Cyst, Clear
Synonyms/Description
Etiology
Premenopausal
Postmenopausal
Ultrasound Findings
Differential Diagnosis
Clinical Aspects and Recommendations
In Premenopausal Women
In Postmenopausal Women
Figures
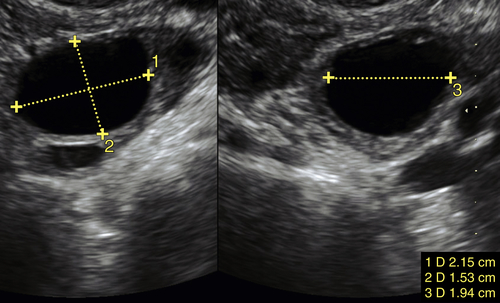
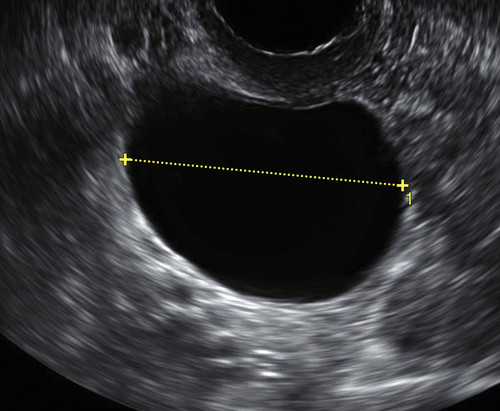
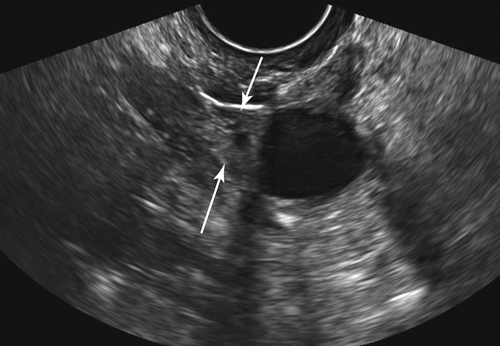
Figure C4-3 Differential diagnosis—paraovarian cyst (see Paratubal or Paraovarian Cysts). Note that the unilocular cyst is located adjacent to the ovary (arrows).
Figure C4-4 Differential diagnosis of large peritoneal inclusion cyst (see the section on complex cysts). This cyst is neither totally anechoic nor unilocular. It seems to take on the shape of the peritoneal space, a characteristic that is typical of a peritoneal inclusion cyst secondary to adhesions after pelvic surgery.
Suggested Reading
Greenlee R.T., Kessel B., Williams C.R., Riley T.L., Ragard L.R., Hartge P., Buys S.S., Partridge E.E., Reding D.J. Prevalence, incidence, and natural history of simple ovarian cysts among women >55 years old in a large cancer screening trial. Am J Obstet Gynecol. 2010;202 373.e1-9.
Levine D., Brown D.L., Andreotti R.F., Benacerraf B., Benson C.B., Brewster W.R., Coleman B., DePriest P., Doubilet P.M., Goldstein S.R., Hamper U.M., Hecht J.L., Horrow M., Hur H.C., Marnach M., Patel M.D., Platt L.D., Puscheck E., Smith-Bindman R. Society of Radiologists in Ultrasound. Management of asymptomatic ovarian and other adnexal cysts imaged at US Society of Radiologists in Ultrasound consensus conference statement. Ultrasound Q. 2010;26:121–131.
Valentin L., Ameye L., Franchi D., Guerriero S., Jurkovic D., Savelli L., Fischerova D., Lissoni A., Van Holsbeke C., Fruscio R., Van Huffel S., Testa A., Timmerman D. Risk of malignancy in unilocular cysts: a study of 1148 adnexal masses classified as unilocular cysts at transvaginal ultrasound and review of the literature. Ultrasound Obstet Gynecol. 2013;41:80–89.