman MP, Weiss RA, Bergan JJ, editors: Varicose veins and telangiectasias: diagnosis and treatment, 2nd ed, St Louis: Quality Medical Publishing, 1999.
29 Bishop CCR, Fronek HS, Froneck A, et al. Real-time color duplex scanning after sclerotherapy of the greater saphenous vein. J Vasc Surg. 1991;14:505.
30 Butie A. Experience with injections at the saphenofemoral junction in the United States. In: Davy A, Stemmer R, editors. Phlébologie ’89. Montrouge, France: John Libbey Eurotext, 1989.
31 Biegeleisen K, Nielsen RD. Failure of angioscopically guided sclerotherapy to permanently obliterate greater saphenous varicosity. Phlebology. 1994;9:21.
32 Cooper WM. The treatment of varicose veins. Ann Surg. 1934;99:799.
33 Boyd AM, Robertson DJ. Treatment of varicose veins: possible danger of injection of sclerosing fluids. Br Med J. 1947;2:452.
34 Raymond-Martimbeau P. Two different techniques for sclerosing the incompetent saphenofemoral junction: a comparative study. J Dermatol Surg Oncol. 1990;16:626.
35 Bassi G. Indikationen und Resultate der Sklerotherapie bzw Chirurgie in der Behandlung der Insuffizienzen. Zbl Phlebol. 1965;4:143.
36 Hordegen K, Sigg K. Krosseverodung der Vena saphena magna: kasuistischer beitrag zur Technik der Verodungsinjektion. Phlebol Proktol. 1985;14:231.
37 Cloutier G, Zummo M. La sclerose des crosses avec compression: resultats a long terme. Phlebologie. 1986;39:145.
38 Leu HJ. Zur Therapie der Saphena-magna-Varikosis: Chirurgie oder Sklerosierung? Praxis. 1968;14:491.
39 Avramovic A, Avramovic M. Statistical evaluation of sclerotherapy of the long saphenous vein and the sapheno-femoral junction. In: Raymond-Martimbeau P, Prescott R, Zummo M, editors. Phlébologie ’92. Paris: John Libbey Eurotext, 1992.
40 Schultz-Ehrenburg U, Weindorf N, Tourbier H. Moderne, hämodynamisch orientierte Richtlinien fur die Sklerosierung der Stamm- und Seitenastvaricosis der V saphena magna und parva. Phlebol Proktol. 1988;17:83.
41 Raymond-Martimbeau P. Role of sclerotherapy in greater saphenous vein incompetence. In Goldman MP, Weiss RA, Bergan JJ, editors: Varicose veins and telangiectasias: diagnosis and treatment, 2nd ed, St Louis: Quality Medical Publishing, 1999.
42 Bjordal RI. Circulation patterns in incompetent perforating veins in the calf and in the saphenous system in primary varicose veins. Acta Chir Scand. 1972;138:251.
43 Trempe J. Long-term results of sclerotherapy and surgical treatment of the varicose short saphenous vein. J Dermatol Surg Oncol. 1991;17:597.
44 McAdam WAF, Horrocks JC, de Dombal FT. Assessment of the results of surgery for varicose veins. Br J Surg. 1976;63:137.
45 Sigg K. Varizen-ulcus cruris und thrombose. Berlin: Springer-Verlag; 1976.
46 McCaffrey JJ. An approach to the treatment of varicose veins. Med J Aust. 1969;1:1379.
47 Sigg K. The treatment of varicosities and accompanying complications. Angiology. 1952;3:355.
48 Kimmonth JB. Discussion on primary treatment of varicose veins. Proc R Soc London. 1948;41:631.
49 Steinacher J, Kammerhuber F. Weg und verweildauer eines kontrastmittels im oberflachlichen Venesystem unter bedingungender Varicenverodung: eine studie zur Technik der Varicenverodung. Zschr Haut-Geschl-Krkh. 1968;43:369.
50 Heyn G, Waigand J, Tamaschke C. Flow behaviour of sclerosants in the treatment of primary varicose veins. In: Davy A, Stemmer R, editors. Phlébologie ’89. Montrouge, France: John Libbey Eurotext, 1989.
51 Meisen V. A lecture on injection-treatment of varicose veins and their sequelae (eczema and ulcus cruris), clinically and experimentally. Acta Chir Scand. 1926;60:435.
52 Foote RR. Varicose veins. St Louis: CV Mosby; 1949.
53 Thornhill R. Varicose veins and their treatment by ‘empty vein’ injection. London: Balliere, Tindall & Cox; 1929.
54 Lufkin H, McPheeters HO. Pathological studies on injected varicose veins. Surg Gynecol Obstet. 1932;54:511.
55 Orbach EJ. A new approach to the sclerotherapy of varicose veins. Angiology. 1950;1:302.
56 Fegan WG. Continuous compression technique of injecting varicose veins. Lancet. 1963;282:109.
57 Foley DP, Forrestal MD. A comparative evaluation of the empty vein utilizing duplex ultrasonography. In: Raymond-Martimbeau P, Prescott R, Zummo M, editors. Phlébologie ’92. Paris: John Libbey Eurotext, 1992.
58 Perchuk E. Injection therapy of varicose veins: a method of obliterating huge varicosities with small doses of sclerosing agent. Angiology. 1974;25:393.
59 Fegan WG. Personal communication, 1990.
60 Orbach EJ. Sclerotherapy of varicose veins: utilization of an intravenous air block. Am J Surg. 1944;66:362.
61 Wollmann JC. The history of sclerosing foams. Dermatol Surg. 2004;30:694.
62 Guex JJ. Foam sclerotherapy: an overview of use for primary venous insufficiency. Semin Vasc Surg. 2005;18:25.
63 Guex J-J. Sclerotherapy in venous disease. In: Davies AH, editor. Vascular surgery highlights 2003–4. London: Health Press; 2004:38-44.
64 Monfreux A. Traitement sclérosant des troncs saphéniens et leurs collaterals de gros caliber par la méthode MUS. Phlebologie. 1997;50:351.
65 Cabrera J, Garrido JR, Garcia-Olmedo A. Nuevo metodo de esclerosis enlas varices tronculares. Pathologica Vasculares. 1995;4:55.
66 Tessari L, Cavezzi A, Frullini A. Preliminary experience with a new sclerosing foam in the treatment of varicose veins. Dermatol Surg. 2001;27:58.
67 Hamel-Desnos C, Desnos P, Wollmann JC, et al. Evaluation of the efficacy of polidocanol in the form of foam compared with liquid form in sclerotherapy of the greater saphenous vein: initial results. Dermatol Surg. 2003;29:1170.
68 Jia X, Mowatt G, Burr JM, et al. Systematic review of foam sclerotherapy for varicose veins. Br J Surg. 2007;94:925.
69 Sadoun S. Testing the viscosity and adherence of the ‘on-site’ made foam for sclerosing varicose veins. Int Angiol. 2005;24(S1–3):75.
70 Yamaki T, Nozaki M, Iwasaka S. Comparative study of duplex guided foam sclerotherapy and duplex guided liquid sclerotherapy for the treatment of superficial venous insufficiency. Dermatol Surg. 2004;30:718.
71 Hamel-Desnos C, Allaert FA. Liquid versus foam sclerotherapy. Phlebology. 2009;24:240.
72 Ouvry P, Allaert FA, Desnos P, Hamel-Desnos C. Efficacy of polidocanol foam versus liquid in sclerotherapy of the great saphenous vein: a multicentre randomised controlled trial with a 2-year follow-up. Eur J Vasc Endovasc Surg. 2008;36:366.
73 Van Den Bos R, Arends L, Kockaert M, et al. Endovenous therapies of lower extremity varicosities: a meta-analysis. J Vasc Surg. 2009;49:230.
74 Kendler M, Wetzig T, Simon JC. Foam sclerotherapy –a possible option in therapy of varicose veins. J Dtsch Dermatol Ges. 2007;5:648.
75 Hill D, Hamilton R, Fung T. Assessment of techniques to reduce sclerosant foam migration during ultrasound-guided sclerotherapy of the great saphenous vein. J Vasc Surg. 2008;48:934.
76 Hu WS. Oxygen transfer in cell culture bioreactors. Cellular Bioprocess Technology. 2004:1-14.
77 Trigilia TCS. Foam preparation for sclerotherapy by means of heat application. Int Angiol. 2005;24(S1–3):70.
78 Frullini A, Cavezzi A. Sclerosing foam in the treatment of varicose veins and telangiectases: history and analysis of safety and complications. Dermatol Surg. 2002;28:11.
79 Redondo P, Cabrera J. Microfoam treatment of Klippel-Trénaunay syndrome and vascular malformations. J Am Acad Dermatol. 2008;59:355.
80 Breu FX, Guggenbichler S, Wollmann JC. 2nd European Consensus Meeting on Foam Sclerotherapy 2006, Tegernsee, Germany. Vasa. 2008;37(Suppl 71):1.
81 Cavezzi A, Tessari L. Foam sclerotherapy techniques: different gases and methods of preparation, catheter versus direct injection. Phlebology. 2009;24:247.
82 Rao J, Goldman MP. Stability of foam in sclerotherapy: differences between sodium tetradecyl sulfate and polidocanol and the type of connector used in the double-syringe system technique. Dermatol Surg. 2005;31:19.
83 Peterson JD, Goldman MP. An investigation on the influence of various gases and concentrations of sclerosants in foam stability. Phlebology. 2011. [In Press]
84 Lai SW, Goldman MP. Does the relative silicone content of different syringes affect the stability of foam in sclerotherapy? J Drugs Dermatol. 2008;7:399.
85 Hill D. Effect of a 5 micron filter on CO2 sclerosant foam stability. Int Angiol. 2009;29(S1–3):8.
86 Rush JE, Wright DD. More on microembolism and foam sclerotherapy. N Engl J Med. 2008;359:656. author reply 657
87 Rabe E, Pannier-Fisher F, Gerlach H, et al. German Society of Phlebology: Guidelines for sclerotherapy of varicose veins (ICD 10: I83.0, I83.1, I83.2, and I83.9). Dermatol Surg. 2004;30:687.
88 Hamel-Desnos C, Ouvry P, Benigni JP, et al. Comparison of 1% and 3% polidocanol foam in ultrasound guided sclerotherapy of the great saphenous vein: a randomised, double-blind trial with 2 year-follow-up: ‘The 3/1 Study’. Eur J Vasc Endovasc Surg.. 2007;34:723.
89 Thibault P. Internal compression (peri-venous compression) following ultrasound guided sclerotherapy to the great and small saphenous veins. Aust N Z J Phlebol. 2005;9:29.
90 Barrett JM, Allen B, Ockelford A, Goldman MP. Microfoam ultrasound guided sclerotherapy treatment for varicose veins in a subgroup with diameters at the junction of 10 mm or greater compared with a subgroup of less than 10 mm. Dermatol Surg. 2004;30:1386.
91 Barrett JM, Allen B, Ockelford A, Goldman MP. Microfoam ultrasound guided sclerotherapy of varicose veins in 100 legs. Dermatol Surg. 2004;30:6.
92 Martimbeau PR. A randomized clinical trial comparing the sclerosing and side effects of foam vs. liquid formula for sclerotherapy of primary varicose veins. Presented at the UIP World Congress Chapter Meeting. San Diego, Calif, 2003.
93 Cabrera J, Cabrera JJr, Garcia-Olmedo A. Treatment of varicose long saphenous veins with sclerosant in microfoam form: long-term outcomes. Phlebology. 2000;15:19.
94 Tessari L. Compression following trans-catheter foam sclerotherapy. Presented at the UIP World Congress Chapter Meeting. San Diego, Calif, 2003.
95 Wright D, et al. Varisolve(r) polidocanol microfoam compared with surgery or sclerotherapy in the management of moderate to severe varicose veins: European randomized controlled trial. J Vasc Surg. 2006;21:180.
96 Myers KA, Jolley D, Clough A, Kirwan J. Outcome of ultrasound-guided sclerotherapy for varicose veins: medium-term results assessed by ultrasound surveillance. Eur J Vasc Endovasc Surg. 2007;33:116.
97 Chapman-Smith P, Browne A. Prospective five-year study of ultrasound-guided foam sclerotherapy in the treatment of great saphenous vein reflux. Phlebology. 2009;24:183.
98 Darke SG, Baker SJ. Ultrasound-guided foam sclerotherapy for the treatment of varicose veins. Br J Surg. 2006;93:969.
99 O’Hare JL, Parkin D, Vandenbroeck CP, Earnshaw JJ. Mid term results of ultrasound guided foam sclerotherapy for complicated and uncomplicated varicose veins. Eur J Vasc Endovasc Surg. 2008;36:109.
100 Ceulen RP, Bullens-Goessens YI, Pi-van de Venne SJ, et al. Outcomes and side effects of duplex-guided sclerotherapy in the treatment of great saphenous veins with 1% versus 3% polidocanol foam: results of a randomized controlled trial with 1-year follow-up. Dermatol Surg. 2007;33:276.
101 Ceulen RP, Shadid N, Essers SM, et al. Outcomes and side effects of duplex-guided sclerotherapy in the treatment of great saphenous veins with 1% versus 3% polidocanol foam: results of a randomized controlled trial with 2.5-years follow-up. Dermatol Surg. 2007;33:276.
102 Yamaki T, Nozaki M, Sakurai H, et al. Multiple small-dose injections can reduce the passage of sclerosant foam into deep veins during foam sclerotherapy for varicose veins. Eur J Vasc Endovasc Surg. 2009;37:343.
103 Gillet JL, Guedes JM, Guex JJ, et al. Side-effects and complications of foam sclerotherapy of the great and small saphenous veins: a controlled multicentre prospective study including 1,025 patients. Phlebology. 2009;24:131.
104 Morrison N, Neuhardt DL, Rogers CR, et al. Comparisons of side effects using air and carbon dioxide foam for endovenous chemical ablation. J Vasc Surg. 2008;47:830.
105 Neuhardt D, Morrison N, Salles-Cunha S. Cerebral emboli comparison detected by transcranial Doppler during ultrasound-guided sclerotherapy using CO2-O2-based foam or air-based foam. Int Angiol. 2009;29(S1–3):108.
106 Cabrera J, Redondo P, Becerra A, et al. Ultrasound-guided injection of polidocanol microfoam in the management of venous ulcers. Arch Dermatol. 2004;140:667.
107 Guex JJ, Allaert FA, Gillet JL, Chleir F. Immediate and midterm complications of sclerotherapy: report of a prospective multicenter registry of 12,173 sclerotherapy sessions. Dermatol Surg. 2005;31:123.
108 Besnard S, Capri A, Philippot M, et al. Vascular distribution of an ultrasound contrast agent used to simulate decompression bubbles. Aviat Space Environ Med. 2006;77:846.
109 Ceulen RP, Sommer A, Vernooy K. Microembolism during foam sclerotherapy of varicose veins. N Engl J Med. 2008;358:1525.
110 Morrison N, Neuhardt D, Knopf K. Simultaneous echocardiography with ultrasound guided foam sclerotherapy. Int Angiol. 2005;24(S1–3):81.
111 Morrison N, Neuhardt DL. Foam sclerotherapy: cardiac and cerebral monitoring. Phlebology. 2009;24:252.
112 Forlee MV, Grouden M, Moore DJ, Shanik G. Stroke after varicose vein foam injection sclerotherapy. J Vasc Surg. 2006;43:162.
113 Bush RG, Derrick M, Manjoney D. Major neurological events following foam sclerotherapy. Phlebology. 2008;23:189.
114 Raymond-Martimbeau P. Pre-foam scleotherapy patent foramen ovale screening. Int Angiol. 2007;26(S1–S2):SS12-03.
115 Eckmann D, Kobayashi S, Li M. Microvascular embolization following polidocanol microfoam sclerosant administration. Dermatol Surg. 2005;31:636.
116 Guex JJ. Complications and side-effects of foam sclerotherapy. Phlebology. 2009;24:270.
117 Shadid N, Frank J, Sommer A. Superficial thrombophlebitis of the venous dorsal arch of the foot and deep venous thrombosis after foam sclerotherapy. Int J Dermatol. 2008;47(Suppl 1):29.
118 Kölbel T, Hinchliffe RJ, Lindblad B. Catheter-directed foam sclerotherapy of axial saphenous reflux: early results. Phlebology. 2007;22:219.
119 Wilson G. Two cases of infection complicating foam ultrasound guided sclerotherapy (UGS). Aust N Z J Phlebol. 2005;9:39.
120 Goldman MP. Sclerotherapy treatment of varicose and telangiectatic leg veins: my way and my practice. Int Angiol. 2005;24(S1–3):48.
121 Goldman MP. My sclerotherapy technique for telangiectasias and reticular veins. Dermatol Surg. 2010;36(Suppl 2):967.
122 Yamaki T, Nozaki M, Sakurai H, et al. Prospective randomized efficacy of ultrasound-guided foam sclerotherapy compared with ultrasound-guided liquid sclerotherapy in the treatment of symptomatic venous malformations. J Vasc Surg. 2008;47:578.
123 Kalodiki E, Azzam M, Kakkos SK, et al. Ultrasound-guided foam sclerotherapy combined with saphenofemoral ligation versus surgical treatment of varicose veins: intermediate results of a randomized control trial. Phlebology. 2008;23:242.
124 King T. Preliminary experience with concomitant ultrasound-guided foam sclerotherapy and endovenous laser ablation: a series of 1000 cases. Phlebology. 2008;23:241.
125 Tejedor C, Guex JJ. Foramen ovale perméable et sclérothérapie. Phlébologie. 2008;61:319.
126 Wright DD, Gibson KD, Barclay J, et al. High prevalence of right-to-left shunt in patients with symptomatic great saphenous incompetence and varicose veins. J Vasc Surg. 2010;51:104.
127 Handke M, Harloff A, Olschewski M, et al. Patent foramen ovale and cryptogenic stroke in older patients. N Engl J Med. 2007;357:2262.
128 Diener HC, Weimar C, Katsarava Z. Patent foramen ovale: paradoxical connection to migraine and stroke. Curr Opin Neurol. 2005;18:299.
129 Post MC, Thijs V, Herroelen L, Budts WI. Closure of a patent foramen ovale is associated with a decrease in prevalence of migraine. Neurology. 2004;62:1439.
130 Schwerzmann M, Wiher S, Nedeltchev K, et al. Percutaneous closure of patent foramen ovale reduces the frequency of migraine attacks. Neurology. 2004;62:1399.
131 Raymond-Martimbeau P. Transient adverse events positively associated with patent foramen ovale after ultrasound-guided foam sclerotherapy. Phlebology. 2009;24:114.
132 Orbach EJ. Clinical evaluation of a new technique in the sclerotherapy of varicose veins. J Int Coll Surg. 1948;11:396.
133 Knight RM. Treatment of superficial venous disease with accurate sclerotherapy. Proceedings of the Canadian Society of Phlebology, 1991, Whistler, British Columbia, Canada.
134 Raymond-Martimbeau P. Advanced sclerotherapy treatment of varicose veins with duplex ultrasonographic guidance. Semin Dermatol. 1993;12:123.
135 Knight RM, Vin F, Zygmunt JA. Ultrasonic guidance of injections into the superficial system. In: Davy A, Stemmer R, editors. Phlébologie ‘89. Montrouge, France: John Libbey Eurotext, 1989.
136 Misery G, Reinharez D, Ecalard P. Sclerose sous echographie dans certaines zones a risques. Phlebologie. 1991;44:84.
137 Cornu-Thenard A, Boivin P. Treatment of varicose veins by sclerotherapy: an overview. In Goldman MP, Weiss RA, Bergan JJ, editors: Varicose veins and telangiectasias: diagnosis and treatment, ed 2, St Louis: Quality Medical Publishing, 1999.
138 Thibault PK, Lewis WA. Recurrent varicose veins: Part 2: Injection of incompetent perforating veins using ultrasound guidance. J Dermatol Surg Oncol. 1992;18:895.
139 Grondin L, Soriano J. Echosclerotherapy, a Canadian study. In: Raymond-Martimbeau P, Prescott R, Zummo M, editors. Phlébologie ’92. Paris: John Libbey Eurotext, 1992.
140 Parsi K, Lim AC. Extended long line echosclerotherapy (ELLE). Aust N Z J Phlebol. 2000;4:6.
141 Kanter A, Thibault P. Saphenofemoral incompetence treated by ultrasound-guided sclerotherapy. Dermatol Surg. 1996;22:648.
142 Thibault PK. ‘5 year’ follow-up of greater saphenous vein incompetence treated by ultrasound guided sclerotherapy. Aust N Z J Phlebol. 2003;7:5.
143 Oishi AJ, Zietlow SP, Sarr MG. Erroneous arterial placement of a central venous catheter. Mayo Clin Proc. 1994;69:287.
144 Grondin L, Raymond-Martimbeau P. Superficial venous disease disorders. In: Leclerc JR, editor. Venous thrombo-embolic disorders. Philadelphia: Lea & Febiger, 1991.
145 Thibault PK, Lewis WA. Recurrent varicose veins. Part 1: Evaluation utilizing duplex venous imaging. J Dermatol Surg Oncol. 1992;18:618.
146 Royle JP. Recurrent varicose veins. World J Surg. 1986;10:944.
147 Doran FSA, Barkat S. The management of recurrent varicose veins. Ann R Coll Surg Engl. 1981;63:432.
148 de Waard MM, der Kinderen DJ. Duplex ultrasonography-guided foam sclerotherapy of incompetent perforator veins in a patient with bilateral venous leg ulcers. Dermatol Surg. 2005;31:580.
149 Van Neer PAFA. Perforans varicosis: treatment of the incompetent perforating vein is important. Dermatol Surg. 2004;30:754.
150 Schadeck M. Duplex-guided sclerotherapy of the lesser saphenous vein. Scope Phlebol Lymphol. 2002;1:330.
151 Bullens-Goessens YIJM, Mentink LF, Nelemans PJ, van Geest AJ, Veraart JCJM. Ultrasound-guided sclerotherapy of the insufficient short saphenous vein. Phlebologie. 2004;33:89.
152 Cornu-Thenard A. Sclerotherapy: Doppler-guided injection. Presented at the Annual Meeting of the North American Society of Phlebology, Maui, Hawaii, February 23, 1994.
153 Cornu-Thenard A, De Cottreau H, Weiss RA. Sclerotherapy: continuous wave Doppler-guided injections. Dermatol Surg. 1995;21:867.
154 Van Cleef JF, Desvaux P, Griton P, Cloarec M. Sclerose de la saphene externe sous controle endoscopique. Phlebologie. 1991;44:131.
155 Van Cleef JF. Sclerotherapy of the external saphenous vein under endoscopic control. Presented at the World Congress of Phlebology, Strasbourg, France, 1989.
156 Cavaye DM, White RA, Kopchok GE, et al. Intravascular ultrasound imaging: the new standard for guidance and assessment of endovascular interventions? J Clin Laser Med Surg. 1992;10:349.
157 Gussenhoven WJ, Essed CE, Lancee CT. Arterial wall characteristics determined by intravascular ultrasound imaging: an in vitro study. J Am Coll Cardiol. 1989;14:947.
158 Mallery JAS, Tobis JM, Griffith J, et al. Assessment of normal and atherosclerotic arterial wall thickness within intravascular ultrasound imaging catheter. Am Heart J. 1990;119:1392.
159 Nissen SE, Grines CL, Gurley JC, et al. Application of a new phased-array ultrasound imaging catheter in the assessment of vascular dimensions. Circulation. 1990;81:660.
160 Raymond-Martimbeau P. Intravenous ultrasound in the management of varicose veins. Phlebology. 1995;1(Suppl):326.
161 Raymond-Martimbeau P. Role of sclerotherapy in greater saphenous vein incompetence. In Goldman MP, Weiss RA, Bergan JJ, editors: Varicose veins and telangiectasias: diagnosis and treatment, 2nd ed, St Louis: Quality Medical Publishing, 1999.
162 Min RJ, Navarro L. Transcatheter duplex ultrasound-guided sclerotherapy for treatment of greater saphenous vein reflux: preliminary report. Dermatol Surg. 2000;26:410.
163 Goldman MP, Weiss RA, Bergan JJ. Varicose veins and telangiectasias: diagnosis and treatment, 2nd ed. St Louis: Quality Medical Publishing; 1999.
164 Sadoun S, Benigni JP, Chahim M, et al. Multicenter international prospective study on the side effects of the sclerosing treatment of the greater saphenous vein: SESIS study of the secondary effects of sclerosis of the internal saphenous vein. Phlebologie. 2000;53:345.
165 Ferrara F, Berbach HR. Sclerotherapy of the sapheno-femoral junction: a duplex examination. Acta Phlebol. 2002;3:35.
166 Valsamis M. Diameter of the greater saphenous vein near the saphenofemoral junction and response to injection sclerotherapy treatment. Presented at the UIP World Congress Chapter Meeting. San Diego. Calif., 2003.
167 Ninia JG, Goldberg TL. Treatment of vulvar varicosities by injection-compression sclerotherapy and a pelvic supporter. Obst Gynecol. 1996;87:786.
168 Ninia JG. Treatment of vulvar varicosities by injection-compression sclerotherapy. Dermatol Surg. 1997;23:573.
169 Yamaki T, Nozaki M, Sasaki K. Color duplex-guided sclerotherapy for the treatment of venous malformations. Dermatol Surg. 2000;26:323.
170 Lee BK, Kim DI, Huh S, et al. New experiences with absolute ethanol sclerotherapy in the management of a complex form of congenital venous malformation. J Vasc Surg. 2001;33:764.
171 Lee BB, Do YS, Byun HS, Choo IW, Kim DI, Huh SH. Advanced management of venous malformations with ethanol sclerotherapy: mid-term results. J Vasc Surg. 2003;37:533.
172 Cabrera J, Cabrera JJr, Garcia-Olmedo A, Redondo P. Treatment of venous malformations with sclerosant in microfoam form. Arch Dermatol. 2003;139:1409.
173 Ku H-W, Yang C-H. Venous lake of the lip treated with a sclerosing agent: report of two cases. Dermatol Surg. 2003;29:425.
174 Matsumoto K, Nakanishi H, Koizumi Y, Seike T, Kanda I, Kubo Y. Sclerotherapy of hemangioma with late involution. Dermatol Surg. 2003;29:668.
175 Parsi K, Kossard S. Multiple hereditary glomangiomas: successful treatment with sclerotherapy. Australas J Dermatol. 2002;43:43.
176 Matsumoto K, Nakanishi H, Seike T, Koizumi Y, Mihara K, Kubo Y. Treatment of pyogenic granuloma with a sclerosing agent. Dermatol Surg. 2001;27:521.
177 Moon S, Hwang E, Cho KH. Treatment of pyogenic granuloma by sodium tetradecyl sulfate sclerotherapy. Arch Dermatol. 2005;141:644.
178 Perrin MR, Guex J-J, Ruckley CV, et al. and the REVAS group: Recurrent varices after surgery, a consensus document. Cardiovasc Surg. 2000;8:233.
179 Keates JS, Fitzgerald DE. Limb volume and blood flow changes during the menstrual cycle. Angiology. 1969;20:618.
180 Vin F. Principles, technique, and results of treatment of the greater saphenous vein by sclerotherapy. Presented at the second Annual International Congress of the North American Society of Phlebology, New Orleans, February 25, 1989.
181 Merlen JF, Curri SB, Saout J, et al. Histologic study of a sclerosed vein. Phlebologie. 1978;31:17.
182 Sackmann LA. Etude physique de l’injection sclerosante. Soc Fr Phlebol. 1969;22:149.
183 Green D. Mechanism of action of sclerotherapy. Semin Dermatol. 1993;12:88.
184 Guex J-J. Indications for the sclerosing agent polidocanol. J Dermatol Surg Oncol. 1993;19:959.
185 Cornu-Thenard A. Sclerotherapy of varicose veins: value of measurement of vessel diameter before the first injection. Presented at the second Annual International Congress of the North American Society of Phlebology, New Orleans, February 25, 1989.
186 Kinmonth JB, Robertson DJ. Injection treatment of varicose veins: radiological and histological investigations of methods. Br J Surg. 1949;36:294.
187 Green D. Sclerotherapy for the permanent eradication of varicose veins: theoretical and practical considerations. J Am Acad Dermatol. 1998;38:461.
188 Corcos L, et al. Peripheral venous biopsy: significance, limitations, indications and clinical applications. Phlebology. 1989;4:271.
189 Stegall HF. Muscle pumping in the dependent leg. Circ Res. 1966;19:180.
190 Orbach EJ. The importance of removal of postinjection coagula during the course of sclerotherapy of varicose veins. Vasa. 1974;3:475.
191 Guex J-J. Les contre indications de la sclérothérapie en 2005. J Mal Vasc. 2005;30:144.
192 Barwin BN, Roddie IC. Venous distensibility during pregnancy determined by graded venous congestion. Am J Obstet Gynecol. 1976;125:921.
193 Skudder PAJr, Farrington DT, Weld E, Putnam C. Venous dysfunction of late pregnancy persists after delivery. J Cardiovasc Surg. 1990;31:748.
194 McPheeters HO. Prophylactic injection treatment of varicose veins during pregnancy. Lancet. 1931;51:589.
195 Kilbourne NJ. Varicose veins of pregnancy. Am J Obstet Gynecol. 1933;25:104.
196 Mullane DJ. Varicose veins of pregnancy. Am J Obstet Gynecol. 1952;63:620.
197 McCausland AM. Varicose veins in pregnancy. West J Surg. 1939;47:81.
198 Fegan G. Varicose veins: compression therapy. London: Heinemann Medical; 1967.
199 Mantse L. The treatment of varicose veins with compression sclerotherapy: technique, containdications, complications. Am J Cosmetic Surg. 1986;3:47.
200 Dodd H, Payling Wright H. Vulval varicose veins in pregnancy. Br Med J. 1959;1:831.
201 Tibbs DJ. Varicose veins and related disorders. Oxford: Butterworth-Heinemann; 1992.
202 Rabe E, et al. Die pudendale varicosis. Phlebologie. 1991;20:222.
203 De Takats G. Ambulatory ligation of the saphenous vein. JAMA. 1930;94:1194.
204 Faxon HH. Treatment of varicosities. Arch Surg. 1934;29:794.
205 Conrad P. Sclerostripping – a ‘new’ procedure for the treatment of varicose veins. Med J Aust. 1975;2:42.
206 Hubner K. The outpatient therapy of trunk varicosis of the greater saphenous vein by means of ligation and sclerotherapy. J Dermatol Surg Oncol. 1991;17:818.
207 De Groot WP. Practical phlebology: sclerotherapy of large veins. J Dermatol Surg Oncol. 1991;17:589.
208 Bihari I. Can varicetomy be performed if deep veins are occluded? J Dermatol Surg Oncol. 1990;16:806.
209 Passas H. One case of tetradecyl-sodium sulfate allergy with general symptoms. Soc Fr Phlebol. 1972;25:19.
210 Stroncek DF, Hutton SW, Silvis SE, et al. Sodium morrhuate stimulates granulocytes and damages erythrocytes and endothelial cells: probable mechanism of an adverse reaction during sclerotherapy. J Lab Clin Med. 1985;106:498.
211 Duffy DM, Garcia C, Clark RE. The role of sclerotherapy in abnormal varicose hand veins. Plast Reconstr Surg. 1999;104:1474.
212 Duffy DM. Complications of sclerotherapy for vessels involving the hands and face. Aesth Dermatol Cosmet Surg. 1999;1:91.
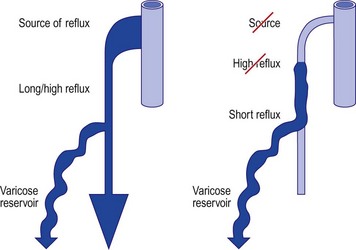
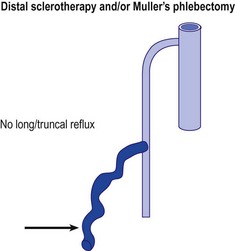
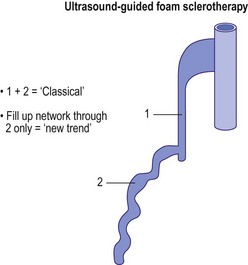
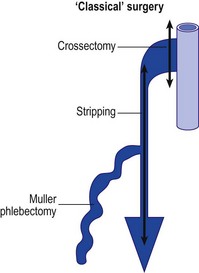
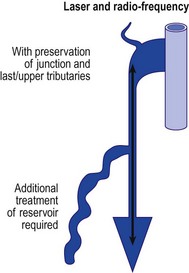
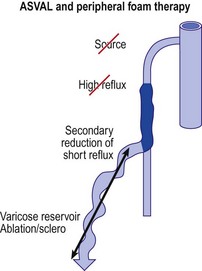
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
CHAPTER 9 Clinical Methods for Sclerotherapy of Varicose Veins
‘We feel from our three and one-half years’ experience that the surgeon who believes that there is nothing more required than a syringe, some solution, and a patient to effect permanent obliteration of varicose veins, still has much to learn.’1
Varicose veins represent tortuous dilations of existing superficial veins. They arise because of multiple factors but are always associated with a relatively elevated venous pressure.2 Therefore, it has been considered for decades that treatment initially consists of cutting off the point of high-pressure inflow to the veins (through either surgical or sclerotherapeutic methods) before treating the varicose veins themselves.3,4
This approach has been recently questioned, since, in certain cases, the importance of the ‘siphon’ effect generated by the underlying varicose reservoir is strong enough to generate a reflux in saphenous trunks. It has been observed that suppression of the varicose network reduces reflux in the saphenous trunks. The development of varicose veins in the reticular network and centripetal progression of the disease, as advocated by Hébrant and Collignon, is a hypothesis which could explain a number of varicose patterns, and an increasing number of specialists are currently applying a more distal and conservative approach, whether surgical or sclerotherapeutic.5
Historical Review of Techniques
Tournay (French) technique
The Tournay procedure encompasses the basic principle of ‘French phlebology’ developed by Tournay et al:6 treating varicose veins ‘from high to low’ (‘de haut en bas’). The rationale for this technique is in first eliminating high-pressure reflux blood flow at the point of occurrence. Treating from proximal to distal sites also eliminates the weight of the column of blood on the sclerosed point. This has the advantage of minimizing thrombosis and the extravasation of red blood cells (RBCs) from a sclerosed vein segment. The French school advocates placement of very few injections at this ‘high (proximal)’ point before treating more distal veins or sections of the same vein at a later date. This same philosophy toward treatment was also reported from the Mayo Clinic in 1941 by Heyerdale and Stalker.7 The principle of eliminating reflux from the saphenofemoral junction (SFJ) was espoused even earlier by Moszkowicz8 in Germany in 1927 and by de Takats and Quint9 in the United States in 1930. Thus the ‘French technique’ is multicultural in its origin.
In addition to developing a treatment regimen with the tenet just mentioned in mind, it is critical to obliterate the SFJ accurately because its location and anatomy are so variable (see Chapter 1). To determine the origin of high pressure in the varicose vein, a noninvasive diagnostic evaluation of the patient should be performed first (see Chapter 5). The handheld Doppler device helps detect points of reflux from the deep to the superficial veins, through either incompetent saphenofemoral or saphenopopliteal junctions or perforating veins. In certain circumstances, additional testing is required. If any points of reflux are detected, they should be treated first. After the high-pressure flow has been eliminated, treatment should proceed first with injection of the largest varicose veins, then injection of the reticular feeding veins, and finally treatment of the remaining ‘spider’ veins.
In defense of the logic of the French technique, de Groot4 pointed out that any vein in the leg belongs to either the greater saphenous system or the lesser saphenous system (Fig. 9.1). This concept implies that a vein within the defined area of the great saphenous vein (GSV) eventually drains into the GSV. Therefore, reflux in that vein is derived from reflux at the SFJ. This concept directs treatment toward the reflux point. Unfortunately, clinical examination of the location of a vein does not always correctly determine the point of reflux. Therefore the clinical examination must be correlated with a noninvasive examination to establish the optimal order of therapy.
Sigg (Swiss) technique
In contrast to the French technique, the Swiss technique of Sigg10 and the modification by Dodd and Cockett11 advocate total sclerosation of the entire varicose vein, including incompetent perforator veins (IPVs) and the SFJ. This technique has also been adopted by some physicians who modify Fegan’s technique of sclerotherapy of the IPVs (described in the following section). Included in this school are Reid and Rothnie,12 who treated 1358 legs of 974 patients and found that selective injection of perforator veins was ineffective, requiring multiple additional treatments of the entire vein. They evolved a technique of placing multiple injections at intervals along the varicose veins to produce diffuse sclerosis and have reported very favorable results. This latter technique is called the total-vein sclerotherapy technique.
Fegan technique
Fegan et al13 proposed a view opposite to the previously mentioned one, namely that saphenofemoral incompetence could occur as a result of perforator incompetence alone. They reached this conclusion by demonstrating that the calf muscle pump is more powerful than the abdominal or femoral muscles regarding venous flow in the leg. They proposed that sclerotherapy of the IPVs should be performed first, to restore normal function. Fegan’s examination of the SFJ and GSV with phlebography after sclerotherapy of IPVs showed narrowing of the vessel lumen in 9 of 11 patients.14 However, surgical exploration of clinically diagnosed areas of perforator vein incompetence has found at best a 60% incidence of perforator veins being correctly identified clinically.15 In addition, phlebographic examination performed on 112 patients with clinically suspected incompetent perforators showed that the clinical examination correctly identified only 38% of perforator veins below the knee and only 17% of thigh perforators.16 An additional study of 180 limbs with primary varicose veins studied with clinical examination, ascending deep-to-superficial venography, Doppler ultrasound, and ambulatory venous pressure measurements showed that only 40% of these patients had evidence of perforator incompetence. Of them, 30% had no hemodynamic significance to the perforator veins.17 Thus, the rationale for Fegan’s technique is open to dispute.
Despite the lack of accuracy of clinical diagnosis of IPVs, many authors have found Fegan’s technique gives excellent results. Tolins18 reported favorable results using Fegan’s technique; he injected varicose veins in areas of fascial defects with 0.5 mL of sodium tetradecyl sulfate (STS) solution at up to 23 sites per leg. Although this many injections may seem similar to the number with total vein sclerotherapy, three-quarters of the patients had two to five injections. Doran and White19 concluded after 2 years of follow-up that there was no difference between the results from Fegan’s technique and ligation and stripping procedures for varicose veins. Hobbs20 concluded from his comparative study of sclerotherapy with Fegan’s technique versus traditional surgery that sclerotherapy is the best treatment of nontruncal varicose veins and IPVs of the lower leg. Tretbar and Pattisson21 have found in their follow-up examinations of 264 patients treated with Fegan’s technique that treatment failures usually occurred in patients with very large or fat legs with varicosities originating above the knee. They believed this failure was caused by the difficulty of placing injections accurately within the veins of these patients and maintaining adequate compression. Sladen22 analyzed 263 limbs with up to 7 years of follow-up and found that more than 95% of his patients were satisfied with the treatment and said they would have it repeated. He estimated a retreatment rate of approximately 5% per year. His patients averaged 3.6 to 5.25 injections per treatment session, and 46% to 74% required one treatment session only. Sladen, in agreement with Hobbs, found that all patients with saphenofemoral reflux eventually required surgery. Therefore, although varicose veins treated with Fegan’s technique respond well to treatment, the supposition of Fegan’s technique – that sclerosis of the IPVs is of primary importance and may reverse the remaining pathology in the GSV system – may not be correct universally.
Hobbs23 provided evidence that when saphenofemoral and perforator incompetence occur together, both abnormalities should be corrected. Kerner and Schultz-Ehrenburg24,25 studied the functional effects of sclerotherapy with photoplethysmography (PPG) and concluded that the greatest functional improvement occurred with obliteration of the SFJ. Obliteration of the IPVs of the lower legs was of variable importance. Treatment of perforator veins of the upper leg had no functional significance that could be ascertained with PPG.
Treatment of reflux from the saphenofemoral junction
There are at least three schools of thought regarding which type of therapy is appropriate for initial treatment of the junctional points of reflux: surgical ligation (with or without limited stripping) of the SFJ versus sclerotherapy of the SFJ versus sclerotherapy of IPVs alone. Bergan (see Chapter 10), Goldman,26 Hobbs,20,27 and others argue that surgical treatment of the junctions is the most appropriate and successful mode of treatment, but this was before the use of endovenous ablation techniques. Neglen,28 in a comprehensive review, determined that with proper follow-up, including functional testing at 5 years, surgical therapy of the GSV in a patient with incompetence of the SFJ, is significantly better than sclerotherapy.28 Color-flow duplex evaluation, from 3 to 55 months after treatment (mean of 27.5 months) of 89 limbs in 55 patients with an incompetent SFJ treated with the Sigg technique, found that only 6% of veins remained sclerosed despite improvement in symptoms in 50%.29 Butie30 has shown that sclerotherapy of the SFJ is difficult and unreliable with the use of liquid STS 3%, which is the strongest sclerosing agent approved for use by the US Food and Drug Administration (FDA). This has been confirmed even when sclerotherapy was performed at the SFJ under angioscopic guidance (see ‘Endoscopic injection’ section).31 In this case, 12 GSVs were occluded at the SFJ through angioscopically guided sclerotherapy with STS 3% liquid (prior to the use of foamed detergent sclerosants). A total of 2 to 5 mL was injected into the GSV just below the junction, which was occluded by manual pressure. Nine veins were evaluated at follow-up, and all were reopened and incompetent between 1 and 12 months. Although these carefully performed, unbiased studies have been carried out only recently, this opinion is not new. As far back as 1934, Cooper,32 in a series of more than 85,000 injections in more than 3000 patients, documented that the number of sclerosing injections required to produce obliteration of the varicose vein was markedly decreased after ligation of the SFJ.
In addition to its lack of consistent success, sclerotherapy of the SFJ has the inherent risk of damaging the deep venous system and the femoral vein when sclerosing solution is injected in the upper thigh region. This has been demonstrated by radiologic examination showing the rapid flow of contrast media from a varicose GSV into the femoral vein when injections are performed in the upper thigh.33 With incompetence of the SFJ, it is recommended that sclerotherapy be used for treating residual varicosities after surgery.
Despite the information in the preceding paragraph, multiple phlebologists have demonstrated that the junctions can be successfully closed with sclerotherapy alone in 50% to 91% of patients.34–40 A comprehensive illustrated discussion of the technique is presented in other sources.41 The difficulty in properly evaluating these conclusions is due to the natural evolution of varicose veins, which obscures the results of both surgical and sclerotherapy treatment. It is sometimes difficult to distinguish between a recanalized vein and a new vein. Results also depend on the type of follow-up examinations (i.e. clinical or objective with duplex or Doppler ultrasound) of patients. One study with clinical 6-year follow-up demonstrated a nearly 90% success rate with sclerotherapy.34 By whatever method, closure of the SFJ has been shown in pressure studies to prevent retrograde flow in the saphenous and perforator systems.42 This suggests that incompetence of the perforator veins occurs as a result of a primary development of saphenofemoral reflux. Therefore, when the GSV or its tributaries are involved, the SFJ, when incompetent, should be the first area to be treated.
Treating incompetence of the SFJ may differ from treating an incompetent saphenopopliteal junction (SPJ). The small saphenous vein (SSV) has a variable termination (see Chapter 1) that is often difficult to approach surgically, but can be approached with modern endovenous ablation techniques. Ligation alone at the SPJ has a 95% failure rate at 1 year.43 Sclerotherapy is much more effective, perhaps because of the larger extent of destruction of abnormal feeding veins into this region.43
A comparison of three independent observers regarding treatment outcome of varicose vein surgery shows 60% agreement in assessing visual improvement, with 30% agreement between observers when symptomatic response and visual impression are compared.44 It is my opinion that no one ‘school’ is absolute but that the correct order of treatment should be individualized for each patient. Some patients have only perforator incompetence and a normal SFJ; thus, Fegan’s technique would be adequate. Patients with saphenofemoral incompetence require treatment of that junction before treatment is initiated elsewhere. Still other patients have no obvious hemodynamic cause for the origin of their varicose veins, thus directing treatment toward the entire varicosity, as described by Sigg.45 A careful workup of all patients is necessary before therapy is begun. In addition to deciding on the sequence of treatment, the physician must consider the various modifications of the injection procedure that some physicians profess have various benefits. As before, comparative and objective studies of these treatment modifications have not been reported. This chapter discusses sclerotherapy treatment of varicose veins, perforator veins, and the SFJ and reviews the available literature. Variations in treatment are addressed, and illustrative cases are presented. A summary of the three schools of sclerotherapy is found in Table 9.1.
Injection Technique
Patient position
Standing
Although the previous description of the treatment of varicose veins seems simplistic, the actual treatment methods for achieving effective sclerotherapy are numerous. Until the 1950s, sclerotherapy was performed with the patient standing throughout the procedure. The purpose was both to distend the varicose vein, allowing easier needle insertion, and to produce firm thrombosis of the treated vein.46 Multiple disadvantages of varicose thrombosis were realized (see Chapter 8), and various methods were devised to limit postsclerotherapy thrombosis. Additionally, injecting sclerosing solution while the patient is standing forces the injection to occur against the hydrostatic pressure of a large column of blood. This may cause the solution to seep along the needle into the perivenous tissues, possibly leading to a chemical phlebitis or tissue necrosis.47
Another disadvantage of the total standing technique is the sclerosing solution may escape through a perforator vein and damage the deep veins, especially if more than 1.5 mL of sclerosing solution is injected in a single site.48 Another radiographic study has shown that an injection of 0.5 mL of contrast media travels rapidly (in 5 seconds) 8 cm distal to the injection site.49 Also, this amount of contrast does not completely fill the vein. An additional radiographic study of the standing position, using metrizamide (Amipaque) 150 as the contrast media (diluted to an isomolarity and specific gravity similar to that of polidocanol (POL)), showed that the injection of 1.5 mL remained in contact with a convoluted varicosity for approximately 10 seconds before flowing rapidly into the deep venous system through a presumed perforator vein (Fig. 9.2, A and B).50 In contrast, when the patient was supine, the contrast media extended proximally along the varicosity and remained relatively undiluted for more than 18 seconds (Fig. 9.2, C and D).50 However, injections in some patients, when using the latter technique, also resulted in the contrast media’s remaining in contact with the varicosity for a longer period with the patient in the standing position (Fig. 9.3). Therefore, multiple variables, including the type of varicosity, its location, the location of associated perforator veins, and the movements of the patient (with associated calf and foot muscle contraction) while standing, may all affect the distribution of the sclerosing solution. For these reasons, the standing technique is not recommended.
Standing and reclining
A modification of the standing technique, the standing and reclining technique, was described in 1926 by Meisen.51 In the standing position, the needle was inserted while the vein was distended. With the needle still in the vein, the patient reclined on a table and the leg was elevated. This produced a relative emptying of blood from the vein. The sclerosing solution was then injected into an ‘empty’ vein that was immediately compressed to prevent or minimize thrombosis.
One of the earliest methods used to limit thrombosis was that of isolating the injected vein segment with pressure placed above and below the needle insertion site after first milking the blood out of the vein.52 One of the first books on sclerotherapy treatment of varicose veins is Varicose Veins and Their Treatment by ‘Empty Vein’ Injection.53 In this book, Ronald Thornhill of London detailed his success with injection of a quinine solution into the elevated leg. He massaged the solution throughout the vein, injecting from distal to proximal. He even sclerosed ‘hair veins’ with a dilute solution. Unfortunately, he did not use compression except when ulcers were present, and his patients had to endure weeks of tender veins until they resolved in approximately 12 months.
Lufkin and McPheeters54 emphasized the importance of empty vein injections in a histologic evaluation of treated veins in 1932. Orbach55 has stressed the significance of compressing the vein to minimize thrombosis since 1943. Thus, these modifications are not new. They result both in improved efficacy and in a decreased incidence of complications when the treatment is directed at the SFJ.19 The improved efficacy may be the result of a longer length of sclerosis of the varicose vein, caused by gravitational flow of the sclerosing solution. However, recent evaluations comparing standing and reclining methods of treating varicose veins below the SFJ have not been performed.
Leg elevation (Fegan)
Another obvious disadvantage of the standing technique is the vasovagal reaction (see Chapter 8). To prevent the sequelae of a vasovagal reaction, Fegan56 recommended that patients sit at the end of the examining table with their legs hanging down while the physician, sitting in front on a low stool, inserts the needle. The leg is then raised while the patient fully reclines for 1 to 2 minutes to empty it of blood. The physician stands to support the raised leg, which is rested on the shoulder or against the chest, and the varicose veins are injected. With this or any technique that moves the patient after the needle is inserted, it is important to ensure that the needle is not displaced from the vein, either by fixing it to the skin with tape (if butterfly catheters or needles attached to syringes are used) or by holding the needle while the leg is raised. Since the varicose veins will collapse when the leg is raised, blood withdrawal must be checked as soon as possible after the leg is raised to ensure that the needle has not slipped out of the vein. The lack of spontaneous pulsatile flow from the needle without an attached syringe is proof of nonarterial placement of the needle.
To ensure that the sclerosing solution acts on the intended vein segment during injection, Fegan56 recommended applying pressure with fingers a few centimeters proximal and distal to the injection point. Finger pressure is maintained for 30 to 60 seconds, and the leg is then bandaged from the toes to the injection site. With this method, injections are made only at the points of fascial defects (which are thought to represent sites of IPVs). Injections proceed from distal to proximal sites, with each vein segment or fascial defect treated.
After injection of varicose veins in the elevated leg, compression should be applied immediately to prevent the vein’s filling with blood. This can be performed easily with the use of the following method. Before insertion of the needle, a compression stocking is placed over the foot and heel and allowed to bunch up at the ankle. After the needle is inserted into the varicosity, the leg is raised. Proper placement is then confirmed through blood withdrawal, and the sclerosing solution is injected. A foam pad is placed over the injection site and secured in place with foam or elastic tape. The compression bandage then can be advanced over the injection site and foam pad in a distal to proximal manner (Fig. 9.4). With this technique, radiographic studies after injection of 0.5 mL of contrast medium show that when the leg is raised above the horizontal plane, the contrast medium travels rapidly for 30 cm before reaching the deep venous system.49 The sclerosing solution is diluted and probably inactivated by the time it reaches the deep venous system (see Chapter 7). With this technique it may not be necessary to repeat injections every few centimeters in the varicose vein.
With the leg-raising technique the varicose vein would be presumed empty of blood, but this is not the case. Duplex examination demonstrates that the GSV is not totally emptied of blood, even with an 80-degree incline, although tributaries to the GSV are emptied at 45 degrees.57 In ‘huge’ varicosities, as much as 18 mL of blood can be withdrawn when the leg is raised 45 degrees above the horizontal.58 Therefore, Perchuk58 developed a method for ensuring an ‘empty’ vein. His method consists of inserting the needle into the varicose vein, elevating the leg 45 degrees, and then withdrawing blood through that needle into a syringe until further blood withdrawal is impossible. Then, a syringe with sclerosing solution is attached to the needle and the injection is made, followed by application of local pressure for 5 minutes. The use of compression bandages or stockings after treatment was not mentioned. A two-way stopcock may also be used for this technique. Perchuk, in an evaluation of 84 patients, found that this technique produced excellent results and limited all complications.58 Pigmentation, thrombophlebitis, and recurrence were very rare. Fegan,59 however, disagreed with Perchuk’s conclusions and stated that the vein would empty of blood if raised for a longer time and at a more acute angle.
Two-phase (Sigg) technique
A variation on the method described previously is the two-phase technique of Sigg.10 This variation involves the way the needle is inserted into the vein. Sigg recommended the needle be passed through the vein with the syringe unattached or with a finger placed over the hub and then slowly drawn back until the escape of blood indicates proper placement. The needle is left open and unobstructed while an assistant places a basin beneath it to catch the dripping blood. The leg is then raised above the horizontal plane, and bleeding stops. A syringe is then attached, and blood is withdrawn. After proper placement is confirmed by withdrawal of venous blood and the vein is emptied of blood, the sclerosing solution is injected and the vein compressed, as described above, with a stocking, bandage, or both. Since Sigg uses mainly iodinated iodine solutions, he developed this technique to ensure continual intravascular placement of the sclerosing solution (see Chapters 7 and 8).
Reclining
Another method for injection advocated since the 1920s is that of having the patient remain horizontal throughout the procedure.60 If the varicose veins easily collapse in this position, they can be marked with indelible ink before the procedure, while the patient is standing. A radiologic study has shown a 0.5-mL bolus of contrast medium injected into a varicose tributary of the GSV travels proximally 8 cm and remains within the vessel for approximately 2 minutes before being drawn into the deep venous system.49 The relaxation of the calf muscles permits the injected fluid to stay within the vein, since blood flow in this position is slow. Thus, this position produces the longest lasting and most uniform contact between the injected solution and the vein wall.
To produce a relatively bloodless vein during injection in the horizontal position, some authors advocate rubbing along the vein in both a proximal and distal direction away from the injection site.60 Manual compression is then maintained at the proximal and distal sites along the vein to prevent the vein segment from refilling with blood. After the injection, a compression pad and bandage are immediately applied to the treated vein segment.
Foam sclerotherapy
Since the earlier editions of this textbook, the use of foam sclerosants has increased dramatically. Far from the primitive techniques described by so many authors and well detailed in Wollmann’s history of sclerosing foams,61 it is now considered as a completely new treatment for varicose veins.62,63 Shaking the syringe60 or aspirating in a closed glass syringe,64 to quote only two of the well-known historic methods, are now obsolete. Three main options remain: high-speed beating in a carbon dioxide-rich atmosphere (Cabrera’s technique65), specific gas mixture combined with POL and passed through a patented sieve in an aerosol canister (Varisolve, Provensis Ltd., UK), and Tessari’s method, using the transfer between two syringes of sclerosant and room air. The latter technique offers different variations: a three-way stopcock as initially described66 (Fig. 9.5), a two-way female connector like in the DSS technique67 (Fig. 9.6), or an automated foaming device, Turbofoam (KreusslerPharma, France), described in Chapter 7, which has the ability to mix the sclerosant with different types of gases through the use of a three-way connector. The Tessari technique is the most common means for foam creation.68
Immediately following the injection of foam sclerosant, the bubbles displace blood and contact with the sclerosant and endothelium begins. Clinically, this is apparent as vasospasm within seconds or minutes, erythema of the feeding telangiectasias, or no immediate visible change (Table 9.2a Pt1). After several days, venous inflammation is present with thickening of the venous wall and presence of a sclerus. This is evidenced clinically by induration, erythema, and tenderness. Weeks to months later, fibrosis results in a progressive decrease in the diameter of the treated vein and clinically by the absence of the varicosity. Occasionally, a fibrous cord may be palpated (Table 9.2b Pt2). At times, complete clearance of the varicose veins does not take place, owing to either partial or total recanalization of the treated vein (Table 9.2c Pt3).
Table 9.2 A-C Pathophysiologic and clinical effects from foam sclerotherapy
|
|
|
|
|
|
Foam sclerotherapy is now regarded as far more efficaceous than liquid sclerotherapy for larger veins due to an increased time of contact between the sclerosant and the vein wall.68 The temporal relationship between foam bubbles and the endovenous wall is related to patient position, injection technique, foam viscosity, and the number of bubbles per milliliter.69 Hamel-Desnos et al67 investigated efficacy rates of a single treatment session of foam or liquid ultrasound guided sclerotherapy of GSVs. The induction of venous spasm was more common following foam sclerotherapy. At 3 weeks follow-up, reflux was absent in 84% of foam sclerotherapy treated veins and 40% of liquid sclerotherapy treated veins. A similar study was performed by Yamaki et al70 to investigate single treatment foam versus liquid sclerotherapy in GSVs and tributary veins. At 12 months, complete occlusion rates were 67.6% and 17.5% in the foam and liquid groups, respectively. Statistically significant increased rates of recurrent varicose veins and recanalization with reflux were identified in the liquid sclerotherapy cohort. A 2009 meta-analysis revealed a 76.8% efficacy of ultrasound-guided foam sclerotherapy (UGFS) as compared to a 39.5% efficacy rate for ultrasound-guided liquid sclerotherapy.71 An additional benefit from foam is its appearance on ultrasound as an intravenous contrast agent. Multiple randomized controlled studies comparing the incidence of adverse events with foam and liquid ultrasound-guided sclerotherapy of the saphenous veins have shown no statistical difference between these techniques.67,71,72
A metanalysis by Van den Bos and colleagues73 compared occlusion rates following endovenous laser ablation (all wavelengths included), radiofrequency (RF) ablation, UGFS, and high ligation with stripping from 64 studies and 12,320 limbs. At 3 years, success rates were 94.5% for laser ablation, 84.2% for RF, 77.4% for UGFS, and 77.8% for high ligation with stripping. After 5 years, the respective treatment success rates were 95.4%, 79.9%, 73.5%, and 75.7%. The authors found efficacy for high ligation and stripping, RF ablation, and UGFS were equal, but endovenous laser ablation therapy (EVLT) was more effective than the other three regimens.
All foams are not the same, as explained by Wollmann.61 Even if prepared with the same agent (foams can be produced only with detergents – namely, STS and POL and, rarely, sodium morrhuate), foams can have different properties depending on the mode of preparation and the gas to air ratio (dilution factor). Foams are wet or dry, accordingly. This difference is thought to have some impact on efficacy. Drier foams tend to break down on passage through a needle while wet foams act more like liquids. Between these extremes, foam is relatively stable and will displace blood from the vein. Liquid sclerosant to gas dilution ratios of 1 : 4 (1 part liquid to 3 parts gas) or 1 : 5 (1 part liquid to 4 parts gas), have been found to produce the most stable foams.74 Currently, most physicians use a foam prepared just prior to injection with a method derived from Tessari and a ratio of solution to air varying from 3 to 5 mL of air to 1 mL of solution (we recommend 4 mL). Some standardization has happened spontaneously.
Foam stability
Foam stability is affected by foam composition, foam volume, and injection technique.75 Composition variables, including the homogeneity of bubble size, viscosity, and temperature, all influence the ‘quality’ and longevity of foam (Table 9.3).76 Heat increases the stability of foam.77
Bubble size is inversely related to the difference in density between a liquid and gas, as represented in the equation below.76
where
Carbon dioxide is 1.5 times denser than room air; therefore, foam bubbles prepared from carbon dioxide are smaller than those of air. Foam bubbles produced via turbulent flow in the Tessari technique and the double syringe system are smaller (less than 100 µm) in size as compared to the larger bubbles produced in the Monfreux technique. This smaller bubble size is associated with an increased surface area of sclerosant, increased displacement of blood inside the vessel, and decreased likelihood of mixing with blood following the initial injection. Therefore, an increased amount of sclerosant can be delivered to the endothelial cells.78,79 Interestingly, the Monfreux method of foam creation has been associated with an increased incidence of side effects. It is speculated that the larger bubbles produced in this method advance more readily in the venous system.78
The majority of phlebologists utilize readily available room air for foam creation in sclerotherapy; however, carbon dioxide is becoming increasingly popular.80 Carbon dioxide foam bubbles quickly disintegrate; this effect is more pronounced as the sclerosant to gas ratio is increased.61 The following equation describes foam stability in vivo:
Carbon dioxide has a much greater diffusibility into blood as compared to nitrogen (the dominant gas in room air), and as a result, the foam-half life is reduced for carbon dioxide. When carbon dioxide is mixed with oxygen for foam creation, the foam-half life is increased due to the decreased diffusibility of this mixture.81
Room air foam half-life varies according to the percent of sclerosant solution. In the study by Rao and Goldman,82 they found a 1% concentration of STS or POL had the maximal foam half-life (90 and 120 seconds, respectively) (Tables 9.4 and 9.5). We recently discovered carbon dioxide foam half-life did not vary according to the concentration of sclerosant solution; however, a mixture of 77% carbon dioxide/23% oxygen did. We also found that foam half-life for room air is over three times longer than carbon dioxide half-life and 1.5 times longer than a combination of 70% carbon dioxide/30% oxygen (see Table 9.3).83
Table 9.4 Times for 0.5 mL of sodium tetradecyl sulfate (STS) to settle from a foam mixture containing 1.0 mL of various STS concentrations*
Table 9.5 Times for 0.5 mL of polidocanol (POL) to settle from a foam mixture containing 1.0 mL of various POL concentrations*
Silicone coating is present in syringes and syringe connectors to provide lubrication, but silicone is also an anti-foaming agent. Prior studies by Rao et al and Lai et al, have shown the amount of silicone in syringe connectors does not affect foam stability; however, foam stability varies between syringe manufacturers due to variances in the silicone content of their syringes.82,84 Hill85 investigated the effect of a 5 µm syringe filter on carbon dioxide foam half-life. In the absence of the filter, foam half-life was 22.7 and 30.1 seconds for STS 2% and POL 2%, respectively. Half-life was prolonged to 35.9 and 48.9 seconds, respectively, with the addition of a 5 µm filter. Of note, carbon dioxide foam stability was greater in POL versus STS throughout the study.
Foam has a spontaneous evolution before and after being injected in varicose veins. Before injection, small bubbles tend to group as bigger units (known as LaPlace’s law) and after some time foam is replaced by large bubbles whose effect will be what was observed with Orbach’s air-block. Stability of the foam can be evaluated by several techniques,82 and one should not talk about foam when prepared more than 90 seconds in advance. The preparation of foam does not change the concentration of sclerosing agent. This is completely different from what happens to the foam when injected. If injected into an isolated segment, a plug of foam is created and behaves as in a syringe, remaining in contact with the endothelium long enough to destroy it and induce venospasm. As the foam is forced from the contracting segment of vein, it mixes at the expanding interface with blood. This is responsible for dilution of foam and the scattering of bubbles, and surface sclerosing agent is rapidly deactivated by attachment to plasma protein and cell membranes. This explains why bubbles, when found far from the injection site for example, in the lung, heart, or brain consist of air and do not carry detectable amounts of sclerosing agent or have any sclerosing properties.86
Regarding the use of foam, the trend in Europe is to develop a consensus for volumes and concentrations.80,87 At the 2nd European Consensus Meeting on Foam Sclerotherapy, experts agreed than no more than 10 mL of foam per injection should be injected into a GSV. The range of volume injected into the GSV varied between less than 2 mL up to 10 mL per injection. The maximum recommended volume of foam per leg and per session was felt to be 10 mL. The Monfreux technique of foam creation was no longer recommended for any subtype of vein.80 In France, there appears to be a reduction in concentrations,88 with vessel spasm used as an indicator for the correct amount of foam injected. However, this option is true only for a proximal and direct injection of terminal parts of the saphenous veins. We have previously advocated for a more distal approach62 with placement of an open vein access (‘butterfly’ needle or catheter; Figs 9.7 and 9.8), filling the vein with relatively low volume concentrations, and massaging to the desired area under duplex control (Fig. 9.9). With several years of experience this is no longer deemed necessary. The necessary volume can be estimated from the diameter and the length of vein, as indicated in Table 9.6. In our practice, however, we do not currently use volumes above 10–12 mL in a single vein. It should not be forgotten that although foam is not air and usually occupies the entire vessel lumen, foam floats, so that in large-diameter veins it will principally be in contact with the upper part of the vein, where gravity leads it (Fig. 9.10). The only solution to this problem is a reduction in the diameter, which can be obtained by compression, leg elevation, or induction of venous spasm. Ten to thirty milliliters of normal saline can be injected perivenously, in a technique similar to tumescent anesthesia for endovenous laser or RF ablation, to cause venous compression and decrease recurrence rates.89
Figure 9.10 Effects of Archimedes’ law on foam contact with venous wall in veins of various diameters.
The most common technique for foam sclerotherapy is via ultrasound guidance81 and using the direct puncture technique.80 While many authors employ short catheters, long catheters with balloon tips have become more prevalent due to a possible increased efficacy. However, long catheters may cause an increased incidence of deep venous thrombosis81 due to a passage through perforators, even if foam is re-aspirated at the end of the procedure. The recommendations from the 2nd European Consensus Meeting on Foam Sclerotherapy is to inject the GSV at the proximal thigh if using the direct puncture technique and distal to the knee if using long catheters. For the SSV, injection should be at the level of the mid calf in order to minimize adverse events including canulization of the popliteal artery.80
Even if every phlebologist using foam sclerotherapy has been impressed by results (see Case Study 13 later in this chapter), evidence-based medicine applies to phlebology too and controlled trials are needed to demonstrate the validity of the technique. Efficacy of foam sclerosants is more substantially documented today than it was when writing the previous editions of this textbook and evidence is now available.67,70,90–92 Cabrera et al93 have followed 500 lower limbs treated with their unique carbon dioxide-foam mixture, with no greater than 81% of the GSV and 96.5% of the superficial branches remaining closed at over 3 years. Results have not been as impressive when room-air-generated foam is used. Fruillini and Cavezzi78 found an 88% success rate when the foam was generated with the glass syringe/Monfreux technique versus 93% when generated with the Tessari technique. Although their follow-up was 20 to 180 days, it is clear that the method for generating foam is important regarding treatment efficacy. Even Tessari reports a 74% efficacy of complete obliteration in a 2-year evaluation of 38 GSVs and SSVs and 194 collateral branches treated.94 In a randomized controlled trial, proprietary pharmaceutical polidocanol microfoam (PPPM; Varisolve) was compared with superficial vein surgery or sclerotherapy in 654 patients with moderate to severe saphenous vein (GSV or SSV) incompetence. The overall success rates were 83.4% for PPPM and 88.1% for control at 3 months, and 78.9% and 80.4%, respectively, at 12 months; at neither time point was the difference significant.95
A 3-year follow-up study in UGFS using either STS or POL for the GSVs, SSVs, and their tributaries revealed a 52.4% success rate. Veins that failed the primary treatment session were re-treated. The 3-year success rate for this group was increased to 76.8%.96 A 5-year 56% efficacy rate was found in a prospective study investigating UGFS prepared from STS of the GSVs. This protocol consisted of weekly foam sclerotherapy treatments until reflux was no longer detected by ultrasound. Additional treatments were performed if recanalization was detected. Currently, this study contains the longest follow-up duration of all published studies on foam sclerotherapy.97 In a recent meta-analysis that included 9000 patients, the median efficacy of foam sclerotherapy was 87% with a median recurrence rate of 8%.68
Darke and Baker98 investigated the number of UGFS treatment sessions required for clinical evidence of complete occlusion of varicose veins. Clinical complete occlusion rates at 6 weeks following the last treatment were as follows: 74.1% with a single treatment, 89.1% with two treatments, and 89.5% with three treatments. O’Hare et al99 found no difference in efficacy rates at 6 month in veins of less than or greater than 7 mm in diameter that were treated with UGFS. However, Myers et al96 found that treatment success was decreased in veins greater than 6 mm as compared to veins of less than 5 mm. This report also concluded success rates were higher in GSVs versus SSVs.
Multiple studies have investigated the influence of various sclerosant concentrations in relation to the efficacy rate of foam sclerotherapy. Efficacy rates were highest for POL 1.5% or STS as compared to 3% or more dilute concentrations in a study investigating saphenous veins and their tributaries.96 A similar study investigating POL for UGFS of GSVs less then 8 mm found short term (3 week) success rates of 96% and 88% in subjects receiving POL 3% foam and POL 1% foam, respectively (difference was not statistically different). After 2 years, the success rates were 69% in patients treated with POL 3% foam and 68% in those treated with POL 1% foam.88 Ceulen et al100 initially found a significant difference in efficacy rates of UGFS between 1% and 3% POL foam at 1-year follow-up (69.5% and 80.1%, respectively). However, when these subjects were followed for 2.5 years, there was no difference in efficacy between the two concentrations of POL (66.7% and 66.8%, respectively).101 No exclusion criteria were made in this study with regards to the diameter of the GSV.100,101
Side effects
A foam bolus can even occur when a small quantity of foam is injected. Hill et al75 showed that leg elevation, but not manual pressure of the SFJ, decreased the migration of foam in sclerotherapy in UGFS of the great saphenous vein. At least this could ensure that bubbles will be washed of their sclerosing molecules, but will release much bigger bubbles. Other methods to decrease foam migration include multiple, sequential injections of foam sclerosant volumes less than 0.5 mL.102 A meta-analysis investigating side effects in over 9000 patients by Jia et al68 found the median rates of deep venous thrombosis and pulmonary embolus were less than 1% each. The median values of visual changes and headache were 1.4% and 4.2%, respectively. Chest tightness and coughing occurred in less than 1%. In a large, prospective, multicenter study of foam sclerotherapy in 1025 patients the incidence of migraine was 0.78% (with aura 0.59%;.19% without aura), visual disturbance 0.68%, chest tightness 0.68%, chest tightness with visual disturbance 0.49%, deep venous thrombosis 0.98%, pulmonary embolism 0.1%, and transient ischemic attack 0.1%.103
A recent study of patients with incompetent GSVs treated with UGFS created from either carbon dioxide or room air, in a 1 : 4 sclerosant to gas dilution ratio, demonstrated decreased incidences of foam-bubble-related side effects including chest tightness (3.1% to 18%), cough (1.6% to 16%), and dizziness (3.1% to 12 %). There was a trend towards decreased visual disturbances in the carbon dioxide versus room air group (3.1% to 8.2%), though this difference was not found to be statistically significant. There were no differences in vital signs or echocardiogram (ECG) changes between the two cohorts. An overall 71.79% decrease in bubble-related side effects (as compared to room air) was attributed to the carbon dioxide foam.104 When cerebral emboli were monitored via transcranial Doppler ultrasound in patients treated with foam created from either room air or a 70% carbon dioxide/30% oxygen mixture, no statistical differences were found between these two cohorts with regard to the rate of high intensity transient signals in the middle cerebral artery.105
One can speculate that the decreased upstream foam-related side effects are attributable to the short carbon dioxide foam half-life83 and the increased diffusibility of this gas into blood in comparison to nitrogen and oxygen.81,83 In a study of 116 patients with stasis ulcers, the incidence of visual changes and cough occurred in less than 2% of patients treated with carbon dioxide created UGFS.106 In a large multicenter prospective study by Guex et al, visual disturbances occurred in 0.28% of patients treated with foam sclerotherapy created using room air.107
Intravenously injected bubbles of less than 10 µm do not produce symptoms in patients, regardless of the presence of a patent foramen ovale.108 Ceulen et al109 noted foam microbubbles created from room air appeared in the right atrium and ventricle 0.75 to 15 minutes following injection. In the small study by Morrison et al,110 foam bubbles were identified in the deep venous system and the right atrium within 10 seconds of the initial injection of foam sclerotherapy into a 1-mm telangiectatic vein. This finding was reproducible in all 15 subjects. In a related study, these bubble emboli ‘showers’ could last minutes and were present in the left side of the heart in 33% of subjects, indicating a shunt. Of interest, 57% of this group of patients showed transcranial Doppler evidence of bubble emboli.111
Four cases of transient ischemic attacks and cerebrovascular events have been reported in the literature. All patients had examples of right to left cardiac shunting, such as patent foramen ovale and atrial septal defects, discovered on further workup.103,112,113 These bubbles can appear in the middle cerebral artery in under 35 seconds.114 Treatment for foam-induced neurological events includes administration of 100% oxygen followed by immediate transfer to an emergency department and the initiation of hyperbaric oxygen therapy.113 As the dominant gas in room-air bubbles is nitrogen, foam bubble half-life is decreased as the concentration of oxygen increases and the nitrogen decreases.115 Theoretically, in the event of cerebral emboli, the osmotic diffusion of oxygen and nutrients should be able to compensate for small bubbles but not larger bubbles.116
Deep venous thrombosis is a rare occurrence in foam sclerotherapy with an incidence of 0.015%.107 Shadid et al117 recommends maintaining a high index of suspicion for the development of deep venous thrombosis when superficial thrombophlebitis occurs distant from the treatment area. Pulmonary embolus have been reported following UGFS.103,118 Infection is a rare event following foam sclerotherapy, but cases of cellulitis and Klebsiella sepsis have been reported.119
Our technique for the treatment of reticular and telangiectatic leg veins
Our classification for veins are as follows: varicose veins are torturous and larger than 4 mm, reticular veins range from 1 to 4 mm, and telangiectactic veins are less than 1 mm. For the most successful outcome of foam sclerotherapy of telangiectatic leg veins, the feeding incompetent reticular veins must be treated simultaneously. At our clinic, we initiate with treatment of refluxing veins, the largest veins, and proceed in a proximal to distal fashion. The double syringe system with room air in a 1 : 5 dilution (1 part sclerosant solution: 4 parts gas) is our preferred method for foam creation. For reticular veins between 1 and 3 mm, we prefer STS 0.25% or, alternatively, POL 0.25% to 0.5%. We increase the concentration of STS to 0.5%, and POL up to 1%, for veins 3 to 5 mm in diameter. Telangiectatic leg veins are treated with liquid STS 0.25%, liquid POL 0.5%, or glycerin 72% with lidocaine 1% or without epinephrine (adrenaline). Our patients remain in the supine position without leg elevation for the duration of the treatment. Following treatment, the patient remains supine as nursing staff apply 30 to 40 mmHg compression stockings. Immediate ambulation for 15 to 30 minutes is required. For the next week, 24 hours a day (for one author RAW, only during waking hours), the patient remains in their compression stockings.120,121
Other applications of foam sclerotherapy
Ulcers
Foam sclerotherapy is also effective in the treatment of venous ulcers. Cabrera et al106 investigated carbon dioxide-POL foam in 116 patients with venous stasis ulcers and found complete resolution at 6 months in 83% of patients. Either the saphenous veins, perforator veins, or a combination were injected under ultrasound guidance. The mean time for complete resolution of an ulcer was 2.7 months. Long-standing ulcers (over 24 months), size greater than 2 cm, patient age over 65 years old, a history of venous surgery, and incompetence of the deep venous system were negative prognostic indicators.
Venous Malformations
Foam sclerotherapy can decrease the progression and size of venous malformations, including Klippel-Trénaunay syndrome.79 In a study by Yamaki et al,122 subjects with symptomatic venous malformations, including limited, infiltrating, and complex-combined variants, received ultrasound guided foam or liquid sclerotherapy. The sclerosants investigated were 1% POL foam or liquid for treatment of the superficial component and 10% ethanolamine oleate for the deep components of the venous malformation. As complete resolution of venous malformations would not be realistic in all patients in this study, patients received enough sessions until patient-perceived cosmetic satisfaction was obtained or when no further benefit was anticipated. A significant decrease in volumes of sclerosants (both POL and ethanolamine oleate) were found in the foam cohort. On 6-month follow-up duplex evaluation, increased rates of disappearance (defined as occluded and shrunken venous space) and partial recanalization (defined as partially recanalized and partially shrunken venous space) were greater in the foam group versus the liquid group (45% and 45% versus 25% and 15%).
Combination therapy
Foam sclerotherapy with saphenofemoral ligation versus high ligation, stripping, and multiple phlebectomies was evaluated by Kalodiki et al.123 With 3-year follow-up, there was no statistical difference in the recurrence rates between these two treatment regimens on Doppler ultrasound evaluation.
Foam sclerotherapy can be combined with endovenous laser ablation at the time of surgery or can be performed at follow-up visits. In a study by King, UGFS was combined with either the 980 nm or 1320 nm endovenous laser for the treatment of incompetent saphenous veins. At 1-month follow-up, treatment success was seen in 97% of patients.124 Further long-term data and controlled clinical trials will be necessary to evaluate whether combined endovenous laser ablation combined with foam sclerotherapy is superior to endovenous laser ablation alone. Any varicosities remaining at 6 weeks post procedure and distal to the site of endovenous ablation should, in our experience, be treated by foam sclerotherapy.
Contraindications
Patent Foramen Ovale
Patent foramen ovale (PFO) is present in 27% of the general population,111,112,125 and decreases in prevalence with increasing age. Transesophageal echocardiogram with contrast is the recommended screening test for the detection of PFO, but transcranial Doppler ultrasound is almost as sensitive.126 Right to left cardiac shunting can occur in the presence of a PFO, atrial septal aneurysm, or any opening between the atria, ventricles or the great vessels.127 Pulmonary arteriovenous malformations can lead to extracardiac shunting and occur in 10% of the population.111 All of the previously listed forms of shunting can result in cerebral vascular system emboli. The incidence of cryptogenic stroke is greater in patients of all ages with PFO127 as compared to the general population.128 Two prospective studies found migraines associated with an aura occur more commonly in patients with PFO.129,130
In a report by Morrison et al,110 15 patients were screened for a PFO with an ECG prior to foam sclerotherapy. Allthough echocardiogram screening revealed no PFO, intraoperative transthoracic ECG monitoring revealed the presence of four PFOs which were accentuated because of the increased visibility of foam. A 2010 study by Wright et al126 found 58.8% of patients with varicose veins (CEAP C3-5) had a right to left cardiac shunt as evidenced by the appearance of bubbles in the middle cerebral artery on transcranial Doppler (at rest or with a Valsalva maneuver) using agitated saline. Next, 61 patients with a right to left heart shunt were treated with UGFS with 1% POL foam created from a 70% carbon dioxide/30% oxygen mixture; 89% had evidence of bubble emboli in their cerebral vascular system. No patients were symptomatic throughout this study. In a study of 3259 patients treated with UGFS, 7 patients (0.21%) experienced foam-related side effects including visual disturbances, chest tightness, and migraine with aura. Of these seven patients, five tested positive on transcranial Doppler examination, indicating the presence of right to left cardiac shunting such as with a PFO.131
A known symptomatic PFO is considered an absolute contraindication for foam sclerotherapy by the 2nd European Consensus Meeting on Foam Sclerotherapy. However, the committee agreed that it is not necessary to screen for a PFO in an asymptomatic patient prior to foam sclerotherapy treatment.80
Thromboembolism and Thrombophilia
An absolute contraindication for foam sclerotherapy is the presence of an acute deep or superficial venous thrombosis. If a patient has a prior history of a deep venous thrombosus or thrombophilia, it is considered a relative contraindication. These patients should undergo a full workup to determine the etiology of thrombophilia, treatment for 7 days with prophylactic low molecular weight heparin, and be administered limited volumes and decreased concentrations of foam sclerotherapy.80 In the study by Wright el al,95 the incidence of deep venous thrombosis decreased when small volumes were utilized per injection and the injection was ceased and compression applied when foam was present 5 cm from the saphenofemoral or saphenopopliteal junction.
Migraine
A straightforward migraine is not considered a contraindication to foam sclerotherapy.80 However, we found that patients with history of ophthalmic migraine (see Chapter 8) where likely to have more frequently visual disturbances after foam sclerotherapy; this must be explained at the time of informed consent.
Other injection techniques
Air bolus
The air-bolus technique was first advocated by Orbach60 to ensure that sclerotherapy treatment of varicose veins occurred with minimal thrombosis. The rationale for instilling air before injecting the sclerosing solution is that clearing the vessel of blood allows undiluted contact to occur between the solution and the vessel wall. This procedure was thought to minimize the concentration and quantity of solution required to produce endothelial injury. A comparative evaluation of this technique demonstrated enhanced efficacy of treatment regardless of the type of sclerosing agent used.132 In reality, the potential complications of air embolism, as addressed in Chapter 8, are nil. A disadvantage of this technique is that air proximal to the sclerosing solution in the syringe causes compression of the solution, producing leakage of solution from the needle after depression of the plunger has stopped. This may cause extravasation of solution on needle withdrawal.
Radiologic studies have shown air-bolus injections into large varicose veins in the area of the GSV are ineffective in clearing the vessel of blood, even when 0.5 mL of air is injected immediately before the injection of contrast medium.49 In addition, the air inhibits complete and even filling of the varix both proximal and distal to the injection site. In smaller varicosities, injected air forms several bubbles and does not act as a bolus. It also moves independently of the position of the patient and is not totally under the influence of gravity. Therefore, the air-bolus technique may not be advantageous for use in treating varicose veins.
