10 Breast disease
Benign breast disease
Breast lumpiness and lumps
It is vital, but sometimes difficult, to distinguish whether a breast lump is part of a diffuse lumpiness or a discrete, isolated lump. The diagnosis may be influenced by whether the lump is painful and/or the age of the patient (Table 10.1).
Table 10.1 Likely diagnosis of discrete breast lumps at different ages
| Young adult | Fibroadenoma |
| Middle-aged | Cyst |
| Elderly | Carcinoma |
Breast cancer
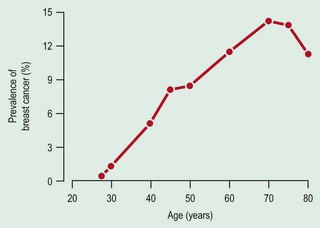
Epidemiology and aetiology
The risk factors for breast cancer are listed in Table 10.2.
| Factor | High risk | Low risk |
|---|---|---|
| Age (years) | Greater than 50 | Less than 35 |
| Country of birth | Northern Europe, North America | Asia or Africa |
| First-degree relative affected | Yes | |
| Age at first pregnancy | >30 years | <20 years |
| Nulliparity | Yes | |
| Previous breast cancer | Yes | |
| History of atypical hyperplasia | Yes |
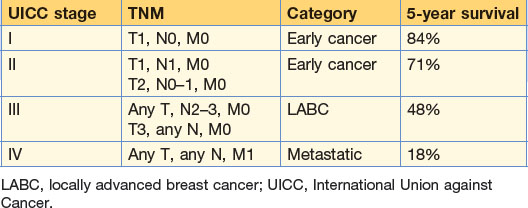
Staging and prognosis
The TNM classification of breast cancer is shown in Table 10.3, and the prognosis in Table 10.4.
| TNM stage | Pathological description |
|---|---|
| Tis | Carcinoma in situ (pre-invasive) |
| Paget’s disease (no palpable tumour) | |
| T0 | No clinical evidence of primary tumour |
| T1 | Tumour less than 2 cm |
| T2 | Tumour 2–5 cm |
| T3 | Tumour greater than 5 cm |
| T4 |
Breast cancer pathology
Invasive breast cancer
The histological types of invasive breast cancer are summarised in Table 10.5.
Table 10.5 Relative frequency of histological types of breast cancer
| Type | Frequency (%) |
|---|---|
| Ductal | 80 (non-specific 50%) |
| Lobular/ductal combined | 5 |
| Medullary | 6 |
| Colloid | 2 |
| Other less common specific types (tubular, papillary) | 2 |
| Sarcoma and lymphoma | 0.5 |
Carcinoma in situ
DCIS is subdivided into commode, solid, cribriform and micropapillary patterns.
Table 10.5 shows the relative frequency of the histological types of breast cancer. Ductal with productive fibrosis is the commonest form. Lobular carcinomas have a high propensity for bilaterality, multicentricity and multifocality and have a particular propensity for metastasising to membrane structures, for example the peritoneum, pleura and meninges.
Clinical features
The lump is solitary, firm, non-tender and may be tethered to the skin or pectoral fascia. In advanced cases, the lymphatic channels are blocked and the skin becomes oedematous with thickening (peau d’orange). Very advanced tumours may ulcerate (Fig. 10.2). Axillary lymph nodes may be palpable.

Diagnosis
Examination
Inspection and palpation of the entire breast and lymph node areas is mandatory. The breast is examined with the patient sitting facing the examiner with the arms first at the side then raised above the head and then placed on the hips to both relax and contract the pectoral muscles. The doctor assesses asymmetry, visible lumps, erythema, peau d’orange, contour flattening, skin tethering (puckering), abnormal fixation, retraction and altered axis of the nipples or obvious gross ulceration. Skin retraction may also be determined by asking the patient to lean forward (Fig. 10.3). The supraclavicular, infraclavicular and axillary lymph nodes should be examined with the examiner taking the weight of the patient’s arm, either on the shoulder or opposite arm (Fig. 10.4). Palpation of the breast is performed in the supine position with the patient’s hand behind the head initially and then at the side. Examine the whole breast, from sternum to clavicle, latissimus dorsi to rectus sheath. Examination occurs one quadrant at a time with the flat of the hand followed by the nipple/areola area. The breast lump should be categorised by its position, size, consistency and any fixation to deep or superficial structures. Mobility should be assessed. If the patient complains of discharge, an attempt to reproduce this should be made (Table 10.6).


| Symptom/sign | Frequency (%) |
|---|---|
| Lump | 76 |
| Pain | 5 |
| Nipple retraction | 4 |
| Nipple discharge | 2 |
| Skin retraction | 1 |
| Axillary mass | 1 |
Treatment of breast cancer
Breast reconstruction
Reconstruction is considered as a functional restoration of appearance and self-image. Potential patients are usually younger and reconstruction may be carried out at the same time as mastectomy. Techniques include latissimus dorsi flaps, which may allow radiotherapy and chemotherapy to begin shortly after surgery. Reconstruction can also be achieved using implanted expanders and prostheses. The aims of reconstructive surgery are to reproduce symmetry of breast form, including consistency and size, with a lasting result with no detrimental effects on treatment and outcome of the primary disease. See also Chapter 18.