Cancer and its consequences
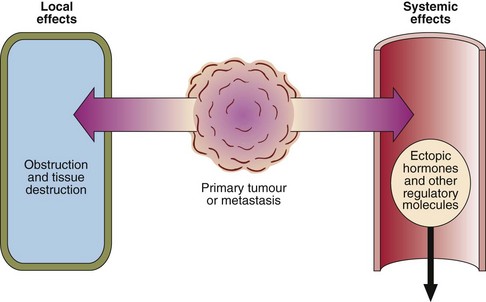
In Western societies one death in five is caused by cancer. The effects of tumour growth may be local or systemic (Fig 69.1), e.g. obstruction of blood vessels, lymphatics or ducts, damage to nerves, effusions, bleeding, infection, necrosis of surrounding tissue and eventual death of the patient. The cancer cells may secrete toxins locally or into the general circulation. Both endocrine and non-endocrine tumours may secrete hormones or other regulatory molecules.
A tumour marker is any substance that can be related to the presence or progress of a tumour (see pp. 140–141).
Local effects of tumours
Renal failure may occur in patients with malignancy for the following reasons:









Ectopic hormones
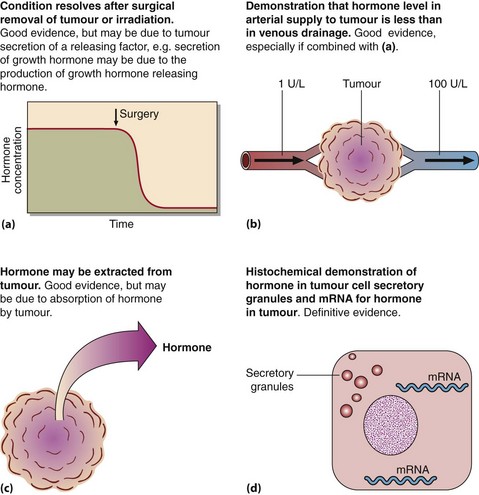
It is a characteristic feature of some cancers that they secrete hormones, even though the tumour has not arisen from an endocrine organ. Referred to as ectopic hormone production, hormone secretion by tumours has frequently been invoked but rarely proven (Fig 69.2). Small cell carcinomas are the most aggressive of the lung cancers and are the most likely to be associated with ectopic hormone production. Ectopic ACTH secretion causing Cushing’s syndrome is the most common. However, the classic clinical features of Cushing’s syndrome are not usually apparent in the rapidly progressing ectopic ACTH disorder. Biochemical features include hypokalaemia and metabolic alkalosis and these may be the sole indicators of the problem.
Consequences of cancer treatment

 Clinical note
Clinical note
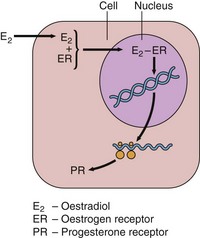
The measurement of oestrogen and progesterone receptors in biopsy material has been used to determine which breast cancer patients will respond to endocrine therapy, e.g. with the anti-oestrogen tamoxifen. As the synthesis of progesterone receptors is dependent on oestradiol, the presence of both receptors indicates the integrity of the oestrogen receptor mechanism in the tumour cells (Fig 69.3). The prognostic value of this is still controversial.
Cancer and its consequences
 Cancer may cause clinical signs and symptoms in patients by causing obstruction, exerting pressure or destroying normal tissue.
Cancer may cause clinical signs and symptoms in patients by causing obstruction, exerting pressure or destroying normal tissue.
 Cancer cachexia is characterized by anorexia, lethargy, muscle wasting, weight loss and anaemia.
Cancer cachexia is characterized by anorexia, lethargy, muscle wasting, weight loss and anaemia.
 Some non-endocrine tumours secrete hormones, e.g. lung cancers may secrete ACTH.
Some non-endocrine tumours secrete hormones, e.g. lung cancers may secrete ACTH.

