CHEST AND ABDOMEN
CHEST AND ABDOMEN
Interrogations in relation to diagnoses of the chest and abdomen are discussed separately below.
CHEST
The chest, or thorax, refers to the part of the body enclosed by the ribs and breast bone. From the Chinese point of view, there is a difference between the front part of the chest, which is under the influence of the Heart and Lungs, and the sides of the chest, which are under the influence of the Liver and Gall-Bladder. The front of the chest is also the area where the Gathering Qi (Zong Qi) is concentrated (see Fig 12.1, p. 121).
WHY WE ASK
In addition, both the tongue and the pulse frequently reflect a pathology of the chest: a Purple area in the tongue’s chest area (see Fig 23.10 on p. 206), for example, or a pulse that is Weak and Deep on both Front positions.
WHEN WE ASK
Chest symptoms often reflect very common pathologies such as Liver-Qi stagnation, Phlegm in the chest and Heart-Blood deficiency. Therefore, I specifically ask about chest symptoms quite early in the interrogation as patients are describing their symptoms.
HOW WE ASK
Cough
Observation, Chapter 20; Hearing, Chapter 53; Symptoms and Signs, Chapter 63
Case history 38.1 illustrates a pattern underlying chronic cough.
Box 38.1 summarizes the patterns underlying cough.
Chest pain
Observation, Chapter 16; Symptoms and Signs, Chapter 63
Chest pain accompanied by cough with expectoration of profuse yellow sputum is due to Phlegm-Heat in the Lungs and this may be seen in acute lung conditions, such as bronchitis, pneumonia or pleuritis.
Chest pain extending to the upper back is usually due to Phlegm or Blood stasis.
Box 38.2 summarizes the patterns underlying chest pain.
Pain in the ribs
Symptoms and Signs, Chapter 63
The most common patterns causing pain in the ribs are Liver-Qi stagnation, Blood stasis and Damp-Heat in the Gall-Bladder. The characteristic symptoms of these patterns are listed in Box 38.3.
Feeling of oppression of the chest
Symptoms and Signs, Chapter 63
Box 38.4 summarizes the patterns underlying a feeling of oppression of the chest.
Feeling of heat in the chest
Symptoms and Signs, Chapter 63
Box 38.5 summarizes the patterns underlying a feeling of heat in the chest.
ABDOMEN
Abdomen here refers to the area of the trunk between the diaphragm and the symphysis pubis (see Fig 16.7, p. 145).
HOW WE ASK
After this, the various abdominal symptoms will be discussed according to areas (see Fig 16.7 on p. 145), which are:
Sensations
Distension
Observation, Chapter 16; Symptoms and Signs, Chapter 71
A feeling of abdominal distension or ‘bloating’ is an extremely common symptom. The following patterns most commonly cause distension of the abdomen (in order of frequency):
Pain
Symptoms and Signs, Chapter 71
Among the Empty conditions are:
(For a detailed discussion of the patterns causing abdominal pain in its various areas, see Part 5, Chapter 71.)
Areas of abdominal pain
The regions of the abdomen in Chinese medicine are as follows (see Fig 16.7 on p. 145):
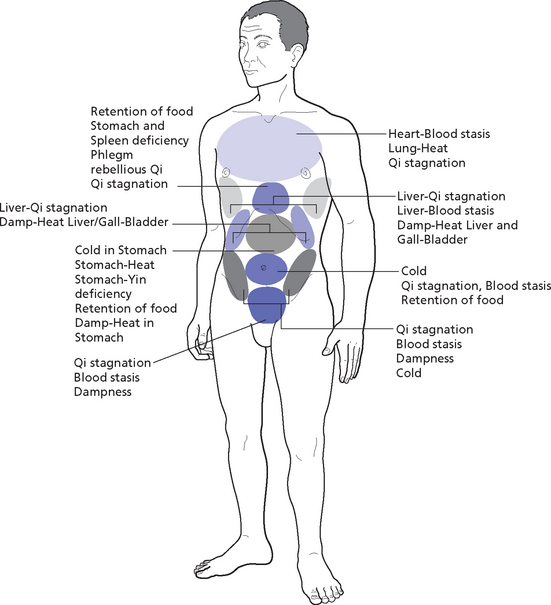
Here I will discuss the most common patterns and conditions differentiated according to their location (i.e. the area under the xyphoid process, epigastrium, hypochondrium, umbilical area, central-lower abdomen, right-lateral lower abdomen and left-lateral lower abdomen). (For the differentiation of various abdominal symptoms, see Part 5, Chapter 71.)
Area under the xyphoid process
Symptoms and Signs, Chapter 71
A feeling of oppression in the area under the xyphoid process usually indicates Phlegm or severe stagnation of Qi in the Heart and Stomach channel. A feeling of fullness in this area indicates retention of food in the Stomach affecting the Heart; a feeling of stuffiness in this area (i.e. the patient feels full but the area is soft on palpation) indicates Stomach and Spleen deficiency with Heart-Heat. A feeling of distension in this area indicates stagnation of Qi in the Stomach.
Box 38.6 summarizes patterns underlying pain in the area under the xyphoid process.
Epigastrium
Symptoms and Signs, Chapter 71
There are many types of epigastric pain, as follows:
Epigastrium manifestation on the tongue
On the tongue, the epigastric area is reflected either in the centre or on the sides around the centre (see Fig 23.3 on p. 205). An examination of the coating in this area is essential to distinguish Full from Empty conditions as a Full condition will be reflected by a thick coating in this area and an Empty condition by a rootless coating or the absence of coating. The coating in this area also closely reflects the Hot or Cold nature of Stomach problems: a white coating indicates Cold while a yellow (including brown) coating indicates Heat. The thickness of the coating reflects the intensity of the pathogenic factor: the thicker the coating, the more intense is the pathogenic factor.
Hypochondrium
Symptoms and Signs, Chapter 71
Case history 38.4 illustrates a pattern underlying hypochondrial pain.
Box 38.8 summarizes the patterns underlying hypochondrial pain.
Central-lower abdominal area
Symptoms and Signs, Chapter 71
The most common patterns causing problems in this area are:
Case history 38.5 illustrates a pattern of Blood stasis and Deficiency causing central-lower abdominal pain.
Box 38.9 summarizes the patterns underlying pain in this area.
Right-lateral lower abdominal area
Symptoms and Signs, Chapter 71
This area is influenced primarily by the Large Intestine and Liver channels and by the Penetrating Vessel. As a rule of thumb, problems in this area are caused by the gynaecological system more often than by the Large Intestine. For example, in women, pain in this area is very often due to ovarian cysts.