[level-membership-for-dermatology-category]
10 Chemical Reconstruction of Skin Scars (CROSS) Technique
Introduction
The chemical reconstruction of skin scars (CROSS) method is a technique for the treatment of atrophic scars and enlarged pores using a sharpened wooden applicator to deeply deliver trichloroacetic acid (TCA) in higher concentration. The CROSS method is used to maximize the effects of TCA and to overcome complications such as scarring and postinflammatory hyper- and hypopigmentation, which are known to develop frequently in dark-skinned patients. The technique was developed to induce neosynthesis of dermal components such as collagen, elastin, and ground substance. This would result in dermal thickening followed by elevation of the depressed scars or narrowing of the enlarged pores. The technique basically consists of firmly pressing down an applicator soaked in TCA on the depressed atrophic acne scars and enlarged pores to produce a confluent frost. However, there are modifications to deliver the TCA in a more controlled manner and to expedite the treatment time (see Box 10.1).
Box 10.1
Key features
Overview of Treatment (Table 10.1)
• Equipment
TCA with various concentrations (% weight/volume, unbuffered) can be purchased (e.g., Sigma-Aldrich, St. Louis, MO) or made by order in a local pharmacy. Clinical efficacy is more pronounced with higher concentrations of TCA. Usually, sharpened wooden applicators are used for CROSS and cotton-tipped wooden applicators are more suitable for the treatment of large and multiple scars (Figure 10.1, Table 10.2).
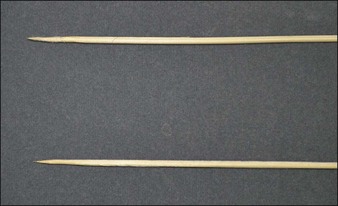
Table 10.1 Summary of expected clinical course in CROSS treatment
| Time required | 5–30 minutes |
| Anesthesia | Not required (topical anesthesia if needed) |
| Pain | Little to moderate prickling and burning sensation |
| Posttreatment daily activity | Crusts usually persist for about one week Posttreatment erythema can persist for one to three months |
| Washing | Possible one day after the treatment |
| Make-up | Possible about seven days after the treatment |

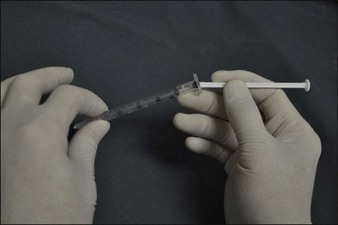
When a large area or numerous enlarged pores have to be treated, multiple repetitive dipping of the wooden applicator in TCA is required which results in the prolongation of the treatment time. Therefore, to shorten the treatment time, we use a method using a 1 mL syringe and a fine-gauge needle as described below. Firstly, a 1 mL syringe is filled with 0.1–0.2 mL of 100% TCA. Secondly, a disposable fine-gauge needle, preferably a 30- or 31-gauge needle for acne scars and a 33-gauge for enlarged pores (Figure 10.2) is inserted. Thirdly, remove the piston gently with caution to prevent spilling of TCA along with the piston (Figure 10.3).

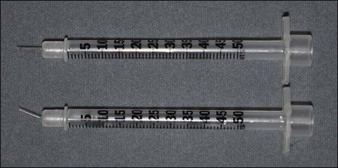
Figure 10.2 A 1 mL syringe is filled with 0.1 mL of 100% TCA and a disposable a 30-gauge needle is used
However, despite its convenience and effectiveness, it is difficult to regulate the flow of TCA from the needle tip compared to a TCA-soaked wooden applicator. To address this problem, the 31-gauge, 8 mm needle on a 1 mL insulin syringe can be gently bent using a mosquito forceps (Figures 10.4–10.6). The flow rate of TCA can be regulated according to the individual needs by the degree of the needle bending and therefore controlling the resistance to the flow.


• Treatment algorithm
Local anesthetics or sedation are not required for the CROSS. Generally, patients feel bearable prickling and burning sensation during the procedure. If needed, a topical anesthetic cream, such as EMLA cream (eutectic mixture of 2.5% lidocaine-HCl and 2.5% prilocaine; AstraZeneca AB, Södertälje, Sweden), can be applied prior to treatment. After facial washing with soap, the skin is cleansed with alcohol. Either 65% or 100% TCA is focally applied on the entire depressed area of atrophic scars or enlarged facial pores with pressure using various applicators (Figures 10.7–10.10). The skin is monitored carefully until it reaches a ‘frosted’ appearance after a single application of TCA, which usually occurs within 10 seconds. The frosted appearance is the result of coagulation of epidermal and dermal proteins and is used mainly to monitor the peel depth. After the procedure, the treated areas are cooled down with ice packs to reduce excessive inflammation and pain.

Figure 10.7 Treatment of chicken pox scars with CROSS method by using a sharpened wooden applicator.

Figure 10.8 Frosted appearance of the lesions on the cheek after CROSS treatment by using a sharpened wooden applicator

Figure 10.9 Treatment of enlarged pores with CROSS method by using a straight needle of an insulin syringe

Case Studies
Lee JB, Chung WG, Kwahck H, Lee KH. Focal treatment of acne scars with trichloroacetic acid: chemical reconstruction of skin scars method. Dermatological Surgery. 2002;28:1017-1021.
McCurdy JAJr, Lam SM. Cosmetic Surgery of the Asian Face 2nd edition. New York: Thieme Medical Publishers; 2005.
Whang SW, Lee KH, Lee JB, Chung KY. Chemical reconstruction of skin scars (CROSS) method using a syringe technique. Dermatological Surgery. 2007;33:1539-1540.
Cho SB, Park CO, Chung WG, et al. Histometric and histochemical analysis of the effect of trichloroacetic acid concentration in the chemical reconstruction of skin scars method. Dermatologic Surgery. 2006;32:1231-1236.
Cho SB, Lee SJ, Kang JM, et al. Chemical reconstruction of skin scars method using a syringe bent-needle technique. Dermatological Surgery. 2009;35:1134-1135.
Kim HJ, Kim TG, Kwon YS, et al. Comparison of a 1,550 nm erbium-glass fractional laser and a chemical reconstruction of skin scars (CROSS) method in the treatment of acne scars: a simultaneous split-face trial. Lasers Surgical Medicine. 2009;41:545-549.
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
10 Chemical Reconstruction of Skin Scars (CROSS) Technique
Introduction
The chemical reconstruction of skin scars (CROSS) method is a technique for the treatment of atrophic scars and enlarged pores using a sharpened wooden applicator to deeply deliver trichloroacetic acid (TCA) in higher concentration. The CROSS method is used to maximize the effects of TCA and to overcome complications such as scarring and postinflammatory hyper- and hypopigmentation, which are known to develop frequently in dark-skinned patients. The technique was developed to induce neosynthesis of dermal components such as collagen, elastin, and ground substance. This would result in dermal thickening followed by elevation of the depressed scars or narrowing of the enlarged pores. The technique basically consists of firmly pressing down an applicator soaked in TCA on the depressed atrophic acne scars and enlarged pores to produce a confluent frost. However, there are modifications to deliver the TCA in a more controlled manner and to expedite the treatment time (see Box 10.1).
Box 10.1
Key features
