[level-membership-for-emergency-medicine-category]
Chapter 68 Chemical and Biological Terrorism
5 What are the four basic phases of disaster response?
Agency for Healthcare Research and Quality: Pediatric Terrorism and Disaster Preparedness: A Resource for Pediatricians: www.ahrq.gov./research/pedprep/resource.htm
7 What are the potential medical consequences of a chemical attack?







10 What clues suggest a biologic attack?
 Epidemic presentation in a relatively compressed time frame (because most persons would be exposed at the same time)
Epidemic presentation in a relatively compressed time frame (because most persons would be exposed at the same time)
 Diseases that are rare or not endemic in the area of exposure
Diseases that are rare or not endemic in the area of exposure
 Especially high infection rate among exposed persons
Especially high infection rate among exposed persons
 More respiratory forms of disease than usual
More respiratory forms of disease than usual
 Particularly high morbidity or mortality
Particularly high morbidity or mortality

 Attack rates lower in persons sheltered from the suspected route of exposure
Attack rates lower in persons sheltered from the suspected route of exposure

 Discovery of suspicious actions or potential delivery systems
Discovery of suspicious actions or potential delivery systems
11 Why may children be disproportionately affected by both chemical and biologic agents?
 Many agents are aerosolized as the intended route of exposure. Children have higher minute ventilation rates and live closer to the ground, which enhances respiratory exposure, especially for agents denser than air.
Many agents are aerosolized as the intended route of exposure. Children have higher minute ventilation rates and live closer to the ground, which enhances respiratory exposure, especially for agents denser than air.







 Pediatric centers probably would be overwhelmed with both indigenous patients and those transferred.
Pediatric centers probably would be overwhelmed with both indigenous patients and those transferred.
KEY POINTS: REASONS THAT CHEMICAL AND BIOLOGIC AGENTS DISPROPORTIONATELY AFFECT CHILDREN
1 They have higher minute ventilation and live closer to the ground, enhancing respiratory exposure of aerosolized agents.
2 They have thinner and more permeable skin, allowing greater injury from vesicant or corrosive chemicals and possibly faster systemic absorption of nerve agents.
3 They have age-related developmental vulnerabilities that may hamper their ability to escape exposure.
4 They may suffer unique psychological trauma after separation from parents or witnessing death of family members.
5 There is limited study of relevant antibiotics, antidotes, and vaccines.
6 EMS systems may be unable to handle pediatric patients.
7 Procedures may be more difficult if providers are garbed in protective gear.
8 Massive numbers of pediatric casualties would overwhelm interhospital transport teams and pediatric treatment centers.
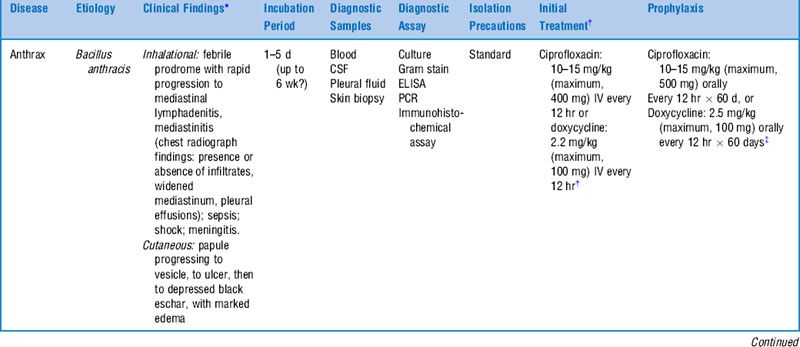
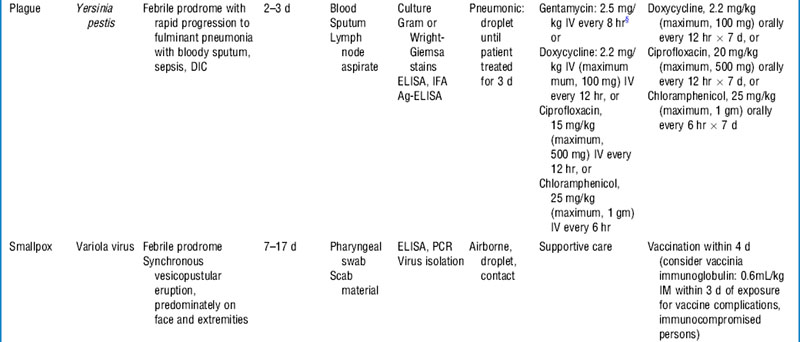
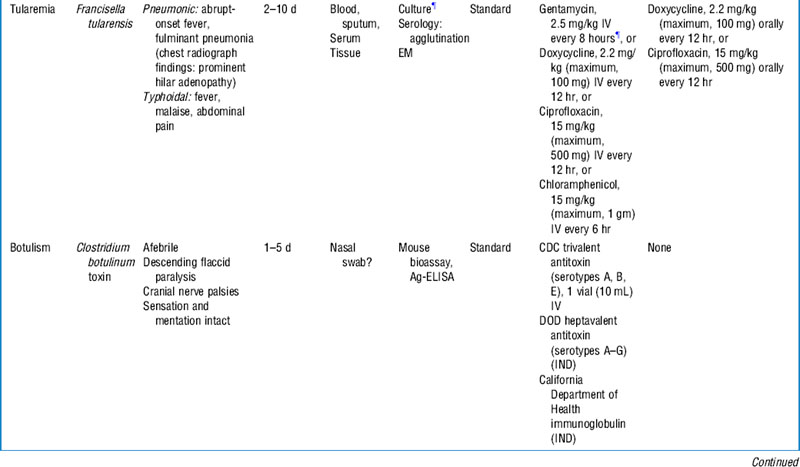
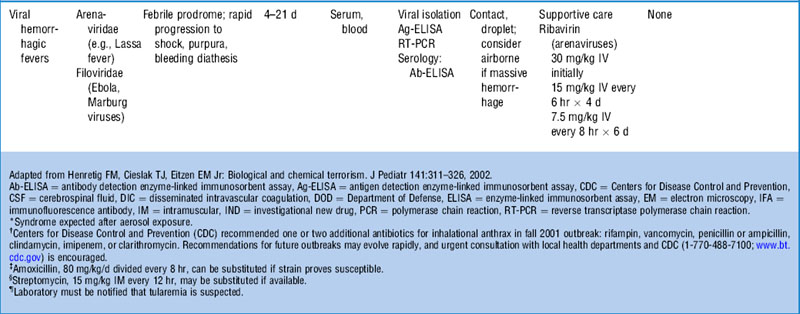
12 What are the principal biologic agent threats?
See Table 68-1. In most circumstances patients will present after a significant time interval from their exposure. In the event of an announced attack, some consideration to decontamination issues is appropriate. In most cases, simple disrobement of outer garments and soap and water washing is sufficient for biologic agents.
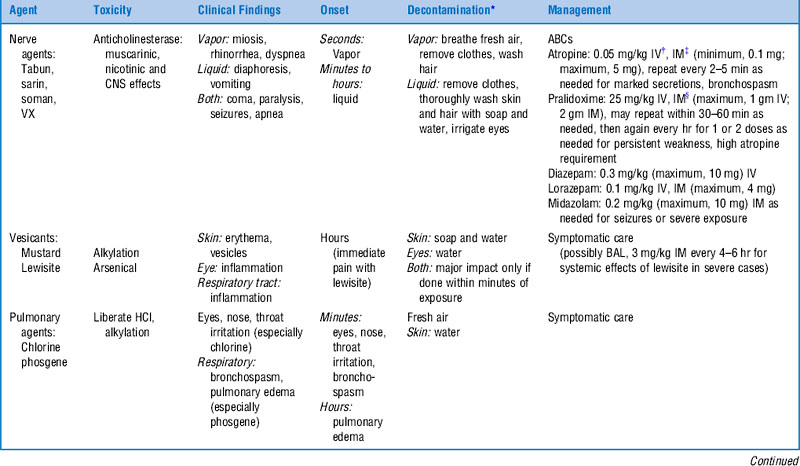
20 Which chemical weapons are most feared?
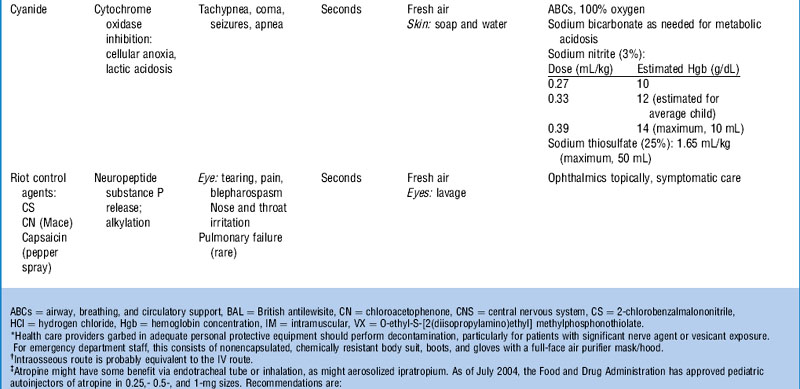
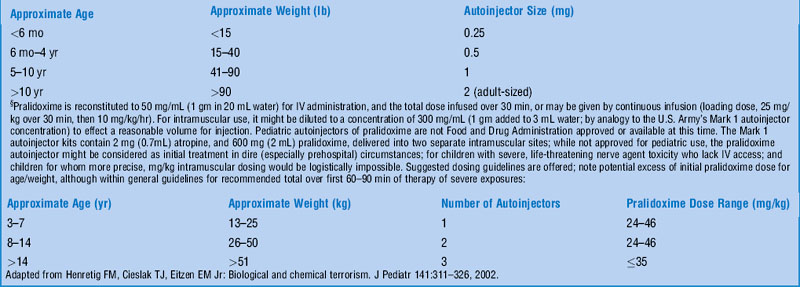
Nerve agents are the most feared chemical weapons. These potent organophosphate compounds, similar to many pesticides, are toxic by inhalation, ingestion, and topical absorption and can result in profound muscarinic (cholinergic syndrome), nicotinic (initial muscle fasciculations, then paralysis), and central nervous system effects (seizures, coma, apnea). The clinical picture varies slightly by route of exposure, as noted in Table 68-2. Severe cases require antidotal therapy with atropine (adults, 2–5 mg; children, 0.02–0.05 mg/kg), pralidoxime (adults, 1–2 gm; children, 25–50 mg/kg), and usually diazepam for seizure control (adults, 5–10 mg; children, 0.1–0.3 mg/kg).
[/level-membership-for-emergency-medicine-category][not-level-membership-for-emergency-medicine-category]
Chapter 68 Chemical and Biological Terrorism
5 What are the four basic phases of disaster response?
Agency for Healthcare Research and Quality: Pediatric Terrorism and Disaster Preparedness: A Resource for Pediatricians: www.ahrq.gov./research/pedprep/resource.htm
