Chapter 237 Circumcision (Male; Newborn and Infant)
REQUIRED EQUIPMENT
Electrosurgical devices should never be used in conjunction with any of the clamp-based procedures.
TECHNIQUE
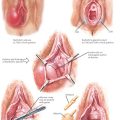
Plastibell
With the dissection of the foreskin free of the glans completed, the Plastibell string is placed as a loop near the base of the penis. The bell is placed under the foreskin, over the glans. This may be facilitated by upward traction on the edges of the foreskin grasped by hemostats and by downward pressure on the stem of the bell. When in a correct position, the bell should rest against the corona. The foreskin is pulled upward, ensuring even placement and positioning that leaves the groove in the bell well below the apex of the dorsal slit. The bell should move freely over the glans. While maintaining these relationships, the string is brought into position, resting in the groove of the bell. The string should be pulled firmly and all aspects should be rechecked before the string is tightened maximally. Tension on the string is maintained for at least 30 seconds and then a square knot is placed.
CPT CODE(S)
Blass EM, Hoffmeyer LB. Sucrose as an analgesic for newborn infants. Pediatrics. 1991;87:215.
Marshall RE. Neonatal pain associated with caregiving procedures. Pediatr Clin North Am. 1989;36:885.
Strimling BS. Partial amputation of glans penis during Mogen clamp circumcision. Pediatr. 1996;97:906.
American Academy of Pediatrics, Committee on Fetus and Newborn, Committee on Drugs, Section on Anesthesiology, Section on Surgery, Canadian Paediatric Society. Prevention and management of pain and stress in the neonate. Fetus and Newborn Committee. Pediatrics. 2000;105:454. 461.
American College of Obstetricians and Gynecologists. Circumcision. ACOG Committee Opinion 260. Obstet Gynecol. 2001;98:707.
Baskin LS, Canning DA, Snyder HM, Duckett JW. Treating complications of circumcision. Pediat Emerg Care. 1996;12:62.
Benini F, Johnston CC, Faucher D, Aranda JV. Topical anesthesia during circumcision in newborn infants. JAMA. 1993;270:850.
Clair DL, Caldamone AA. Pediatric office procedures. Urol Clin North Am. 1988;15:715.
Kaweblum YA, Press S, Kogan L, et al. Circumcision using the Mogen clamp. Clin Pediatr. 1984;23:679.
Niku SD, Stock JA, Kaplan GW. Neonatal circumcision. Urol Clin North Am. 1995;22:57.
Reynolds RD. Use of the Mogen clamp for neonatal circumcision. Am Fam Physician. 1996;54:177.
Task Force on Circumcision, American Academy of Pediatrics. Circumcision policy statement. Pediatrics. 1999;103:686.
Warner E, Strashin E. Benefits and risks of circumcision. Can Med Assoc J. 1981;125:967. 992.
Wolkomir MS. Technique for freehand newborn circumcision. J Fam Pract. 1996;42:447.