[level-membership-for-pediatrics-category]
CHAPTER 4 Branchial Anomalies
Step 1: Surgical Anatomy


Step 2: Preoperative Considerations
Step 3: Operative Steps
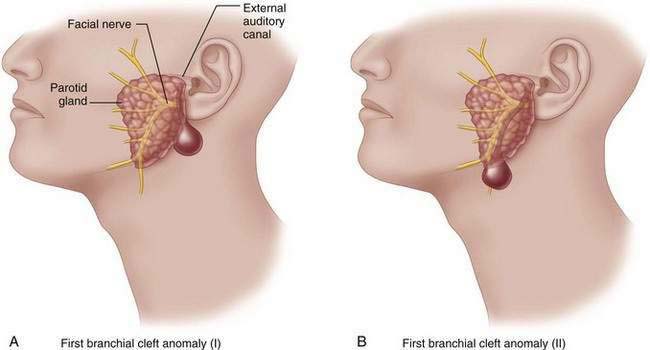
First Branchial Anomalies
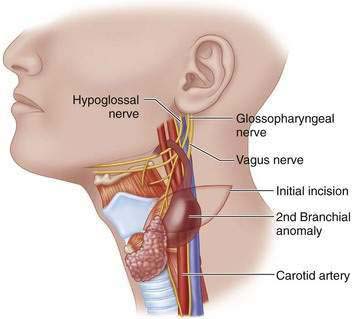
Second Branchial Anomalies
Large Cysts
Fistulas and Small Cysts

Third and Fourth Branchial Anomalies (Pyriform Fossa Sinus Tracts)
Open Operation
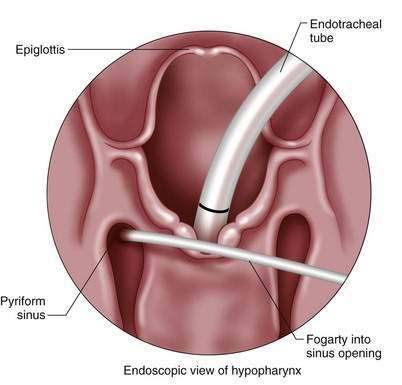
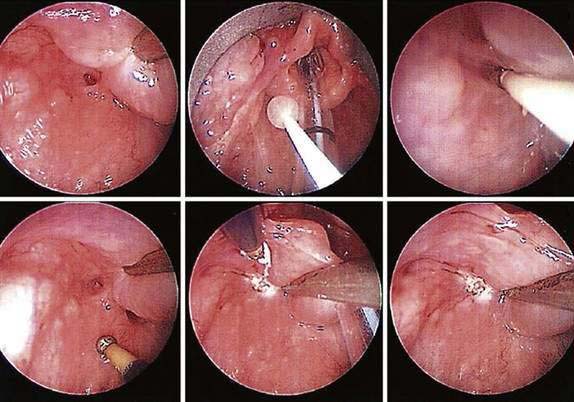
Endoscopic Sinus Cauterization
Step 4: Postoperative Care
Step 5: Pearls and Pitfalls
Acierno SP, Waldhausen JHT. Congenital cervical cysts, sinuses, and fistulas. Otolaryngol Clin North Am. 2007;40:161-176.
Houck J. Excision of branchial cysts. Operative Techn Otolaryngol. 2005;16:213-222.
James A, Stewart C, Warrick P, Tzifa C, Forte V. Branchial sinus of the piriform fossa: reappraisal of third and fourth branchial anomalies. Laryngoscope. 2007;117(11):1920-1924.
Jordan JA, Graves JE, Manning SC, McClay JE, Biavati MJ. Endoscopic cauterization for treatment of fourth branchial cleft sinuses. Arch Otolaryngol Head Neck Surg. 1998;124(9):1021-1024.
Liberman M, Kay S, Emil S, et al. Ten years’ experience with third and fourth branchial remnants. J Pediatr Surg. 2002;37:685-690.
Pereira KD, Davies JN. Piriform sinus tracts in children. Arch Otolaryngol Head Neck Surg. 2006;132:1119-1121.
Sai Prasad TR, Chong Cl, Mani A, et al. Acute suppurative thyroiditis in children secondary to pyriform sinus fistula. Pediatr Surg Int. 2007;23(8):779-783.
Schroeder JW, Mohyuddin N, Maddalozzo J. Branchial anomalies in the pediatric population. Otolaryngol Head Neck Surg. 2007;137(2):289-295.
Smith CD. Cysts and sinuses of the neck. In: Grosfeld JL, O’Neill JA, Coran AG, Fonkalsrud EW, editors. Pediatric surgery. 6th ed. Philadelphia: Mosby Elsevier; 2006:861-869.
Tracy TJ, Muratore CS. Management of common head and neck masses. Semin Pediatr Surg. 2007;16(1):3-13.
Verret DJ, McClay J, Murray A, Biavati M, Brown O. Endoscopic cauterization of fourth branchial cleft sinus tracts. Arch Otolaryngol Head Neck Surg. 2004;130(4):465-468.
Waldhausen JHT, Tapper D. Head and neck sinuses and masses. In: Ashcraft KW, Holcomb GW, Murphy JP, editors. Pediatric surgery. 4th ed. Philadelphia: Saunders; 2005:1054-1057.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
CHAPTER 4 Branchial Anomalies
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
Step 3: Operative Steps
First Branchial Anomalies
[/not-level-membership-for-pediatrics-category]
