104 Bronchogenic carcinoma
Salient features
History
• Symptoms related to primary tumour: cough, dyspnoea, haemoptysis, postobstructive pneumonia)
• Symptoms related to mediastinal spread:
• Symptoms related to metastases:
• Systemic effects: anorexia, weight loss, weakness and profound fatigue.
Questions
How may patients with bronchogenic carcinoma present?
• Cough (in 80%), haemoptysis (70%) and dyspnoea (60%); loss of weight, anorexia
• Skeletal manifestations: clubbing (in 30%)
• Local pressure effects: recurrent laryngeal palsy, superior vena caval obstruction, Horner syndrome
• Endocrine manifestations (12% of the tumours)—in particular small cell tumours—present with syndrome of inappropriate antidiuretic hormone (SIADH), hypercalcaemia, adrenocorticotrophic hormone (ACTH) secretion or gynaecomastia. SIADH does not usually cause symptoms. When Cushing syndrome occurs, the manifestations are primarily metabolic (hypokalaemic alkalosis)
• Neurological manifestations: Eaton–Lambert syndrome, cerebellar degeneration, polyneuropathy, dementia, proximal myopathy, encephalomyelitis, subacute sensory neuropathy, limbic encephalitis, opsoclonus, myoclonus
• Cardiovascular: thrombophlebitis migrans, atrial fibrillation, pericarditis, non-bacterial thrombotic endocarditis
• Cutaneous manifestations: dermatomyositis, acanthosis nigricans, herpes zoster
• Anaemia, disseminated intravascular coagulation, thrombotic thrombocytopenic purpura. Hypercoagulatopathy in the form of venous thromboembolism is seen especially with adenocarcinoma
How would you investigate this patient?
• Sputum cytology: high yield for endobronchial tumours such as squamous cell and small cell carcinoma) but the yield is poor for adenocarcinoma
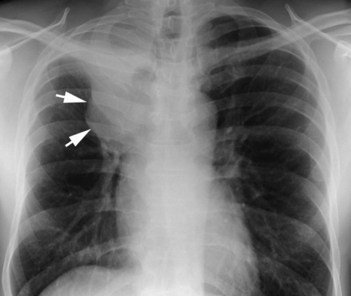
• Chest radiography (Fig. 104.1)
• Bronchoscopy gives a high yield in excess of 90%, particularly when the tumour is viewed endobronchially. For tumours that are not visualized, the yield for washing and brushing is about 75% in central lesions and 55% in peripheral lesions. The yield in small cell and squamous cell carcinomas is higher than adenocarcinomas
• CT scan of the chest and upper abdomen (to image the liver and adrenals)
• Bone scan for metastases (helpful in staging)
• PET scanning is highly sensitive and specific for mediastinal staging
• Pulmonary function tests (most surgeons aim for a FEV1 of about 1000 ml after planned resection), a DLCO (carbon monoxide diffusing capacity of the lung) <60% predicted is associated with a mortality rate as high as 25% as a result of respiratory complications.
Advanced-level questions
What are the drugs used in non-small-cell lung cancer?
• Old agents: cisplatin, carboplatin, etopside, vinblastine, vindesine
• Newer agents: docetaxel, paclitaxel, irinotacen, vinorelbine, gemcitabine
• Vascular endothelial growth factor (VEGF) inhibitors: bevacizumab
• Epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (e.g. gefitinib, erlotinib. cetuximab): most effective in women, patients who have never smoked, patients with pulmonary adenocarcinomas and patients of Asian origin.
What are the indications for radiotherapy?
Radiotherapy is administered for palliation in the following circumstances:






