[level-membership-for-basic-science-category]67
Clinical disorders of lipid metabolism




Classification
Currently there is no satisfactory comprehensive classification of lipoprotein disorders. Genetic classifications have been attempted but are becoming increasingly complex as different mutations are discovered (Table 67.1). Familial hypercholesterolaemia (FH), which may present with xanthelasma (Fig 67.1), tendon xanthomas, severe hypercholesterolaemia and premature coronary heart disease, may be due to any of over 500 different mutations of the LDL receptor gene. Mutations of the apolipoprotein (apo) B gene can give an identical syndrome. Familial hyperchylomicronaemia, which presents with recurrent abdominal pain and pancreatitis, may result from genetic mutations of the lipoprotein lipase or apo C-II genes. Eruptive xanthomas (Fig 67.2) are characteristic of hypertriglyceridaemia.
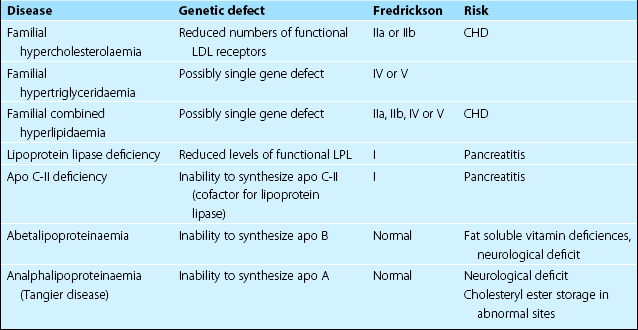
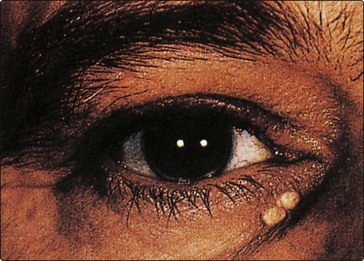
Fig 67.1 Xanthelasmas in younger individuals (age <40 years) usually indicate hypercholesterolaemia. In the elderly they do not carry the same significance.

 Primary – when the disorder is not due to an identifiable underlying disease.
Primary – when the disorder is not due to an identifiable underlying disease.
 Secondary – when the disorder is a manifestation of some other disease.
Secondary – when the disorder is a manifestation of some other disease.
Primary
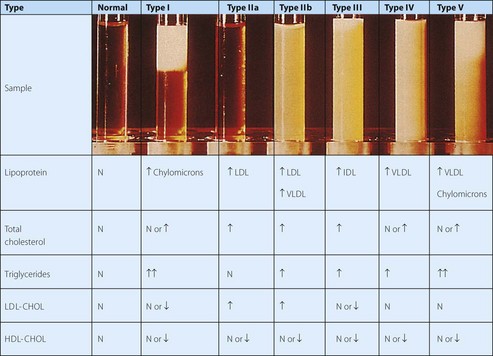
The Fredrickson or World Health Organization classification is the most widely accepted for the primary hyperlipidaemias (Fig 67.3). It relies on the findings of plasma analysis, rather than genetics. As a result, patients with the same genetic defect may fall into different groups, or may change grouping as the disease progresses or is treated (Table 67.1). The major advantage of this classification is that it is widely accepted and gives some guidance for treatment.
Secondary
Secondary hyperlipidaemia is a well-recognized feature of a number of diseases (Table 67.2) that divide broadly into two categories:
Table 67.2
Common causes of secondary hyperlipidaemia
| Disease | Usual dominant lipid abnormality |
| Diabetes mellitus | Increased triglyceride |
| Alcohol excess | Increased triglyceride |
| Chronic renal failure | Increased triglyceride |
| Drugs, e.g. thiazide diuretics | Increased triglyceride |
| Hypothyroidism | Increased cholesterol |
| Nephrotic syndrome | Increased cholesterol |


Atherogenic profiles
 Clinical note
Clinical note
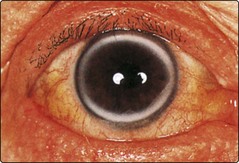
The physical signs of the hyperlipidaemias are not specific for any particular disease and may sometimes be present in normolipidaemic patients, e.g. arcus senilis (Fig 67.4). Their presence is, however, highly suggestive of raised lipids. Tendon xanthomas (Fig 67.5) are particularly associated with familial hypercholesterolaemia.

Case history 54
A 53-year-old man was found to have the following results on a fasting blood sample:

A non-smoker, his blood pressure was 145/95 mmHg and he was obese with central fat distribution.



[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]67
Clinical disorders of lipid metabolism
Classification
Currently there is no satisfactory comprehensive classification of lipoprotein disorders. Genetic classifications have been attempted but are becoming increasingly complex as different mutations are discovered (Table 67.1). Familial hypercholesterolaemia (FH), which may present with xanthelasma (Fig 67.1), tendon xanthomas, severe hypercholesterolaemia and premature coronary heart disease, may be due to any of over 500 different mutations of the LDL receptor gene. Mutations of the apolipoprotein (apo) B gene can give an identical syndrome. Familial hyperchylomicronaemia, which presents with recurrent abdominal pain and pancreatitis, may result from genetic mutations of the lipoprotein lipase or apo C-II genes. Eruptive xanthomas (Fig 67.2) are characteristic of hypertriglyceridaemia.
Fig 67.1 Xanthelasmas in younger individuals (age <40 years) usually indicate hypercholesterolaemia. In the elderly they do not carry the same significance.
Primary – when the disorder is not due to an identifiable underlying disease.
[/not-level-membership-for-basic-science-category]
