Chapter 1 Cell and Tissue Damage
Cellular Physiology And Pathology
Understanding disease requires knowledge of cellular function and dysfunction.
Plasma Membranes

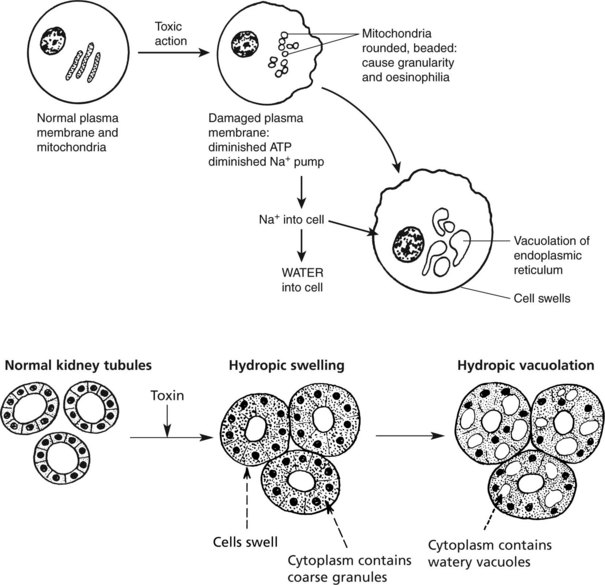
Membrane damage may lead to cellular dysfunction or death.
MITOCHONDRIA These are the main sites of ENERGY production.
Disorder of energy production affects all cellular functions.


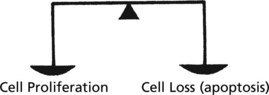
Control of Cell Number
In adult life the CELL NUMBER is fairly constant. Complex control mechanisms evenly balance new cell production with cell loss.
During SOMATIC GROWTH cell proliferation outweighs cell loss.
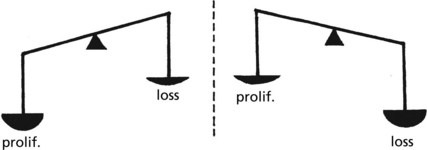
In the ATROPHY of old age, cell loss outweighs cell proliferation.
In many diseases the balance is lost.
Cell Proliferation – the Cell Cycle
In adult life, cells can be classified into 3 groups according to their proliferation potential.
| Proliferation potential | Examples | |
|---|---|---|
| 1. LABILE CELLS | rapid proliferation and cell turnover | gut-lining epithelial cells |
| 2. STABLE CELLS | slow proliferation and cell turnover | hepatocytes |
| 3. PERMANENT CELLS | NOT able to proliferate | neurones |
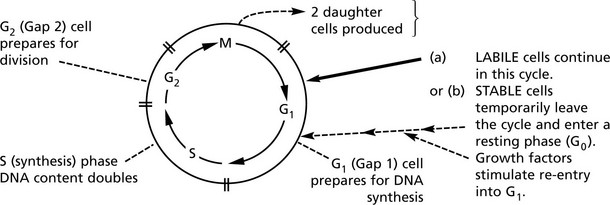
A variety of growth promotors, inhibitors and drugs influence the cycle at various stages.
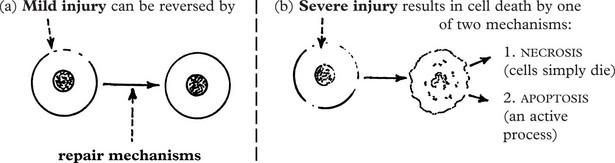
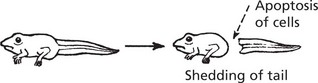
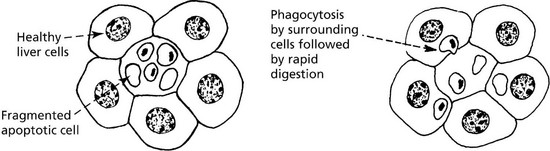
Apoptosis
A variety of noxious agents can damage cells. These include:
The severity of the injury determines the outcome:
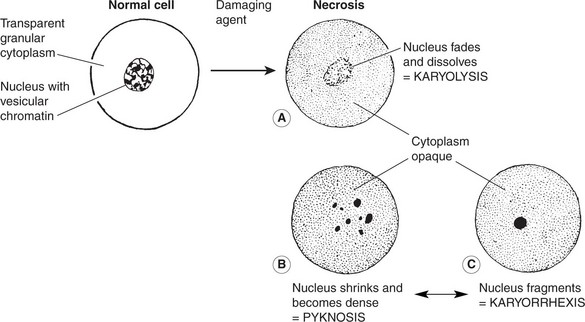
Cell Damage

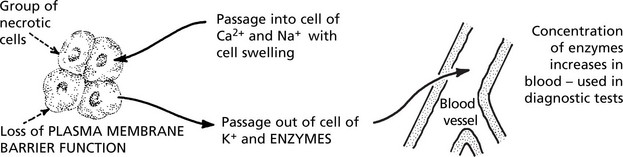
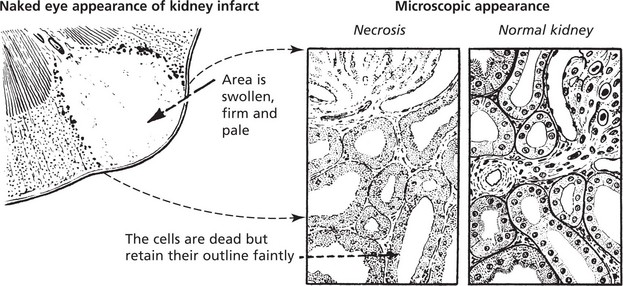
Necrosis
Coagulative Necrosis
This type of necrosis is frequently caused by lack of blood supply, e.g. infarcts of the heart, spleen and kidney.
Colliquative Necrosis (Liquefactive Necrosis)
Death of cells in the brain result in liquefactive necrosis in which the dead cells are broken down to form a liquid mass. There is complete loss of structure (see p. 535).
An abscess (see p.39, 40) is another example of colliquative necrosis.
Gangrene
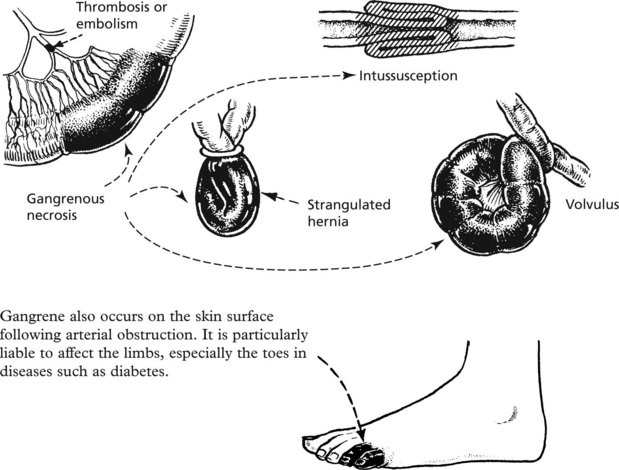
A special type of gangrene follows infection with clostridial organisms (gas gangrene; see p.70).
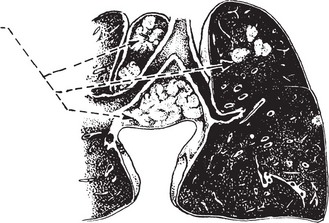
Caseous Necrosis
This is commonly seen in tuberculosis (p. 72). The necrotic tissue has a cream-cheesy appearance.
Necrosis – Autolysis
Cell Damage – Hydropic Swelling
The various agents which can cause cell necrosis may also cause lesser cell damage which is reversible when the injurious agent is removed.
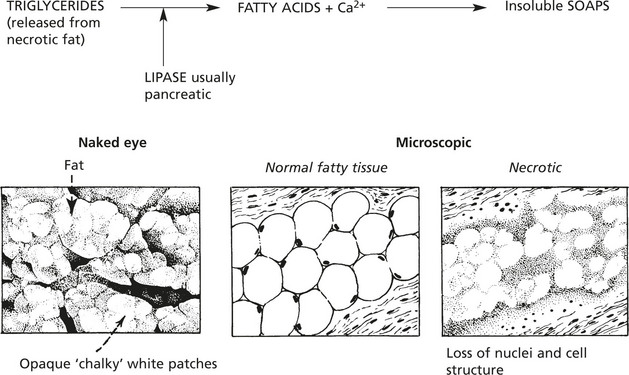
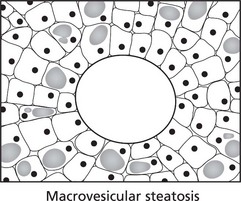
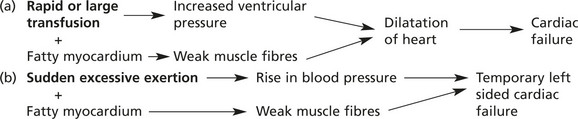
Cell Damage – Fatty Change
Fatty Change
This is accumulation of fat in non-fatty tissues, e.g. skeletal muscles and the heart.

For example, in the LIVER, the increase of deposited fat causes enlargement of the organ.
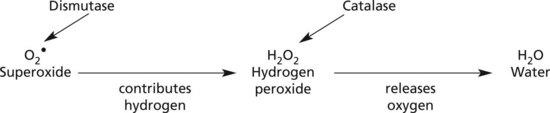
Cell Damage – Free Radicals
The formation of free radicals is an important contributory factor in many disease processes.
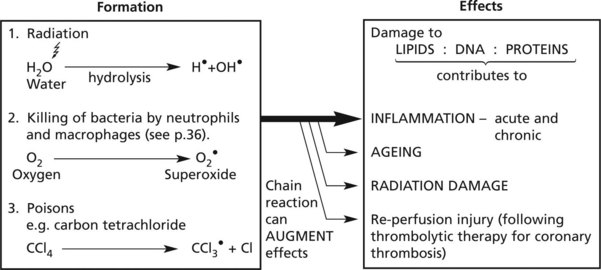
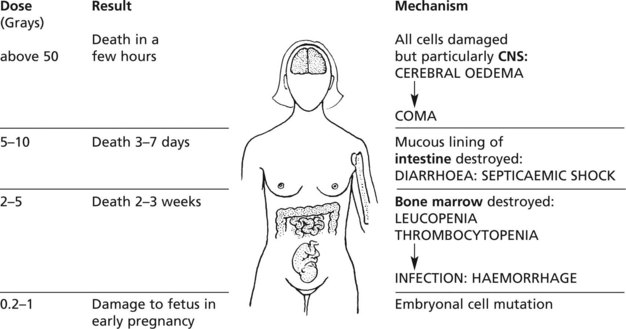
Cell Damage – Radiation
High energy (ionising) radiation, particularly in the form of gamma (γ) or X-rays can cause serious cellular and tissue damage. At cellular level there are 2 mechanisms involving:

These effects will be considered under 3 headings:

Note: Total body irradiation is used in treatment of some leukaemias.
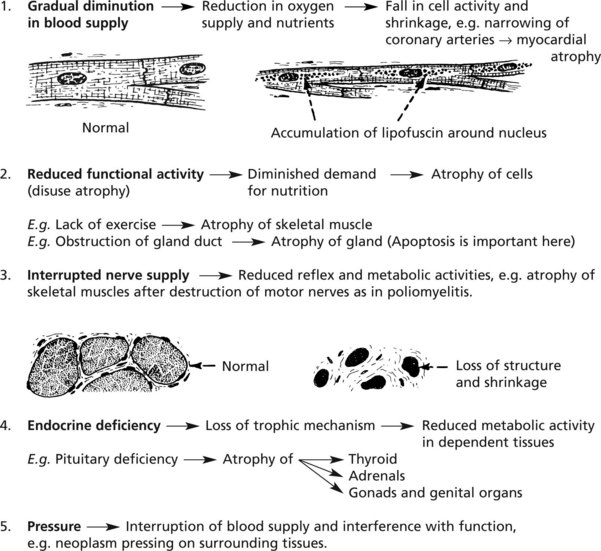
Atrophy
This is a simple decrease in cell size or number, resulting in a shrinkage of affected tissues and organs. The most common example is atrophy of old age (see p.15).
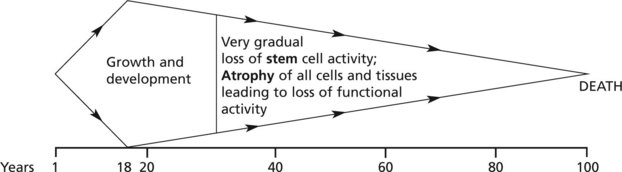
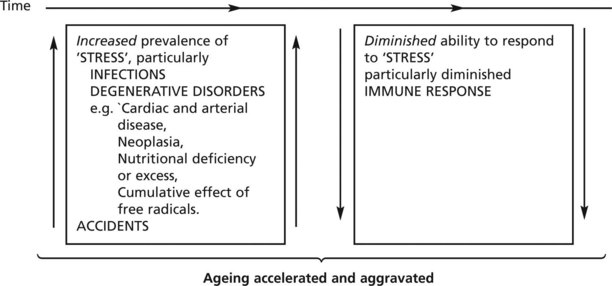
Ageing
The distinction between ‘true’ ageing and ageing complicated by disease processes may be difficult; since therapy can be directed at the latter the distinction is important in clinical practice.
The following diagram is illustrative. The main controlling factors are intrinsic, i.e. genetic:
Heredity, Genes and Disease
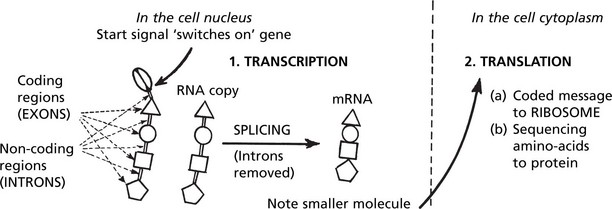
Cell Nucleus and Chromosomes
The cell NUCLEUS contains chromosomes, which transmit hereditary traits from one generation to the next and also control the synthesis of all the proteins in the body.
Chromosomes
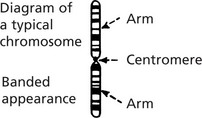
The following features are specific to each chromosome:

Using these morphological criteria each chromosome is identified and numbered 1 to 22.
The sex chromosomes are labelled

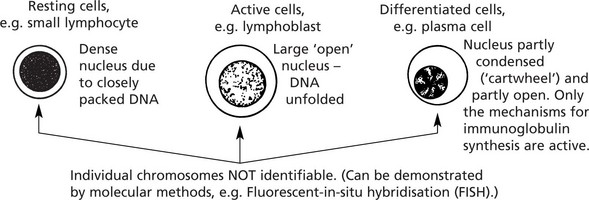
Note: This appearance represents a very condensed and coiled molecular arrangement, i.e. inactive.

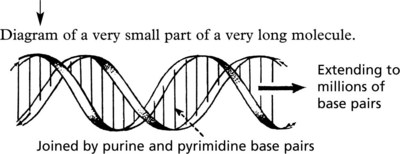
Deoxyribonucleic Acid (DNA)
Since Watson and Crick defined the molecular structure of DNA in 1953, there has been a great increase in knowledge of the ‘genetic code’. Each chromosome is a very long single molecule of deoxyribonucleic acid (DNA), condensed during mitosis. It is extended to its characteristic structure when active:

There are over 10 000 genes in all the human chromosomes, not all are active: some are repetitive: some form clusters subserving related activities (e.g. MHC (HLA) locus, see p.91).
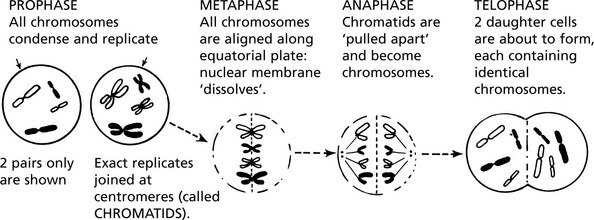
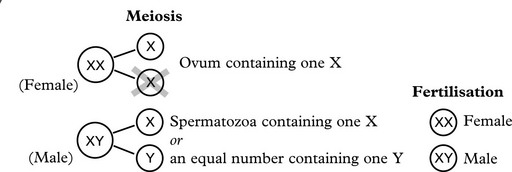
Mitosis and Meiosis
MITOSIS is the process by which somatic cells proliferate ensuring exact replication of the daughter cells. Following the stimulus to proliferate, the chromosomes condense and replicate exactly.
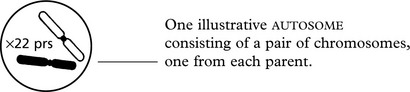
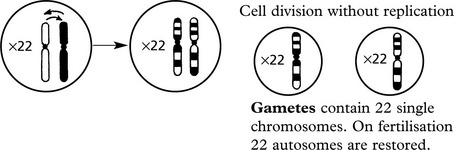
Primitive germ cell contains 46 chromosomes (i.e. 22 autosomes + XX or XY)
Genetic Abnormalities and Associated Disorders
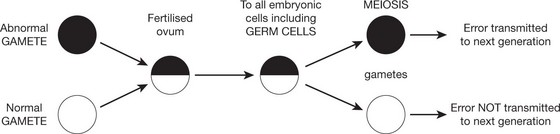
It is not surprising that errors arise during these complex genetic activities. germ cells and proliferating somatic cells (including stem cells) are susceptible to such errors.
They may occur spontaneously or be the result of external influences.
It is important to distinguish between germ cell and somatic cell abnormalities.
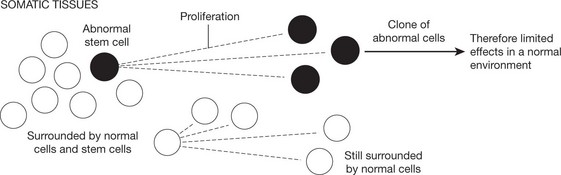
Abnormalities Arising in Somatic Cells
These tend to cause restricted effects: they are not transmitted to the next generation.
Chromosomal Abnormalities
Single Gene Disorders
Factors regulating the production of the final specific protein are extremely complex.
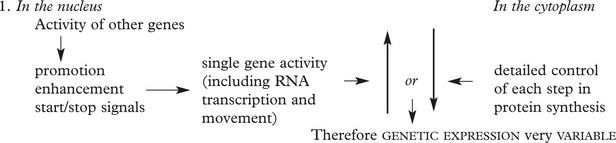

This concept is important in inherited single gene disorders.

The concept of dominant and recessive traits is useful in genetic counselling. Long lists of dominant and recessive disorders are available: only a few important examples are given.

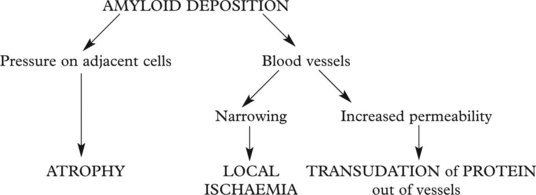
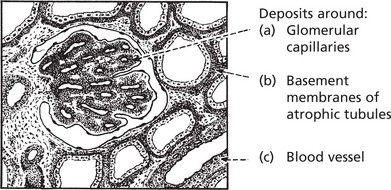
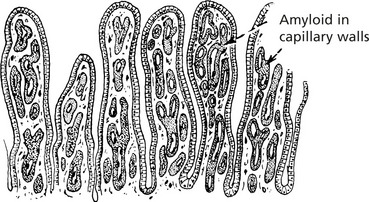
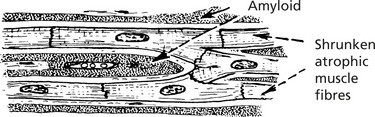
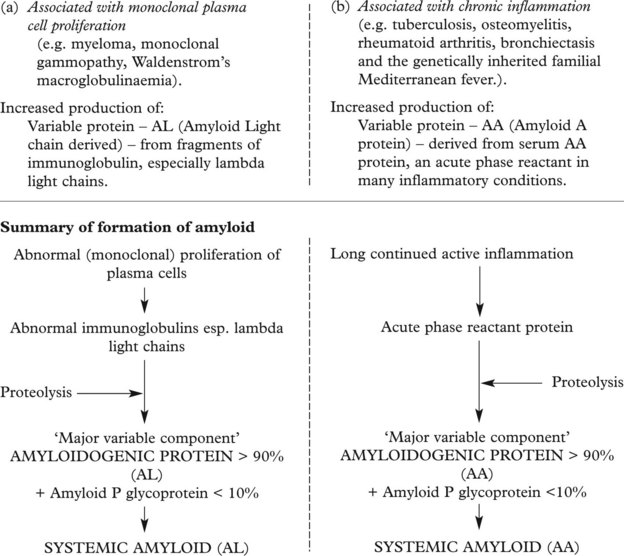
Amyloid Deposition
Amyloid is a waxy substance deposited in the extracellular tissues, particularly around blood vessels and in basement membranes. Various forms of amyloid are seen and they have varying effects. Amyloid is resistant to degradation and its deposition tends to progress relentlessly.



Amyloid Classification
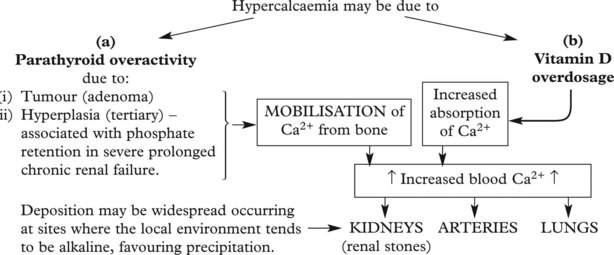
Calcification
Abnormal deposits of calcium occur in 2 circumstances: dystrophic calcification and metastatic calcification.
Local deposits of calcium may occur in:
The mechanism may be as follows:

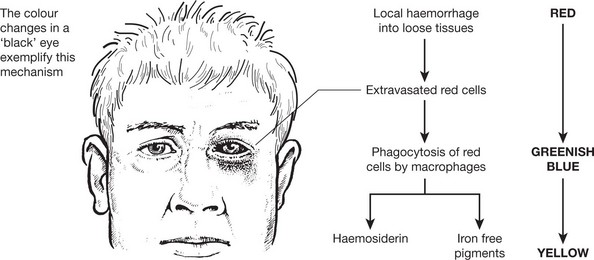
Endogenous Pigmentation
Iron-Containing Pigment
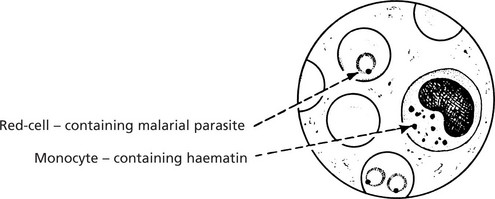
Two main pigments are derived from the breakdown of red blood cells:
1. haemosiderin and 2. bilirubin.
The detailed mechanism is described on page 340 in relation to jaundice.
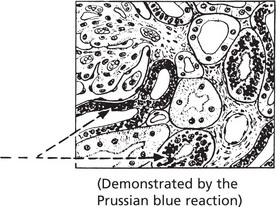
Haemosiderin
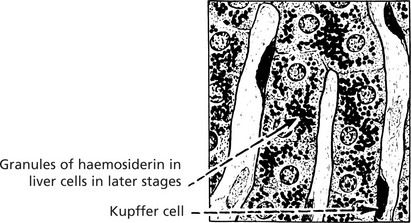
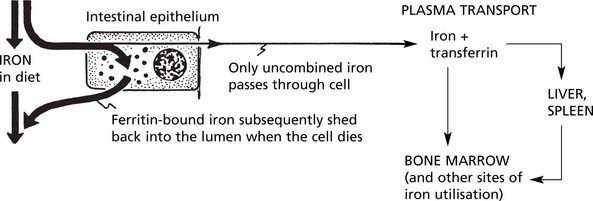
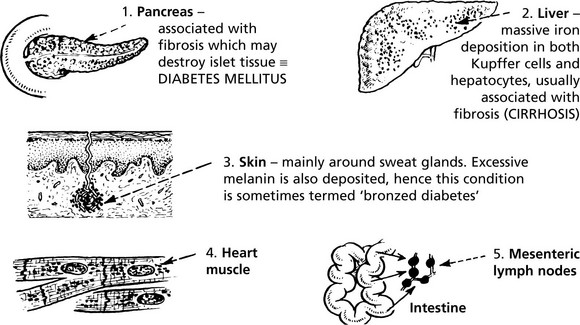
Haemosiderin may be found in almost any site in the body.
Haemoglobin
Intravascular haemolysis can result in haemoglobin appearing in the urine, giving it a dull red colour. In severe acute haemolysis (e.g. incompatible blood transfusion) acute renal tubular necrosis occurs. In chronic haemolysis (e.g. paroxysmal haemoglobinuria), some of the haemoglobin is reabsorbed and subsequently broken down so that iron, as haemosiderin, appears in the renal tubular epithelium.

Exogenous Pigmentation – Degenerations
Exogenous Pigmentation
Pigments may be introduced by inhalation, ingestion or injection.
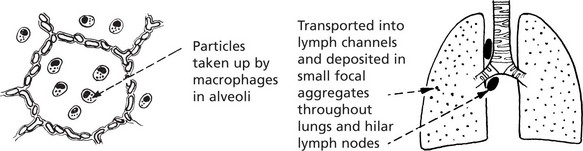
Inhalation
The commonest substances inhaled are coal dust (carbon) – black, and stone dust (silica) – grey.