Chapter 239 Cervical Cryocautery
REQUIRED EQUIPMENT
TECHNIQUE
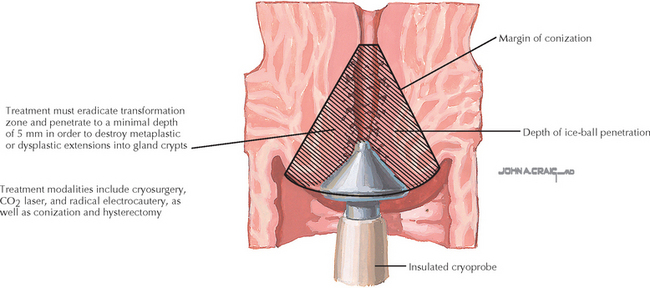
Freezing should continue for 3 minutes, resulting in an ice ball that extends 5 mm beyond the cervical lesion. The freezing mechanism is then deactivated to allow for a 5-minute thaw. The probe should not be actively loosened from the cervix but allowed to defrost and detach by itself. After thawing for 5 minutes, the lesion is refrozen for another 3 minutes. A single 5-minute freeze may also be used, but with either method, the ice ball must extend to a distance of more than 5 mm for the procedure to be effective.
Kwikkel HJ, Helmerhorst TJ, Bezemer PD, et al. Laser or cryotherapy for cervical intraepithelial neoplasia: a randomized study to compare efficacy and side effects. Gynecol Oncol. 1985;22:23.
Mathevet P, Dargent D, Roy M, Beau G. A randomized prospective study comparing three techniques of conization: cold knife, laser, and LEEP. Gynecol Oncol. 1994;54:175.
Mitchell MF, Tortolero-Luna G, Cook E, et al. A randomized clinical trial of cryotherapy, laser vaporization, and loop electrosurgical excision for treatment of squamous intraepithelial lesions of the cervix. Obstet Gynecol. 1998;92:737.
Andersen ES, Thorup K, Larsen G. Results of cryosurgery for cervical intraepithelial neoplasia. Gynecol Oncol. 1988;30:21.
Benedet JL, Miller DM, Nickerson KG, Anderson GH. The results of cryosurgical treatment of cervical intraepithelial neoplasia at one, five, and ten years. Am J Obstet Gynecol. 1987;157:268.
Loobuyck HA, Duncan ID. Destruction of CIN 1 and 2 with the Semm cold coagulator: 13 years’ experience with a see-and-treat policy. Br J Obstet Gynaecol. 1993;100:465.
Ostergard DR. Cryosurgical treatment of cervical intraepithelial neoplasia. Obstet Gynecol. 1980;56:231.
Wright VC, Davies EM. The conservative management of cervical intraepithelial neoplasia: the use of cryosurgery and the carbon dioxide laser. Br J Obstet Gynaecol. 1981;88:663.
American College of Obstetricians and Gynecologists. Management of abnormal cervical cytology and histology. ACOG Practice Bulletin 66. Obstet Gynecol. 2005;106:645.
American College of Obstetricians and Gynecologists. Evaluation and management of abnormal cervical cytology and histology in the adolescent. ACOG Committee Opinion 330. Obstet Gynecol. 2006;107:963.
Cox JT. Management of cervical intraepithelial neoplasia. Lancet. 1999;353:857.
Ferenczy A. Management of patients with high grade squamous intraepithelial lesions. Cancer. 1995;76:1928.
Figge DC, Creasman WT. Cryotherapy in the treatment of cervical intraepithelial neoplasia. Obstet Gynecol. 1983;62:353.
Gage AA. Cryosurgery in the treatment of cancer. Surg Gynecol Obstet. 1992;174:73.
Kirwan PH, Smith IR, Naftalin NJ. A study of cryosurgery and the CO2 laser in treatment of carcinoma in situ (CIN III) of the uterine cervix. Gynecol Oncol. 1985;22:195.
Ostergard DR. Cryosurgical treatment of cervical intraepithelial neoplasia. Obstet Gynecol. 1980;56:231.