[level-membership-for-basic-science-category]
Chapter 19 Chest and Abdominal Wall
Thoracic Ventral Spinal Rami
There are 12 pairs of thoracic ventral rami. The upper 11 lie between the ribs (intercostal nerves), and the twelfth lies below the last rib (subcostal nerve) (Figs 19.1, 19.2). Each is connected with the adjoining ganglion of the sympathetic trunk by grey and white rami communicantes; the grey ramus joins the nerve proximal to the point at which the white ramus leaves it. Intercostal nerves are distributed primarily to the thoracic and abdominal walls. The first two nerves supply fibres to the upper limb in addition to their thoracic branches, the next four supply only the thoracic wall and the lower five supply both thoracic and abdominal walls. The subcostal nerve is distributed to the abdominal wall and the gluteal skin. Communicating branches link the intercostal nerves posteriorly in the intercostal spaces, and the lower five nerves communicate freely in the abdominal wall.
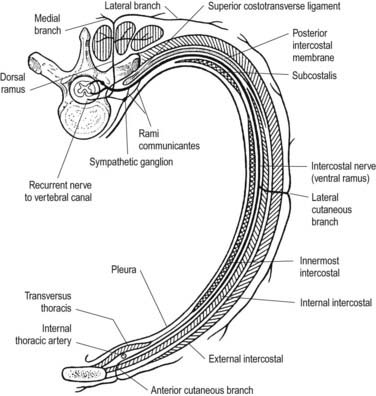
Fig. 19.1 Course of a typical intercostal nerve. The muscular and collateral branches are not shown.
First to Sixth Thoracic Ventral Rami
The second to sixth thoracic ventral rami pass forward in their intercostal spaces below the intercostal vessels. At the back of the chest they lie between the pleura and external intercostal membranes, but in most of their course they run between the internal intercostals and the subcostals and innermost intercostals (see Fig. 19.2). Near the sternum, they cross anterior to the internal thoracic vessels and transversus thoracis; pierce the internal intercostals, external intercostal membranes and pectoralis major; and end as the anterior cutaneous nerves of the thorax, which supply the skin on the front of the thorax. The second anterior cutaneous nerve may be connected to the medial supraclavicular nerves of the cervical plexus; twigs from the sixth intercostal nerve supply abdominal skin in the upper part of the infrasternal angle.
Branches
The lateral cutaneous branch of the second intercostal nerve is the intercostobrachial nerve (see Fig. 18.9). It crosses the axilla to gain the medial side of the arm and joins a branch of the medial cutaneous nerve of the arm. It then pierces the deep fascia of the arm and supplies the skin of the upper half of the posterior and medial parts of the arm, communicating with the posterior cutaneous branch of the radial nerve. Its size is in inverse proportion to the size of the medial cutaneous nerve. A second intercostobrachial nerve often branches off from the anterior part of the third lateral cutaneous nerve and sends filaments to the axilla and the medial side of the arm.
Seventh to Twelfth Thoracic Ventral Rami
The seventh to twelfth lower thoracic ventral rami continue anteriorly from the intercostal spaces into the abdominal wall (Fig. 19.3). Approaching the anterior ends of their respective spaces, the seventh and eighth nerves curve superomedially across the deep surface of the costal cartilages between the digitations of the transverse abdominis. They reach the deep aspect of the posterior layer of the aponeurosis of internal oblique. Both the seventh and eighth nerves then run through this aponeurosis, pass posterior to the rectus abdominis and supply branches to the upper portion of the muscle. They pass through the muscle near its lateral edge and pierce the anterior rectus sheath to supply the skin of the epigastrium.
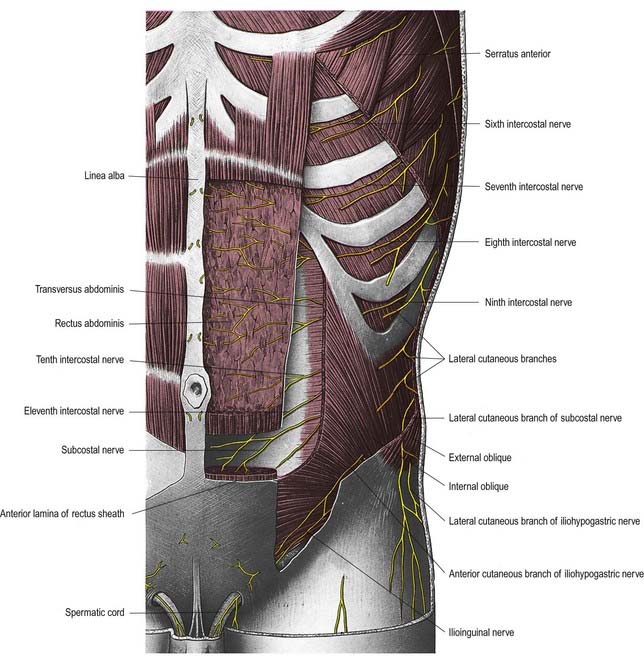
The ninth to eleventh intercostal nerves pass from their intercostal spaces between digitations of the diaphragm and transversus abdominis. They enter the layer between the transversus abdominis and internal oblique. Here, the ninth nerve runs forward almost horizontally, whereas the tenth and eleventh pass inferomedially. At the lateral edge of rectus abdominis, the nerves pierce the posterior layer of the aponeurosis of internal oblique and pass behind the muscle to end, like the seventh and eighth intercostal nerves, with cutaneous branches. The ninth nerve supplies skin above the umbilicus; the tenth supplies skin, which includes the umbilicus; and the eleventh supplies skin below the umbilicus (see Fig. 8.15). The twelfth thoracic nerve (subcostal nerve) connects with the first lumbar ventral ramus (dorsolumbar nerve). It accompanies the subcostal vessels along the inferior border of the twelfth rib, passing behind the lateral arcuate ligament and kidney and anterior to the upper part of the quadratus lumborum. It perforates the transversus abdominis fascia, running deep to the internal oblique, to be distributed like the lower intercostal nerves. It supplies the anterior gluteal skin, reaching down to the greater trochanter.
Twelfth Thoracic Ventral Ramus (Subcostal Nerve)
The ventral ramus of the twelfth thoracic nerve (subcostal nerve) is larger than the others. It gives a communicating branch to the first lumbar ventral ramus (sometimes termed the dorsolumbar nerve). Like the intercostal nerves, it soon gives off a collateral branch. It accompanies the subcostal vessels along the inferior border of the twelfth rib, passing behind the lateral arcuate ligament and kidney and in front of the upper part of quadratus lumborum. It perforates the aponeurosis of the origin of the transversus abdominis and passes forward between that muscle and internal oblique, to be distributed in the same manner as the lower intercostal nerves. It connects with the iliohypogastric nerve of the lumbar plexus and sends a branch to the pyramidalis. The lateral cutaneous branch of the subcostal nerve pierces the internal and external oblique muscles and supplies the lowest slip of the latter. It descends over the iliac crest approximately 5 cm behind the anterior superior iliac spine (see Fig. 19.3) and is distributed to the anterior gluteal skin; some filaments reach as low as the greater trochanter of the femur.
Thoracic Dorsal Spinal Rami
Medial branches of the upper six thoracic dorsal rami pass between and supply the semispinalis thoracis and multifidus; they then pierce the rhomboids and trapezius and reach the skin near the vertebral spines (see Fig. 8.14). Medial branches of the lower six thoracic dorsal rami are distributed mainly to multifidus and longissimus thoracis; occasionally they give filaments to the skin in the median region. Lateral branches increase in size from above downward. They run through or deep to longissimus thoracis to the interval between it and iliocostalis cervicis, supplying these muscles and levatores costarum; the lower five or six also give off cutaneous branches that pierce serratus posterior inferior and latissimus dorsi in line with the costal angles (see Fig. 8.14). The lateral branches of a variable number of upper thoracic rami also supply the skin. The lateral branch of the twelfth sends a filament medially along the iliac crest, then passes down to the skin of the anterior part of the gluteal region.
Lesions of the Intercostal Nerves
CASE 1 Herpes Zoster
Discussion: This woman has typical herpes zoster infection (‘shingles’), a remarkably painful but limited disorder of acute onset. Herpes zoster virus remains dormant in dorsal root ganglia following infection with chickenpox, generally for many years; it may be reactivated in immunocompromised individuals or in the non-immunocompromised elderly. Pain usually precedes the skin lesions and follows a dermatomal distribution in one or several adjacent dermatomes. The appearance of vesicular lesions in the same distribution clearly identifies the cause. The motor nerve and even the spinal cord may be involved, resulting in the appearance of an acute radiculopathy, sometimes leaving the patient with weakness and atrophy in that nerve root distribution. In some patients, severe and incapacitating pain lingers—so-called postherpetic neuralgia.
[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]
Chapter 19 Chest and Abdominal Wall
Thoracic Ventral Spinal Rami
There are 12 pairs of thoracic ventral rami. The upper 11 lie between the ribs (intercostal nerves), and the twelfth lies below the last rib (subcostal nerve) (Figs 19.1, 19.2). Each is connected with the adjoining ganglion of the sympathetic trunk by grey and white rami communicantes; the grey ramus joins the nerve proximal to the point at which the white ramus leaves it. Intercostal nerves are distributed primarily to the thoracic and abdominal walls. The first two nerves supply fibres to the upper limb in addition to their thoracic branches, the next four supply only the thoracic wall and the lower five supply both thoracic and abdominal walls. The subcostal nerve is distributed to the abdominal wall and the gluteal skin. Communicating branches link the intercostal nerves posteriorly in the intercostal spaces, and the lower five nerves communicate freely in the abdominal wall.
Fig. 19.1 Course of a typical intercostal nerve. The muscular and collateral branches are not shown.
First to Sixth Thoracic Ventral Rami
The second to sixth thoracic ventral rami pass forward in their intercostal spaces below the intercostal vessels. At the back of the chest they lie between the pleura and external intercostal membranes, but in most of their course they run between the internal intercostals and the subcostals and innermost intercostals (see Fig. 19.2). Near the sternum, they cross anterior to the internal thoracic vessels and transversus thoracis; pierce the internal intercostals, external intercostal membranes and pectoralis major; and end as the anterior cutaneous nerves of the thorax, which supply the skin on the front of the thorax. The second anterior cutaneous nerve may be connected to the medial supraclavicular nerves of the cervical plexus; twigs from the sixth intercostal nerve supply abdominal skin in the upper part of the infrasternal angle.
