Circuit A
STATION 1
This station assesses your ability to elicit clinical signs:
STATION 2
This station assesses your ability to elicit clinical signs:
STATION 3
This station assesses your ability to elicit clinical signs:
STATION 4
This station assesses your ability to elicit clinical signs:
CLINICAL SCENARIO
Auscultation of the chest is normal with no wheeze. The expiratory phase is normal.
You present your findings as a child with atopic eczema and a normal chest examination.
What do you say to the examiner?
You are asked to explain to his mother how to manage the skin complaint. How would you do this?
STATION 5
This station assesses your ability to elicit clinical signs:
STATION 6
This station assesses your ability to assess specifically requested areas in a child with a developmental problem:
STATION 7
This station assesses your ability to communicate appropriate, factually correct information in an effective way within the emotional context of the clinical setting:
STATION 8
This station assesses your ability to communicate appropriate, factually correct information in an effective way within the emotional context of the clinical setting:
STATION 9
This station assesses your ability to take a focused history and explain to the parent your diagnosis or differential management plan:
COMMENTS ON STATION 1
DIAGNOSIS: PERSISTENT DUCTUS ARTERIOSUS
Every candidate has a fear that they will have little positive (or negative) to say to the examiner because they have been unable to examine the child properly. Even worse, they have examined the child properly and still have nothing to say! There are numerous learning points to remember in this type of station and if you remember a few you should always be able to give a professional answer.
1 APPROACH
Ask mother to show the child a colourful book while you listen to their chest.
Tap a wooden tongue depressor on the desk to attract attention.
Ask the child if you can guess what they had for breakfast by listening to their abdomen (and chest) with your stethoscope.
Start listening to teddy’s heart, lungs, abdomen, etc., or mother’s arm, leg, etc., so the child feels more comfortable.
If you say, ‘May I listen to your heart?’ and the child says ‘No’ then you have dug a large hole for yourself. ‘I am going to …’ should avoid this catastrophe.
2 OBSERVATION
We note that she sits without oxygen and is not cyanosed or dyspnoeic.
• pulmonary artery (PA) banding;
• a Blalock-Taussig (BT) shunt;
COMMENTS ON STATION 2
DIAGNOSIS: KIDNEY TRANSPLANT
Causes of chronic renal failure
| Disease | Cause | Features |
|---|---|---|
| Renal scarring | Multiple UTIs Vesicoureteric reflux | Has the child got spina bifida? |
| Glomerulonephritis | Henoch-Schönlein purpura | Any joint swelling or arthralgia? |
| Vasculitides | Purpura? | |
| Hereditary | Polycystic kidney disease | Are the parents well? |
| Cystinosis | Hearing difficulty? | |
| Alport’s syndrome | ||
| Congenital dysplasia | ||
| Systemic | Tumours | |
| SLE | Butterfly rash |
CAN YOU …
List the investigations you would perform in a child you suspect has chronic renal failure?
| Pre-treatment | Treatment | Post-treatment PASS |
|---|---|---|
| Hypertension | Control medically: Beta-blocker (care asthma) Furosemide (care potassium) Must involve nephrologists |
Dialysis – complications Peritonitis Volume depletion Dialysate leakage Transplant -complications Infection – particularly CMV Must prevent UTI Rejection Immunosuppression |
| Metabolic acidosis | Sodium citrate solutions (care: sodium may worsen hypertension) | |
| Growth failure | Growth hormone | |
| Renal osteodystrophy | Dietary phosphate restriction Phosphate binders Vitamin D |
|
| Uraemic symptoms (anorexia, nausea and lethargy) | Dietary protein restriction | |
| Anaemia | Erythropoietin | |
| Seizures (hypertensive or electrolyte imbalance) | ||
| If poor concentrating power: | ||
| Polyuria | ||
| Salt wasting |
REMINDER
Renal osteodystrophy
1. Poorly functioning kidneys unable to convert (hydroxylate) vitamin D to its active form.
2. Vitamin D needed to absorb calcium (mainly intestinal dietary calcium).
3. Calcium subsequently falls.
4. Parathyroid hormone (PTH) increases to compensate by increasing bone resorption of calcium.
5. Without treatment calcium levels stay low. Increasing PTH causes further excessive bone demineralisation.
6. As kidney function falls, the excretion of phosphate (aided by PTH) becomes inadequate.
7. This further increases PTH (with no effect on phosphate excretion due to the kidney’s poor function), thereby increasing bone demineralisation.
8. Treatment: phosphate restriction by diet and binding with calcium carbonate; increase calcium by giving vitamin D supplements.
Renal transplants
Renal transplants may be from live donors or cadaveric. They are usually located in the pelvis with the native kidneys left in. Occasionally the native kidneys are removed prior to transplantation, so remember to look at the sides and back for scars too. You may sometimes see a scar or plaster from a renal biopsy to give you a clue.
COMMENTS ON STATION 3
DIAGNOSIS: PREVIOUS MASTOIDECTOMY
Although we rarely use tuning forks in clinical practice it is one of those things that occasionally comes up in the exam and can flummox candidates if you don’t refresh your memory. Tuning fork tests are based on the principle that sound should travel better through air than through bone in the absence of hearing impairment. Weber’s test is performed by placing a vibrating 512 Hz tuning fork on the vertex of the skull. If the patient, when asked, can hear the sound louder on one side compared to the other then this is abnormal. The side the sound is localised to indicates conductive hearing loss on that side or sensory hearing loss on the contralateral side. Rinne’s test involves placing a vibrating fork next to the pinna (testing air conduction) and then behind the pinna on the mastoid process (testing bone conduction). If the sound is heard better through air than through bone then it is said to be Rinne’s positive and vice versa. Rinne’s test is positive in sensorineural hearing loss or normal hearing and negative in conductive hearing loss.
COMMENTS ON STATION 4
DIAGNOSIS: ATOPIC ECZEMA
‘Anthony is a well-grown 6-year-old with eczema. Eczema is associated with other atopic conditions such as asthma and hay fever. He has no wheeze or signs of chronic respiratory distress on examination at present. However, it would be important to take a good history from Anthony and his parents to ensure he has no interval symptoms.’
| Diagnosis | May present in infancy onwards |
| Family or personal history of atopy | |
| Management: non-medical | Switch to a non-biological washing powder |
| Trim fi ngernails | |
| Use mittens in the persistent child | |
| Management: medical | Emollient: Apply generously. Examples include 50:50 paraffin. |
| Avoid soap and use bath oils such as Oilatum. Some bath oils include antiseptic, such as Emulsiderm | |
| Steroid cream: Use sparingly on troublesome areas. Be wary of using too high a strength. 0.5–1% hydrocortisone on the face or on babies. | |
| Stronger steroid creams include: |
COMMENTS ON STATION 5
DIAGNOSIS: WILLIAMS’ SYNDROME
This question is another example of the need to be versatile. You may be asked to perform small, separate tasks. In this question it is important to be able to interact well with a child and think on your feet. Don’t be thrown by simple questions such as ‘Look at this. What do you think?’ – a difficult skill to revise for but may be practised by asking friends to pretend to be syndromes and feed you snippets of their features until you recognise them. You may not be able to spot the particular feature in the exam but you will start to learn certain patterns of abnormality.
Does Nicola attend a mainstream school?
Does Nicola have a statement of special educational needs/special educational needs coordinator?
Is Nicola under the care of a community paediatrician? Did Nicola spend time in SCBU/NICU?
(Tuberous sclerosis and neurofibromatosis do not have cardiac defects as part of their clinical and associated features.)
The other clue we have above is her very happy, chatty demeanour.
With this in mind you could ask mum and the examiner some clever questions to show that you know what you’re talking about.
Did Nicola have problems with high calcium levels as a baby?
Did she have an operation due to supravalvular aortic stenosis?
Or if you’re feeling really clever: has she had FISH studies to show she has a problem with chromosome 7?
REMINDER
| Facial | Systemic | Clinical |
|---|---|---|
| Prominent lips | Hypoplastic nails | Transient neonatal hypercalcaemia |
| Blue eyes | Supravalvular aorticstenosis | Mild IUGR |
| Microdontia | Pulmonary artery stenosis | Mild microcephaly |
| Snub nose | Renal artery stenosis | Mild learning difficulties |
| Medial eyebrow flare | ||
| Stellate pattern to iris | ||
| Short palpebral fissures |
COMMENTS ON STATION 6
DIAGNOSIS: ISOLATED SPEECH DELAY/SPEECH DIFFICULTY
Although the station implied delayed speech and language, the question demanded a complete developmental age assessment. Without doing any formal assessment the above has already given you a good framework in which to calculate any potential delays. In this brief segment you see a child who is probably 18–24 months with a potential speech and hearing delay.
When listening to speech it is important to appreciate the difference between:
• Developmental problems: this encompasses a delay due to familial, environmental or central causes.
CAN YOU …
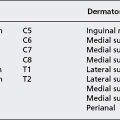
Examine the ninth, tenth, eleventh and twelfth cranial nerves?
(Look away now and talk through your examination with a colleague or in the mirror. Don’t cheat!)
• Ninth: glossopharyngeal nerve
COMMENTS ON STATION 7
Are any other health professionals (health visitor, for instance) involved in her care?
You are: The mother of one child, Laura, who was diagnosed with asthma a year ago.
Background information: You are a busy single working mother who is struggling with working and raising a child at the same time. Laura is repeatedly unwell and has required multiple hospital admissions. On each occasion you have found the doctors too busy to take a little extra time to explain Laura’s treatment plan with you. You did not want to impose on them and were grateful to leave the hospital quickly so you could get back to work. The inhalers you have been given seem still to be working, so you have never felt the need to pick up further prescriptions.
• You have been increasingly worried about Laura’s health recently and feel maybe it is time to get to grips with the situation. You would also like to stop smoking but don’t know how to get the support.
• How do I get advice on the correct way to give Laura her medication?
• Don’t steroids impair growth?
• It’s very difficult to stop smoking. Is there anyone who can help?
Compare the above story with the following:
• If she will get better anyway why do I have to give her the steroids? They are bad, aren’t they?
• I don’t smoke in the same room as the children, so why should I give up?
• It’s difficult to organise trips to the GP/hospital so I don’t want to come to any follow-up.
REMINDER
You may remember the term ‘non-lexical utterances’ from communication skills at medical school. These are small noises or prompts, which are not true words, that act as an encouragement to the person you are speaking to. They are often associated with nodding motions of the head or arm gestures. Examples include ‘Mmmmm’, ‘Ahhhh’, ‘Uh-huh’. Some candidates will use them almost subconsciously.
COMMENTS ON STATION 8
1. Introduce yourself. Ask the student’s name and understanding of the topic.
2. Explain the objectives of the session:
 Practical demonstration.
Practical demonstration.3. Neonatal hip examination is a screening procedure carried out on every child born in the UK. The screening is for developmental dysplasia of the hip (DDH); avoid the term ‘congenital dislocation’. There is a repeat test by the GP at 6 weeks of age.
4. DDH may present with asymmetrical skin creases or an apparent shortening of the femur (Galeazzi’s sign). These features are unlikely to present at birth and are more likely to be apparent at the 6-week check.
5. You must inform the parents that you will be opening and closing the hips. This will not hurt the child but they may not like the sensation and so may become upset.
6. Barlow’s test: The child must be lying on their back with the hips flexed at approximately 90° to the abdomen and heels touching the buttocks. Keeping the knee fully flexed, place your thumb on the medial condyle of the femur. Your fingers should be placed on the greater trochanter so that you have complete control of the femur and will not be touching the hip. These landmarks may be difficult to find in the chunky neonate. It is most important that the student is seen to have a good grip on the femur and has their thumb on the medial aspect and fingers on the lateral aspect of the thigh. Pushing down on the hip following a line of force through the femur may demonstrate the ‘clunk’ of hip dislocation – a positive Barlow’s test.
7. Ortolani’s test: This test relocates a dislocated hip. With hands in the same position as in Barlow’s test, you must simultaneously abduct (open out) the hips and provide an anterior force on the femur (i.e., the opposite to Barlow’s test). This may produce the ‘clunk’ of reduction – a positive Ortolani test.
8. In practice, both hips are examined at the same time and both Barlow’s and Ortolani’s tests are performed in one ‘in and out’ motion. For the purposes of student demonstration it may be best to focus on one hip and one procedure.
9. The hip dummy tends to have one hip which obviously comes out of place. If this is the case the student must demonstrate his ability to produce and recognise hip dislocation. You will fail the station if there is the possibility the student may not be able to correctly identify DDH. You will not fail the station if you run out of time.
10. Ask the student to demonstrate their understanding by asking them to roleplay an exam with you as parent of the hip dummy. He must introduce himself, explain the procedure and perform the test. If you have time you can then discuss what he would say to parents if the test is positive.
REMINDER
DDH
Epidemiology
• Check your local policy. Those children with risk factors must have an ultrasound regardless of examination findings, although actual criteria differ between units. Universal ultrasound screening is a controversial area and further studies are ongoing as to its effectiveness.
COMMENTS ON STATION 9
There are many reasons why Tamsin may find it difficult to go back to school.
• She is bullied for being ‘short’.
• She only has one friend due to the time she has missed.
• She needs help with toileting and dressing at school.
• She is unable to take flights of stairs to different lessons.
To enable Tamsin’s return to school many people need to be involved: