Gastric and esophageal, ± duodenal submucosal edema
Best evaluated by CECT
Caustic agents cause intense pylorospasm, so duodenal injury is less common
• Acute: Severe
Pneumoperitoneum (perforation)
• Chronic phase
Gastric outlet obstruction (antral scarring and fibrosis)
Linitis plastica: Small, aperistaltic stomach with effaced folds
Best evaluated by upper GI series
TOP DIFFERENTIAL DIAGNOSES
• Gastric carcinoma (scirrhous type)
• Gastric metastases and lymphoma
• Gastric thermal injury (iced saline)
CLINICAL ISSUES
• Prognosis
Acute mild phase with early treatment: Good
Acute severe and chronic phases: Poor
• Treatment
Conservative treatment for stable patients
– Antibiotics, steroids, parenteral feedings
Gastric outlet obstruction
– Gastroenterostomy or partial gastrectomy
– Complete gastrectomy with colonic interposition
(Left) Axial NECT shows tremendous thickening of the wall of the stomach and ascites. These findings suggest transmural inflammation and a high likelihood of subsequent necrosis and perforation of the stomach.
(Right) Axial NECT of the same patient shows diffuse involvement of the entire stomach . The patient subsequently had gastric perforation and died.
(Left) Upright film from an upper GI series in a 24-year-old man who drank drain cleaner several days prior shows delayed gastric emptying with fluid levels . Note the fixed contraction (linitis plastica) of the body and antrum of the stomach .
(Right) Film from an upper GI series in a 56-year-old man who drank acid several weeks prior demonstrates a linitis plastica appearance of the stomach being small, rigid, nondistensible, and without peristalsis.
Upper GI series shows an extremely small, nondistensible, distorted stomach due to the ingestion of hydrochloric acid.













 and ascites. These findings suggest transmural inflammation and a high likelihood of subsequent necrosis and perforation of the stomach.
and ascites. These findings suggest transmural inflammation and a high likelihood of subsequent necrosis and perforation of the stomach.
 . The patient subsequently had gastric perforation and died.
. The patient subsequently had gastric perforation and died.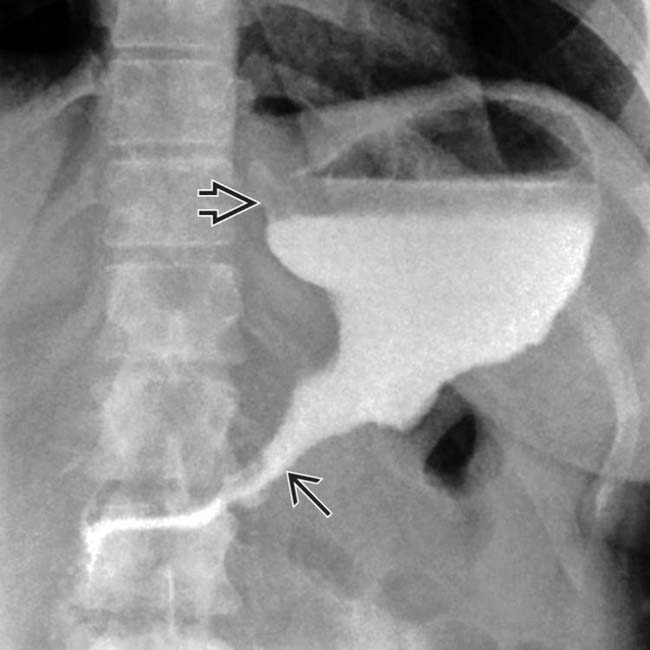
 . Note the fixed contraction (linitis plastica) of the body and antrum of the stomach
. Note the fixed contraction (linitis plastica) of the body and antrum of the stomach  .
.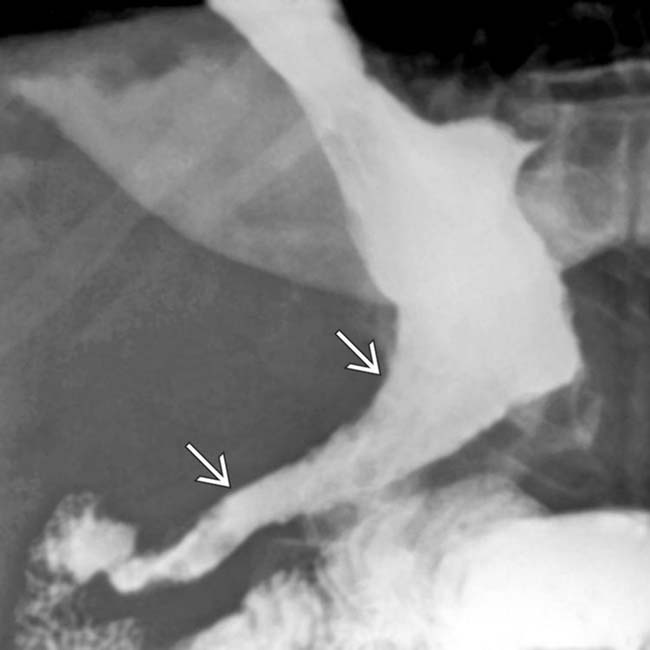
 being small, rigid, nondistensible, and without peristalsis.
being small, rigid, nondistensible, and without peristalsis.


