[level-membership-for-emergency-medicine-category]
CHEST PAIN
Chest pain may be a manifestation of a variety of disorders, ranging from a harmless chest cold or heartburn to a life-threatening heart attack. To try to attain a diagnosis, it is important to ask these questions:
2. What is the nature of the pain?
4. How long have you had the pain?
5. Does the pain extend into the arm, neck, jaw, or abdomen?
ANGINA PECTORIS
Angina pectoris (“angina”) is caused by narrowing or obstruction (spasm or actual occlusion) of the coronary arteries, which supply the heart muscle. The pain, which lasts from 3 to 15 minutes, is most often described as heavy and pressure-like (“squeezing,” like a weight on the chest); it is classically located beneath the breastbone (but may also commonly be present in the left front chest), with occasional radiation to the jaw, back (between the shoulder blades), and left arm. Rarely, it can radiate to the right arm. Associated symptoms include nausea, sweating, shortness of breath, anxiety, and weakness. It is commonly associated with exertion, emotional stress, or both, and may be more frequent at high altitudes (this is debated by doctors), where less oxygen is available. Symptoms are sometimes worse in cold weather or after meals. “Atypical” angina is pain that occurs at rest or that awakens a victim from sleep. Women more commonly have nonclassic symptoms of angina than do men. These include irregular heartbeat, “sharp” or “stabbing” pain, pain that can be reproduced by pressing on the chest, and pain that is localized to underneath the breast. Additional symptoms in elders include shortness of breath with exercise, weakness, or sweating. A first-time angina episode, change in the pattern of existing angina episodes, or increased frequency of episodes may portend a heart attack. Angina may be relieved by rest. Persons with known angina are generally prescribed drugs: nitrates (e.g., isosorbide dinitrate), beta-adrenergic blockers (e.g., metoprolol), or calcium channel blockers (e.g., nifedipine, verapamil, or diltiazem). They also may be taking low-dose aspirin and a “statin” drug to achieve target lipid (e.g., cholesterol) levels. Any person who is taking a nitrate should not be prescribed medication for erectile dysfunction (e.g., silfenadil citrate [Viagra]).
HEART ATTACK (ACUTE MYOCARDIAL INFARCTION)
This is an emergency, because it may rapidly lead to complete cardiac arrest (standstill). A person suffering a heart attack will usually show some or all of the following symptoms: crushing substernal (under the breastbone) chest pain that may extend into the back, left arm or both arms, or neck; shortness of breath; profound weakness; nausea or vomiting; pale, moist, and cool skin; sweating; agitation; abnormal heart rate and rhythm—slow, fast, or irregular; and collapse. Typically, the chest pain does not subside with the administration of nitroglycerin. When cardiac arrest occurs, the victim stops breathing and has no heartbeat. Any elderly person with chest pain requires prompt physician evaluation.
Treatment for a Heart Attack
2. If the victim has a pulse and is breathing, he should be kept at absolute rest and arrangements should be made for immediate transport to a medical facility. Adminster one aspirin tablet (325 mg) by mouth. If oxygen is available, it should be administered by face mask at a flow rate of 5 to 10 liters per minute.
3. If the victim collapses, assess the need for cardiopulmonary resuscitation (CPR) by feeling for a pulse (see page 33) and checking for breathing (see page 12). If these are absent, begin CPR (see page 32).
RAPID HEART RATE
Supraventricular tachycardia (SVT), sometimes called paroxysmal atrial tachycardia (PAT), is a disorder that causes a person’s heart to beat very rapidly, sometimes up to 250 beats per minute. This can make the victim extremely uncomfortable, with a sensation of pounding or fluttering in the chest, palpitations, chest discomfort or tightness, anxiety, light-headedness, shortness of breath, nausea, or weakness. If he is not carrying appropriate medications to treat this syndrome, you might try having the victim bear down and hold his breath as if straining to lift a heavy weight, or immerse his face in a pool of ice water. Another technique is to have him close his eyes, then have him press firmly on both eyeballs for 15 seconds to the point of moderate discomfort. Do not suggest this if the victim has glaucoma or recent eye surgery. Rubbing and pressing (“massaging”) one of the carotid arteries (see page 133) in the victim’s neck can sometimes send a reflex signal through the nervous system to the heart to cause it to slow to a normal rate (“break” the SVT). Carotid artery massage must be done in elders with extreme caution, because on rare occasion it has been noted to precipitate a stroke (see page 144). SVT is definitively treated by a physician with an intravenous injection of a specific medication (often adenosine), or in a dire emergency with a controlled (synchronized) electrical shock to the heart. Persons may carry medications to control or treat SVT. These include diltiazem (or another calcium channel blocker), metoprolol (or another beta blocker), and many others.
NONCARDIAC CAUSES OF CHEST PAIN
Heartburn
The pain of gastrointestinal upset (in particular, reflux of food and acid from the stomach into the esophagus) may closely mimic angina. Typically, heartburn (reflux esophagitis, or “reflux”) occurs after a large meal, especially when the victim immediately lies down. Foods that are often troublesome include alcoholic and carbonated beverages, coffee, chocolate, and fats. The discomfort radiates sharply from the stomach through the breastbone and into the throat. Pain, belching, and a sour taste in the mouth may indicate a hiatal hernia, which allows reflux of stomach acid back up into the esophagus. Treatment for heartburn is discussed on page 221. If there is any suggestion that angina (see page 49) is present, seek medical attention. Because the symptoms of a heart attack can be easily confused with those of heartburn, any elderly person with chest or abdominal pain requires prompt physician evaluation.
Muscle Injuries
Heavy physical exertion can lead to overuse syndromes. The pain is related to muscle motion and is accompanied by pain with motion and soreness to the touch. Treatment for these injuries is discussed on page 284.
Costochondritis
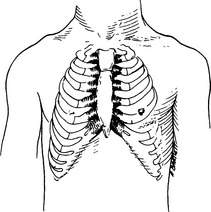
Costochondritis is an irritation of the cartilaginous ends of the ribs where they attach to the sternum (Figure 30). The pain is sharp and well localized to the breastbone and adjacent rib ends. It is worsened considerably by pressing on the area or by deep breathing. Occasionally, slight painful swellings of the rib ends can be felt. The treatment is administration of aspirin or a nonsteroidal anti-inflammatory drug (such as ibuprofen).
[/level-membership-for-emergency-medicine-category][not-level-membership-for-emergency-medicine-category]
CHEST PAIN
Chest pain may be a manifestation of a variety of disorders, ranging from a harmless chest cold or heartburn to a life-threatening heart attack. To try to attain a diagnosis, it is important to ask these questions:
2. What is the nature of the pain?
4. How long have you had the pain?
5. Does the pain extend into the arm, neck, jaw, or abdomen?
ANGINA PECTORIS
Angina pectoris (“angina”) is caused by narrowing or obstruction (spasm or actual occlusion) of the coronary arteries, which supply the heart muscle. The pain, which lasts from 3 to 15 minutes, is most often described as heavy and pressure-like (“squeezing,” like a weight on the chest); it is classically located beneath the breastbone (but may also commonly be present in the left front chest), with occasional radiation to the jaw, back (between the shoulder blades), and left arm. Rarely, it can radiate to the right arm. Associated symptoms include nausea, sweating, shortness of breath, anxiety, and weakness. It is commonly associated with exertion, emotional stress, or both, and may be more frequent at high altitudes (this is debated by doctors), where less oxygen is available. Symptoms are sometimes worse in cold weather or after meals. “Atypical” angina is pain that occurs at rest or that awakens a victim from sleep. Women more commonly have nonclassic symptoms of angina than do men. These include irregular heartbeat, “sharp” or “stabbing” pain, pain that can be reproduced by pressing on the chest, and pain that is localized to underneath the breast. Additional symptoms in elders include shortness of breath with exercise, weakness, or sweating. A first-time angina episode, change in the pattern of existing angina episodes, or increased frequency of episodes may portend a heart attack. Angina may be relieved by rest. Persons with known angina are generally prescribed drugs: nitrates (e.g., isosorbide dinitrate), beta-adrenergic blockers (e.g., metoprolol), or calcium channel blockers (e.g., nifedipine, verapamil, or diltiazem). They also may be taking low-dose aspirin and a “statin” drug to achieve target lipid (e.g., cholesterol) levels. Any person who is taking a nitrate should not be prescribed medication for erectile dysfunction (e.g., silfenadil citrate [Viagra]).
[/not-level-membership-for-emergency-medicine-category]
