47
Cellulitis

Typical cellulitis of an extremity. An erythematous patch with edema. These findings were accompanied by tenderness in the affected skin and fever.

Cellulitis limited to distal nasal tip. The skin is tender and swollen.

Sharply demarcated erythema, swelling, and tenderness. Usual organisms are S. aureus and group A β-hemolytic Streptococcus pyogenes. Diabetes and lymphedema are risk factors.
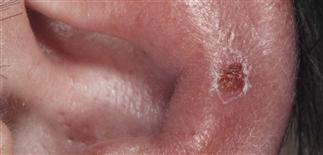
Cellulitis of the pinna may result from infection with Pseudomonas species or with staphylococci and streptococci.
DESCRIPTION
Infection of dermis and subcutaneous tissues characterized by fever, erythema, edema, and pain.
HISTORY
• Localized pain, redness, tenderness, swelling. • Risk factors: diabetes, cirrhosis, renal failure, chemotherapy, immune suppression, malignancy, alcohol, malnourishment, HIV. • Surgical wounds and trauma sites (e.g. bites, burns, abrasions, lacerations, ulcers) are common locations. • Recurrent episodes at sites of compromised venous or lymphatic circulation (i.e. stasis dermatitis). • Ear and lower legs susceptible to recurrence.
PHYSICAL FINDINGS
• Expanding, red, swollen, tender or painful plaque with indefinite border in a small or wide area. • Palpation produces pain, rarely crepitus. • Occasionally, vesicles, blisters, hemorrhage, necrosis, or abscesses. • Regional lymphadenopathy sometimes; lymphangitis common with Streptococcus pyogenes. • Pre-existing lesion: ulcer, erosion, tinea, or dermatitis may be entry portal.
TREATMENT
• Rest, elevation of affected extremity. • Empiric antibiotic coverage: staphylococcal and streptococcal organisms. • Treatment options: dicloxacillin 350–500 mg orally every 6 h, or oral amoxicillin/clavulanate 875 mg/125 mg b.i.d. or 500 mg/125 mg t.i.d. (adult dose), or first-generation cephalosporin, i.e. cephalexin 250–500 mg q.i.d., or azithromycin 500 mg initial dose then 250 mg on days 2–5, or clarithromycin 500 mg every 12 h. • Severe infection may require hospitalization, i.v. antibiotics. Intravenous empiric therapy for group A streptococci and Staphylococcus aureus with cefazolin 1.0 g every 8 h or nafcillin 2 g every 4–6 h. • Clostridial anaerobic cellulitis most commonly caused by Clostridium perfringens, sometimes other clostridia. Pain, soft tissue swelling, and systemic toxicity occur; gas may be palpable or visible by X-ray. Treatment with high-dose i.v. penicillin in addition to prompt surgical exploration and debridement of devitalized tissue. • Infected decubitus ulcers: organisms mixed bowel flora (Gram-negatives, streptococci, anaerobes). • Infection of burns: organisms Pseudomonas aeruginosa, other Gram-negatives, S. aureus, Candida. • Postsurgical cellulitis: Gram-negative organisms, complicated by wound dehiscence and sepsis; coverage for S. aureus, group A streptococci, Gram-negatives. • Gangrenous cellulitis involves extensive necrosis, is a rapidly progressive cellulitis most commonly caused by group A streptococci. Streptococcal gangrene most commonly at site of trauma. Painful erythema followed by edema, bullae, necrosis; may be complicated by rapid bacteremia and septic shock. • Dog and cat bite cellulitis: treat with oral amoxicillin/clavulanic acid 875 mg/175 mg b.i.d. for 7–10 days or 500 mg/125 mg t.i.d., or oral doxycycline 100 mg b.i.d. for 10 days.






