70
Candidiasis of large skin folds
(candidal intertrigo)
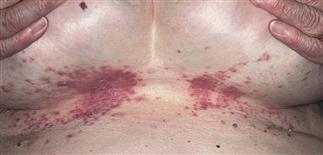
Yeast thrives in warm moist areas created by skin folds. Pendulous breasts in older women predispose. Red plaques appear, increasing in size. Satellite pustules appear beyond plaque edge.

Candida infections of the axillae occur in the obese, especially in warm humid weather. The red plaques with satellite pustules occur just as they do under the breasts and on groin.

Maceration causes pustules to rupture and skin to scale. Painful fissures may develop at the base of the skin fold.

A white fringe of scale may appear at the junction where skin surfaces diverge and no longer touch. Satellite papules and pustules are seen along the edge of involved areas.
DESCRIPTION
Intertrigo is skin fold inflammation. Many causes. Psoriasis causes red, glistening plaques with macerated scale. Groin and axillae commonly affected. Seborrheic dermatitis looks just like psoriasis. Can appear on scalp and intertriginous areas, especially in infants. Accumulation of moisture in obese people predisposes to skin irritation, eczema. These compromised, warm, intertriginous areas frequently colonized and infected with Candida species. Topical steroid use favors yeast growth within fold areas.
HISTORY
• Warm, moist, intertriginous areas where skin touches skin are a breeding ground for yeast. Skin folds retain heat and moisture, providing suitable environment for yeast infection. Infection occurs under pendulous breasts, between overhanging abdominal folds, in groin and rectal area, and in axillae. • Infection occurs in winter, when warm tight clothing promotes heat retention. Sweating and poor hygiene promote infection in hot, humid weather. • Persons with diabetes are predisposed.
PHYSICAL FINDINGS
• Most common finding: slowly evolving, red, moist, glistening plaques extending to or just beyond limits of apposing skin folds. Inflammation becomes more intense with deep erythema. Erosions occur in chronic cases. Painful fissures eventually form at base of folds. • Acute infections show different pattern. Begin with bright-red plaques in skin folds. This pattern is commonly seen under breasts. Pustules form but become macerated under apposing skin surfaces, and develop into red papules with a fringe of moist scale at border. Intact pustules may be found outside apposing skin surfaces.
TREATMENT
• Topical medication effective in most cases. • Warm, moist conditions must be eliminated. • Apply antifungal cream in a thin layer twice a day until rash clears. Miconazole, clotrimazole, ketoconazole, oxiconazole, or econazole is applied in a thin layer twice a day. • Daily application of a group VII topical steroid suppresses inflammation and controls itching and pain. • Use cool, wet, Burow’s or tap water compress 20–30 min several times daily to promote dryness. Apply compress right after application of medication. Continue use until skin remains dry. • Fluconazole 100 mg q.d. for 7 days used for resistant cases. Potential drug interaction between oral hypoglycemic agents and fluconazole requires careful monitoring of blood sugars with concomitant use. • Medicated or non-medicated absorbent powder (Zeasorb) may be applied after inflammation is gone. Powder absorbs moisture and acts as a dry lubricant, allowing skin surfaces to slide freely, preventing moisture accumulation in a potentially stagnant area. • Weight loss eliminates folds and avoids recurrence.






