126 Chronic lymphocytic leukaemia
Salient features
Examination
• Usually men over the age of 40 years (male : female ratio is 2 : 1)
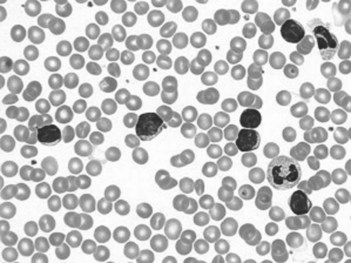
• Tell the examiner that you would like to do a FBC and examine the peripheral smear (lymphocytosis >15 × 109 cells/l, with mature appearance of small lymphocytes) (Fig. 126.1).
Questions
Advanced-level questions
How is chronic lymphocytic leukaemia staged?
A: no anaemia or thrombocytopenia and less than three areas of lymphoid enlargement
B: no anaemia or thrombocytopenia, with three or more involved areas
C: anaemia and/or thrombocytopenia, regardless of the number of areas of lymphoid enlargement.
How are patients with chronic lymphocytic leukaemia treated?
• Stage A. Specific treatment may not be indicated until stage B or C. Patients with stage A disease should be reassured that, despite the frightening diagnosis of leukaemia, they will be able to live a normal life for many years, with a median survival of 8 years (N Engl J Med 1998;338:1506–14).
• Stage B and C. Patients will require specific and supportive therapy: correction of anaemia and folic acid deficiency, and correction of bone marrow infiltration initially with prednisolone and oxymetholone and subsequently with chemotherapeutic agents. The initial treatment of choice is the combination of the chemotherapeutic agent fludarabine plus the antibody rituximab, with or without the addition of the chemotherapeutic drug cyclophosphamide. Fludarabine is first choice for elderly patients, for whom frequent trips to the clinician’s office is difficult. The monoclonal antibody alemtuzumab has been approved for treatment of refractory chronic lymphocytic leukaemia, and lenalidomide has also been shown to have effectiveness in refractory disease. The role of lenalidomide in primary therapy is being studied. The investigational agent flavopiridol has shown encouraging results in certain types of chronic lymphocytic leukaemia (such as those with deletions of 17p) that have not responded to other therapy.






