Chest
Normal anatomy
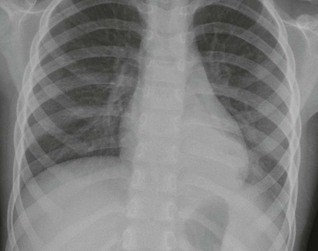
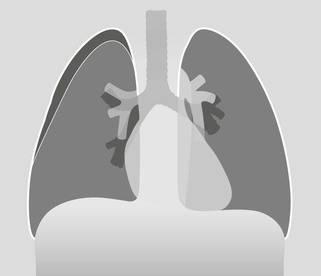
Frontal CXR—the lungs
Frontal CXR—lung markings
Normal lung markings are solely due to vessels and to nothing else. The normal bronchial walls, normal interstitium, and normal lymphatics are not visible.
There is a complete absence of any lung markings in the lung immediately adjacent to each costophrenic angle.
In this peripheral part of the lung the normal vessels are simply too small to be visualised.
If this area shows detectable markings, then interstitial disease, or oedema, is likely1.
Frontal CXR—hila
The hilum is the site at which the bronchi and vessels enter or leave the lung.
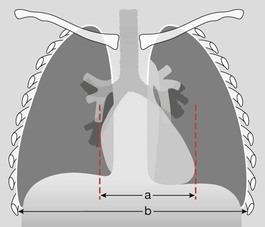
Frontal CXR—cardiothoracic ratio
Most normal hearts have a cardiothoracic ratio (CTR) of less than 50% when assessed on a PA chest radiograph obtained in full inspiration2.
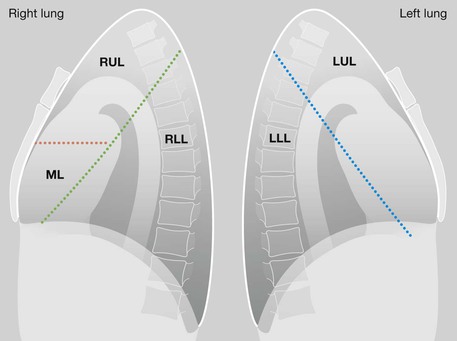
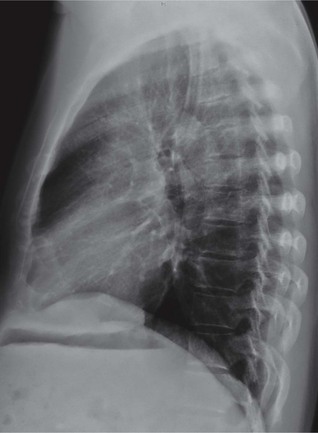
Lateral CXR—the lobes of the lung
The two fissures in the right lung divide the lung into three lobes.
The single fissure in the left lung divides the lung into two lobes.
The oblique fissure on each side is propeller shaped and consequently we only, and very occasionally, see a part of a fissure on a normal lateral CXR.
On the other hand, we will see most of the horizontal fissure on the lateral CXR because it is straight. We will often see this fissure on the frontal CXR for the same reason.
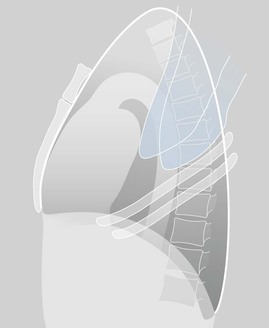
Lateral CXR—three normal appearances

Analysis: the checklists
The frontal CXR
Four steps underpin accurate analysis.
4. Now you can assess the radiograph in an organised and systematic manner. As follows:
□ Is the heart enlarged?
In an adult, the cardiothoracic ratio (CTR) should be < 50% on a PA CXR (see p. 309).
□ Are both domes of the diaphragm clearly seen and well defined?
If part of a dome is obscured, suspect pathology in the adjacent lower lobe.
□ Are both heart borders clearly seen and well defined?
If not, there is a high probability of pathology in the immediately adjacent lung.
□ Are the hila normal … position, size, density?
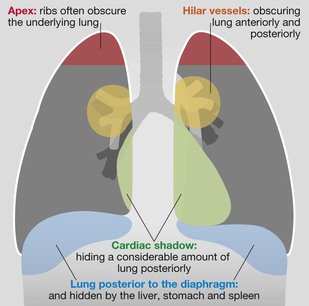
□ Check the tricky hidden areas of the lung: both apices, behind the heart shadow, around each hilum, below the diaphragm (see p. 308).
□ Finally, ask yourself once again:
Have I addressed this patient’s particular clinical problem?


The lateral CXR
Four questions underpin accurate analysis:
1. Are the vertebral bodies becoming blacker from above downwards?
If not (ie they are becoming whiter or greyer) then suspect disease in a lower lobe or in a pleural space.
3. Is there any abrupt change in density across the heart shadow?
“An abrupt change in density” is likely to be a lung abnormality.
4. Have I correlated my findings on the lateral CXR with the frontal CXR appearances?
Ten clinical problems
The full breadth of the radiology of thoracic disease as revealed by the plain CXR is addressed in our companion book The CXR: A Survival Guide1. We cannot cover that detail in this single chapter.
Instead, we will consider the ten clinical problems that account for well over 90% of all CXR requests made in the Emergency Department. We will take each problem in turn and pose a clinical question of the frontal CXR.
Question 1: Is there pneumonia (consolidation)?
Physical examination is not always sufficiently accurate on its own to confirm or exclude the diagnosis of pneumonia3. Many pneumonias will be obvious on the frontal CXR. Some are much more difficult to detect—the hidden pneumonias.
Detecting a hidden pneumonia
▪ Search for any evidence of a silhouette sign1,2,4 on the CXR.
▪ Assess the mediastinal and diaphragmatic boundaries/borders.
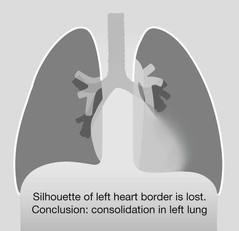
The silhouette sign. An intrathoracic lesion or density touching a border of the heart, aorta, or diaphragm will obliterate part of the border on the CXR1,2.
Explanation: the borders of the heart and both domes of the diaphragm are visible on a normal CXR because the air in the lung contrasts with the water density of the heart and diaphragm. If lung air is replaced by pus (pneumonia) the immediately adjacent border will disappear or be ill-defined. This obliteration is termed the silhouette sign.
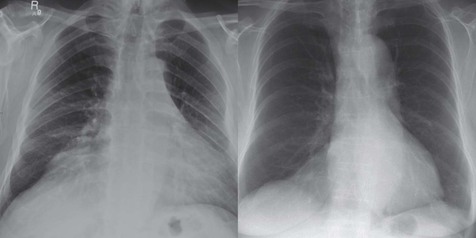
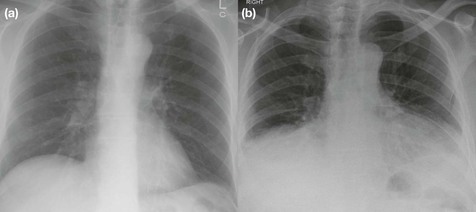
Silhouette sign—Pitfall. Mediastinal fat1.
Some middle aged people accumulate a large collection of fat adjacent to the heart causing the heart border to be ill defined. The fat is of lower density than the water density of lung consolidation and this difference will help you to avoid this pitfall. The patient on the left has lost the sharp silhouette of both the right heart border and of the right dome of the diaphragm. The patient on the right has lost the silhouette of part of the right dome of the diaphragm. In both cases the cause is a large collection of fat.
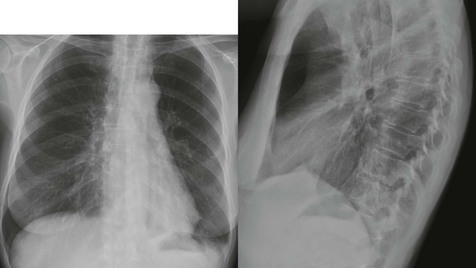
Silhouette sign—Pitfall. Depressed sternum.
The right heart border is effaced, and there is added density suggesting middle lobe consolidation. The lateral CXR shows the depressed sternum which is the cause of the grossly abnormal appearance on the frontal CXR1. The lungs are clear.
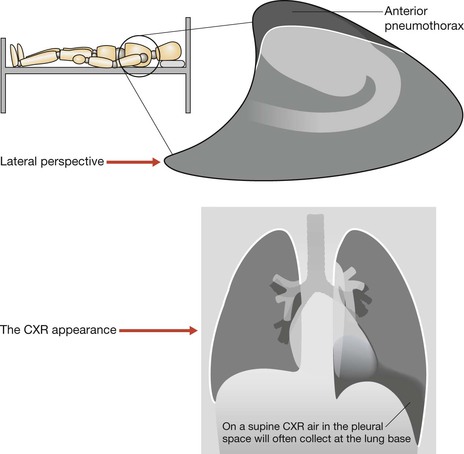
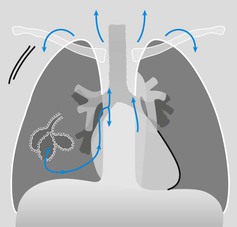
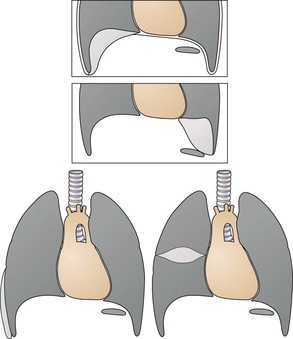
Question 2: Is there a pneumothorax?
An erect CXR obtained in full expiration is recommended. The normal lungs are more opaque (or slightly whiter) on an expiration CXR. Consequently, when a pneumothorax is present the air (black) in the pleural space contrasts with the adjacent (whiter) lung. This accentuation of the difference in contrast, as compared with an inspiration film, sometimes makes it slightly easier to detect a pneumothorax.
Supine CXR. In a severely injured patient the CXR will inevitably be obtained with the patient supine. On a supine CXR the pleural air will rise to the highest point in the pleural space—ie to the anterior aspect of the thorax. Consequently the lung base and the area around the heart need careful evaluation4.
Question 3: Are there signs of left ventricular failure (LVF)?
Look for cardiac enlargement and for lung and pleural changes.

Cardiac enlargement.
Almost all patients with LVF have an enlarged heart. The occasional exception is a patient with an acute myocardial infarction.
Most enlarged hearts have a cardiothoracic ratio (CTR) over 50% when assessed on a PA CXR (p. 309).
The CTR is well over 50% in this patient.
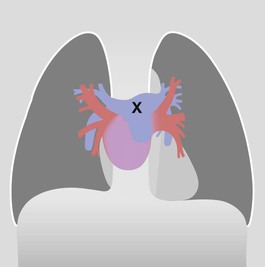
LVF; heart, lung and pleural changes. Erect PA, CXR
| Early | Enlarged heart |
| Oedema: poorly defined (slightly blurred) margins of the hilar vessels | |
| Oedema: septal lines (Kerley B lines) | |
| Small pleural effusions, usually bilateral | |
| Later | Interstitial shadowing, |
| and/or alveolar shadowing (florid oedema), | |
| and/or larger pleural effusions, usually bilateral. |

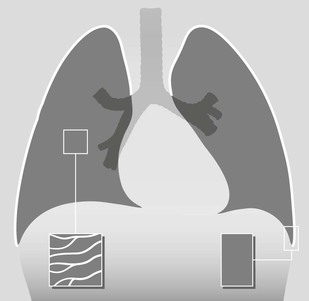
Early LVF. Septal lines (Kerley B lines) caused by fluid in the interstitium. These short, straight lines reach the pleural surface and have this characteristic appearance at the lung base.
Early LVF. Small pleural effusions. Slight blunting of the costophrenic angles. Effusions in LVF are usually bilateral.



Question 4: Severe asthmatic attack—is there a complication?
The complications to look for are lung consolidation, lobar collapse, pneumothorax and pneumomediastinum.


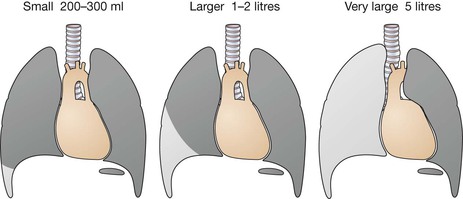
Question 5: Is there a pleural effusion?
Fluid in the pleural space can adopt several different appearances.
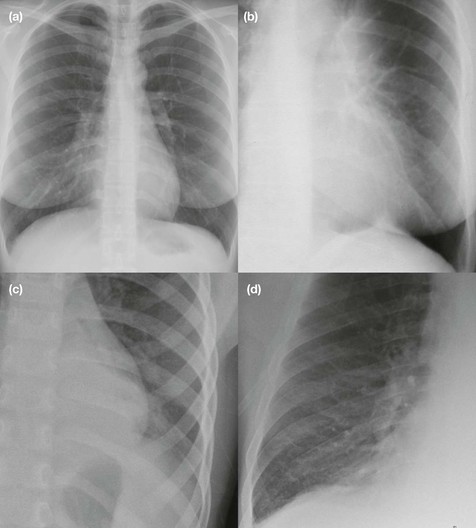
On the erect frontal CXR1
Other patterns also occur:
Bottom left: A linear (lamellar) effusion.
Bottom right: Fluid loculated in the pleural space. In this example—within the horizontal fissure.


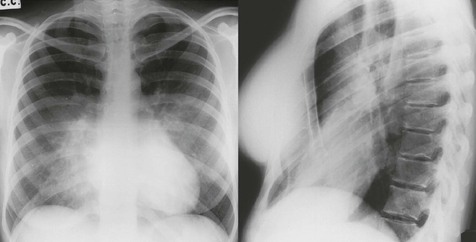
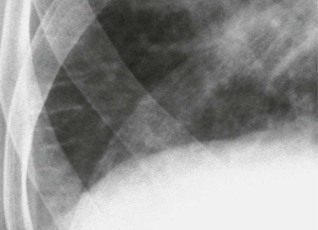
On the supine CXR1
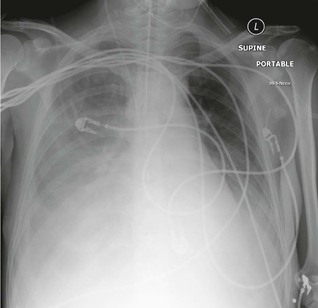
Pleural fluid on a supine CXR1.
The fluid spreads to the most dependent site (ie to the posterior aspect of the pleural space). This causes the right hemithorax to appear greyer/whiter than the opposite side.
In this patient almost all of the shadowing over the right hemithorax is due to a large pleural effusion.
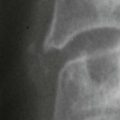
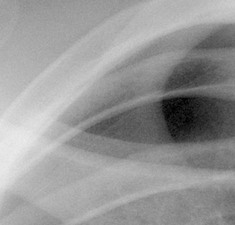
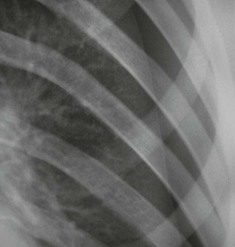
Question 7: Is there a rib fracture?
Oblique views of the ribs are not indicated following a relatively minor injury to the thorax. Clinical management is rarely altered by demonstration of a simple rib fracture. A frontal CXR is obtained solely to exclude an important complication such as a pneumothorax.
Question 9: Is there evidence of a pulmonary embolus?1,4
90% of emboli occur without pulmonary infarction and the CXR often appears normal.
Sometimes non-specific CXR findings are present, including: small areas of linear collapse; a small pleural effusion; slight elevation of a dome of the diaphragm.
Whenever a pulmonary embolus remains a clinical possibility then—whatever the CXR findings—the patient requires definitive imaging, usually a CT pulmonary angiogram.
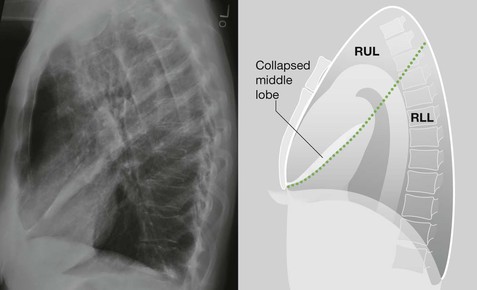
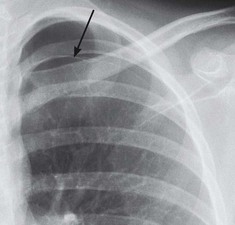
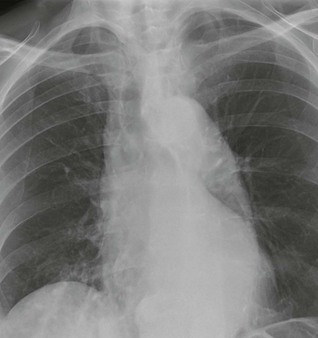
Question 10: Is there evidence of an inhaled foreign body?

This patient had inhaled a peanut and attended the Emergency Department. This CXR is abnormal. It shows evidence of an obstructed bronchus. An additional CXR was obtained, following a particular manouvre, and that CXR provided confirmation of the obstruction. The peanut was removed.
The CXR analysis is provided on p. 30.