25 Cardiac Trauma
Blunt Cardiac Trauma
Pericardial Sequelae




Myocardial Sequelae
 Myocardial damage is produced in the area underlying the impact, but also may occur elsewhere in the heart, often on the opposite wall.
Myocardial damage is produced in the area underlying the impact, but also may occur elsewhere in the heart, often on the opposite wall.
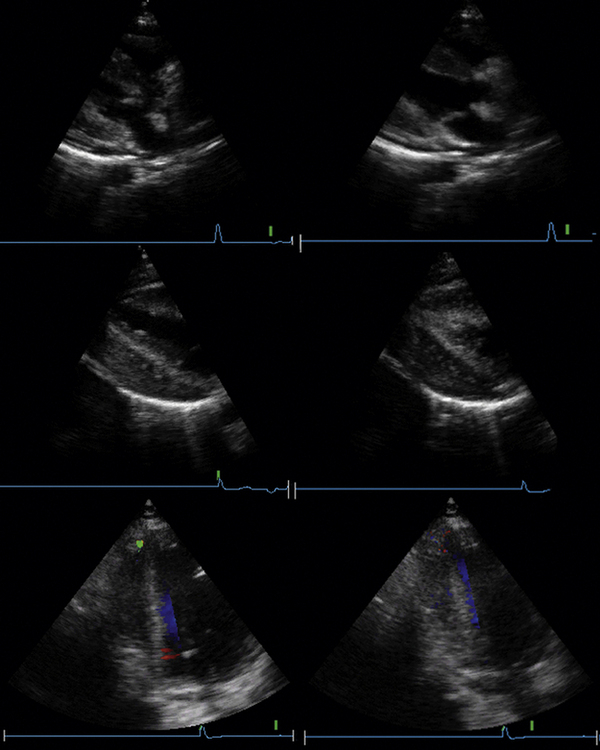
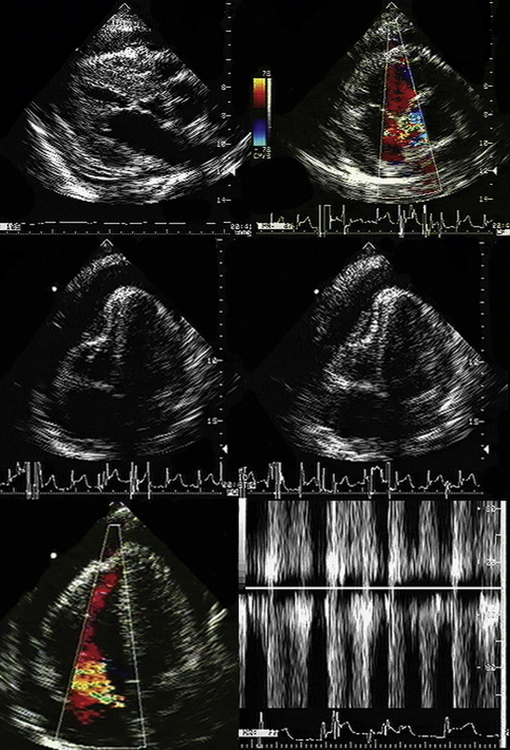
 Echocardiographic features of myocardial contusion include
Echocardiographic features of myocardial contusion include
 There is a spectrum of severity of myocardial contusion. Echocardiography is most likely to be sensitive to severe degrees of contusion, but some authors have questioned its sensitivity to less severe degrees of contusion.1
There is a spectrum of severity of myocardial contusion. Echocardiography is most likely to be sensitive to severe degrees of contusion, but some authors have questioned its sensitivity to less severe degrees of contusion.1
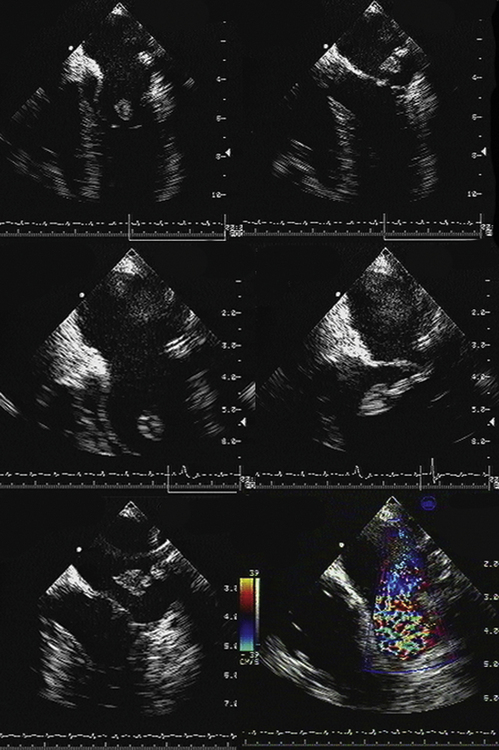
 Cardiac rupture may occur due to breakdown of myocardium post-contusion, due to violent compression of the heart, puncture by a rib, or coronary disruption or thrombosis from trauma. Ventricular septal defect,2 free wall rupture, tamponade, and pseudoaneurysms have all occurred.
Cardiac rupture may occur due to breakdown of myocardium post-contusion, due to violent compression of the heart, puncture by a rib, or coronary disruption or thrombosis from trauma. Ventricular septal defect,2 free wall rupture, tamponade, and pseudoaneurysms have all occurred.



Penetrating Cardiac Trauma
 In the urban milieu, the missiles that most commonly penetrate the heart are knives and bullets.
In the urban milieu, the missiles that most commonly penetrate the heart are knives and bullets.
 Most (60–80%), but not all, of these wounds are fatal, often immediately.
Most (60–80%), but not all, of these wounds are fatal, often immediately.
 The clinical presentation is usually tamponade or bleeding into the chest.
The clinical presentation is usually tamponade or bleeding into the chest.

 Bullet wounds commonly involve the left ventricle.
Bullet wounds commonly involve the left ventricle.
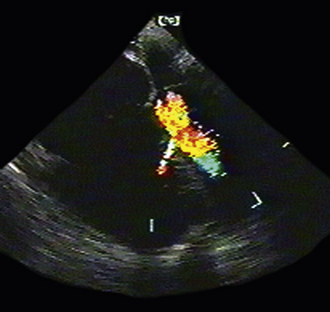
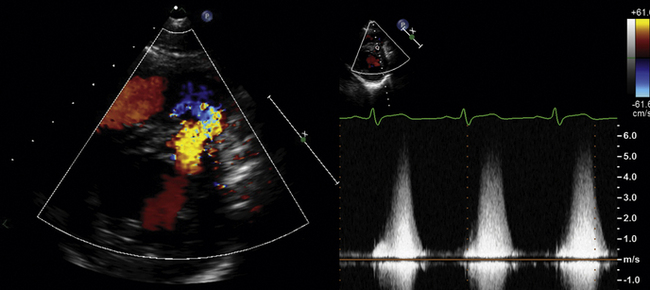
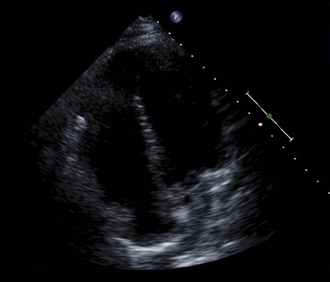
 Puncture of a cardiac chamber may result in the following:
Puncture of a cardiac chamber may result in the following:



Missiles within the Heart
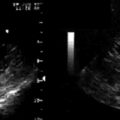
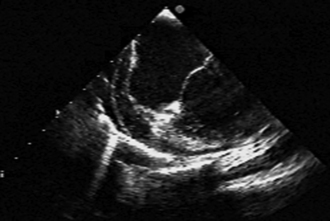
 Echocardiography may help localize a missile within the heart by imaging the location and motion6:
Echocardiography may help localize a missile within the heart by imaging the location and motion6:
 Some missiles may be free within a cardiac chamber.
Some missiles may be free within a cardiac chamber.
 Bullets and shotgun pellets are conspicuous by their tail of reverberations.
Bullets and shotgun pellets are conspicuous by their tail of reverberations.
Blunt Aortic Trauma
 As many as one sixth of motor vehicle deaths are caused by aortic rupture.
As many as one sixth of motor vehicle deaths are caused by aortic rupture.
 Eighty percent of patients with aortic rupture die outright.
Eighty percent of patients with aortic rupture die outright.
 Twenty percent get to the hospital; of those who survive to the hospital, 70% may survive.
Twenty percent get to the hospital; of those who survive to the hospital, 70% may survive.


 Ninety percent of blunt injuries to the aorta involve either:
Ninety percent of blunt injuries to the aorta involve either:
 Lesions that may occur include the following:
Lesions that may occur include the following:
 TEE has a major contribution to offer to the diagnosis of traumatic injury to the aorta.
TEE has a major contribution to offer to the diagnosis of traumatic injury to the aorta.
Indications for Transesophageal Echocardiography in Cardiac Trauma
 When the transthoracic echocardiographic study quality is not adequate
When the transthoracic echocardiographic study quality is not adequate
 To exclude disruption of the aorta when other tests are equivocal
To exclude disruption of the aorta when other tests are equivocal
Transthoracic Echocardiography
ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocardiography7


ACC/AHA/ASE 2003 Guideline Update for the Clinical Application of Echocardiography
Conditions and Settings in which TEE Provides the Most Definitive Diagnosis in the Critically Ill and Injured






Recommendations for Echocardiography in the Critically Injured*




TABLE 25-1 Utility of Different Imaging Modalities and Cardiac Catheterization in the Assessment of Cardiac and Aortic Trauma
| Modality | Pros | Cons/Caveats |
|---|---|---|
| Transthoracic Echocardiography | 2D echocardiography |
• Unlikely to recognize specific cardiac injury; more likely to recognize complications of cardiac injuries
• Pulmonary contusion and aspiration findings may confound the recognition of heart failure.
• Without a lateral view, it is difficult to localize projectiles within the heart.
• Will not image nonradiopaque projectiles
• Mediastinal hematomas are not synonymous with traumatic disruption of the aorta.
2D, two-dimensional; NA, not applicable; TEE, transesophageal echocardiography; TEVAR, thoracic endovascular aortic repair; TTE, transthoracic echocardiography; VSD, ventral septal defect.
1. Hossack K.F., Moreno C.A., Vanway C.W., Burdick D.C. Frequency of cardiac contusion in nonpenetrating chest injury. Am J Cardiol. 1988;61:391-394.
2. Boland M.J., Martin H.F., Ball R.M. Nonpenetrating traumatic ventricular septal defect: two-dimensional echocardiographic and angiographic findings. Am J Cardiol. 1985;55:1242-1243.
3. Rehr R.B., Mack M., Firth B.G. Aortic regurgitation and sinus of Valsalva-right atrial fistula after blunt thoracic trauma. Br Heart J. 1982;48:410-412.
4. Pandian N.G., Skorton D.J., Doty D.B., Kerber R.E. Immediate diagnosis of acute myocardial contusion by two-dimensional echocardiography: studies in a canine model of blunt chest trauma. J Am Coll Cardiol. 1983;2:488-496.
5. Sareli P., Goldman A.P., Pocock W.A., et al. Coronary artery-right ventricular fistula and organic tricuspid regurgitation due to blunt chest trauma. Am J Cardiol. 1984;54:697-699.
6. Hassett A., Moran J., Sabiston D.C., Kisslo J. Utility of echocardiography in the management of patients with penetrating missile wounds of the heart. J Am Coll Cardiol. 1986;7:1151-1156.
7. Douglas P.S., Garcia M.J., Haines D.E., et al. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 appropriate use criteria for echocardiography. J Am Coll Cardiol. 2011;57(9):1126-1166.
8. Taylor A.J., Cerqueira M., Hodgson J.M., et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. J Am Coll Cardiol. 2010;56(22):1864-1894.
9. Hendel R.C., Berman D.S., Di Carli M.F., et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide imaging. J Am Coll Cardiol. 2009;53(23):2201-2229.