[level-membership-for-neurosurgery-category]
Chapter 4 Brachial Plexus Injury Types
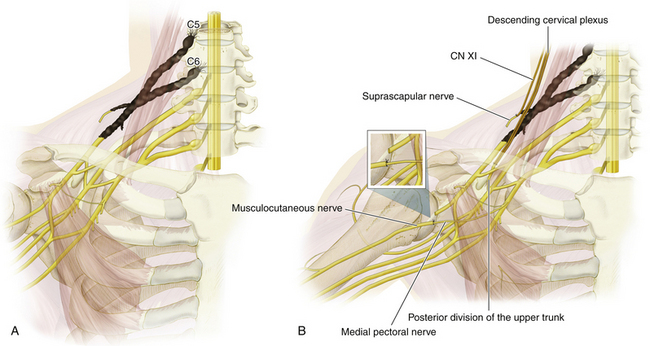
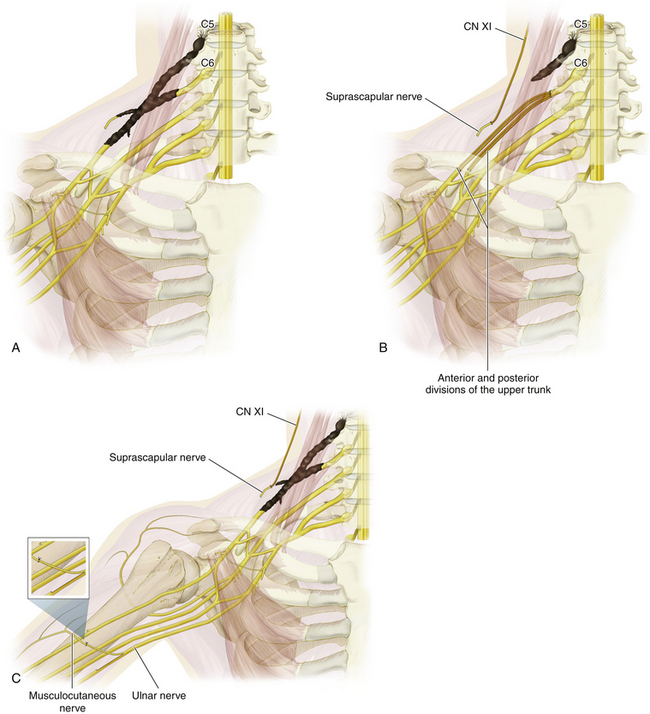
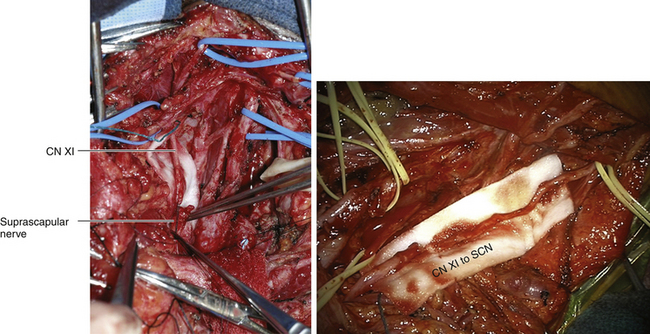
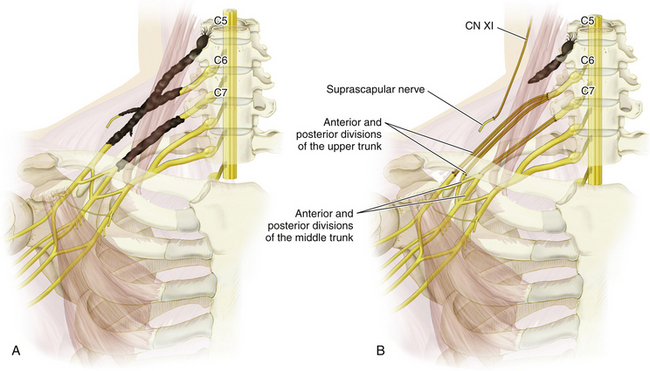
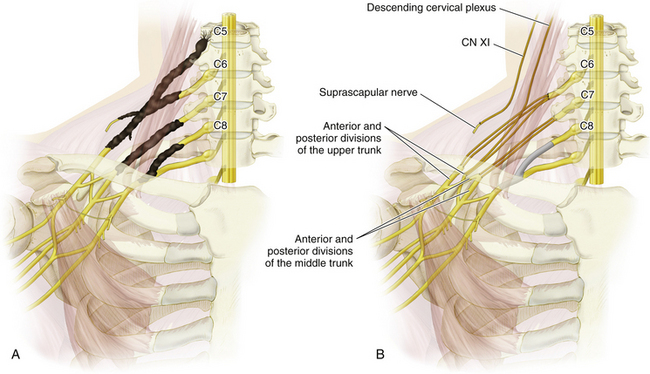
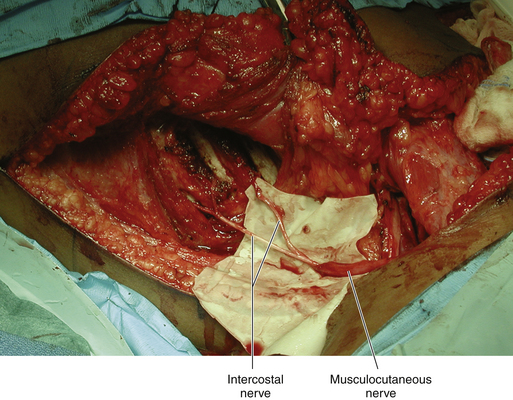
Figure 4-8 Intraoperative photo of nerve transfer of the intercostal nerve to the musculocutaneous nerve.
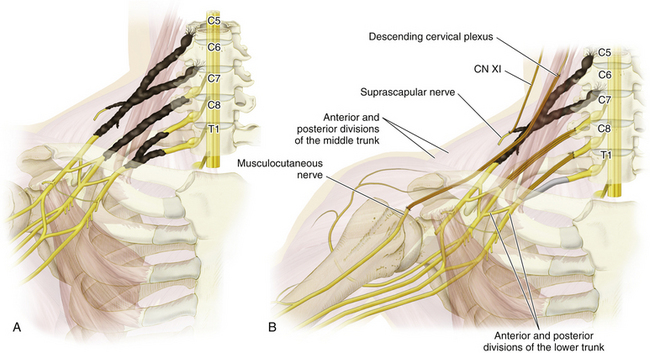
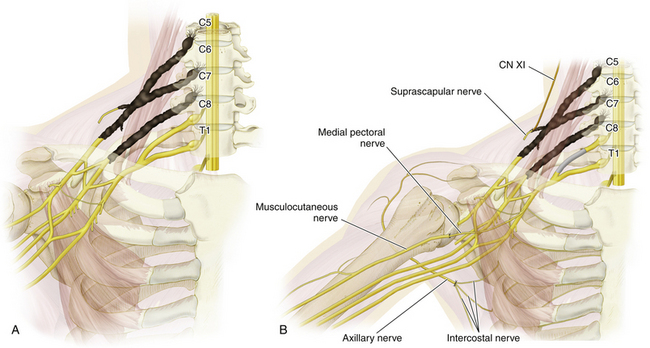
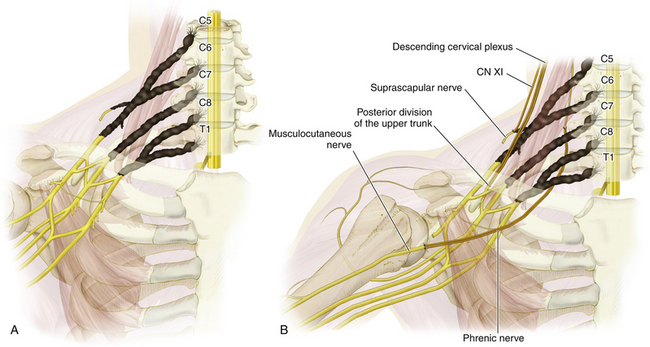

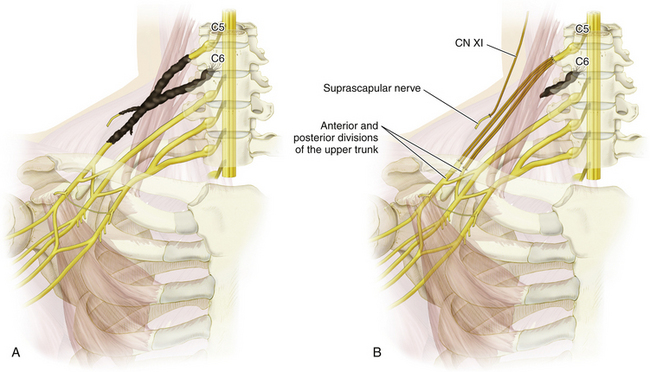
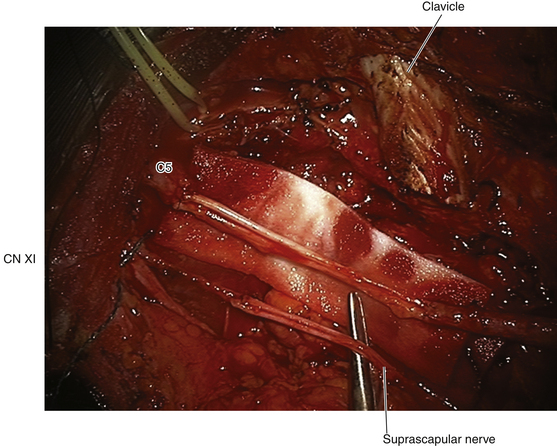
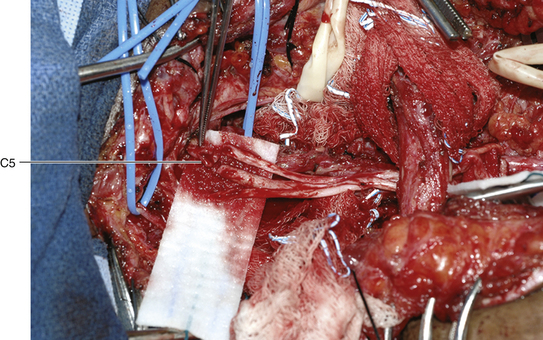
Figure 4-16 C5 interfascicular graft repair to the anterior and posterior divisions of the upper trunk.

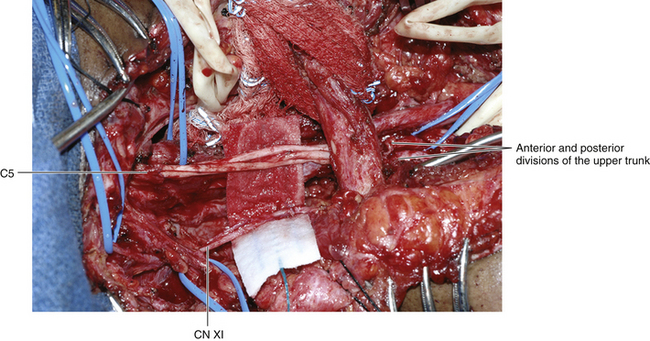
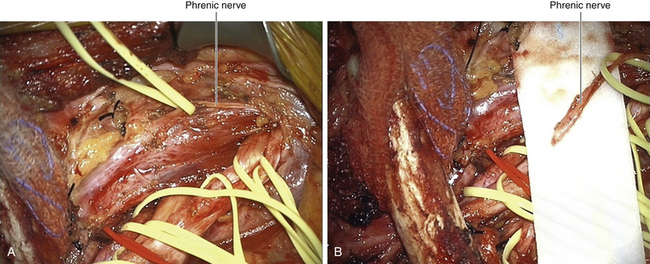
Figure 4-18 C5 graft repair to the anterior and posterior divisions of the upper trunk and of CN XI to the SCN.
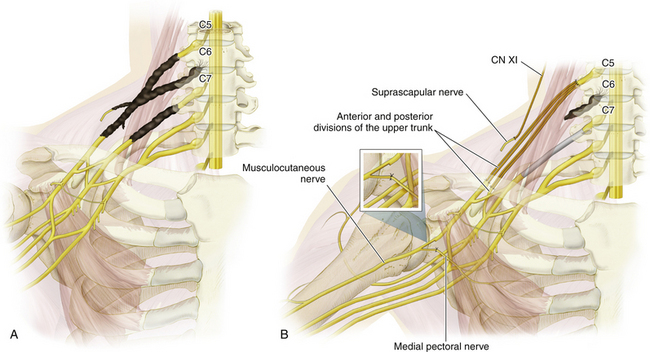
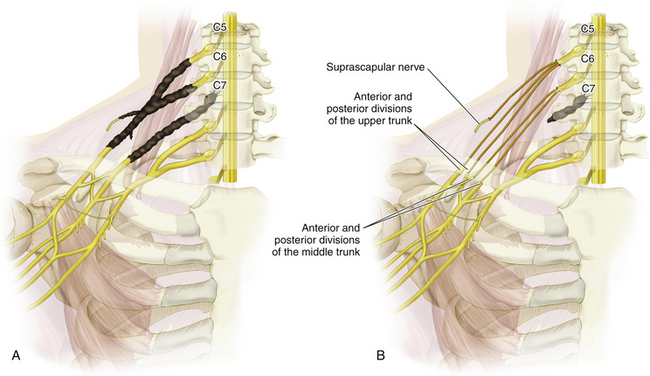
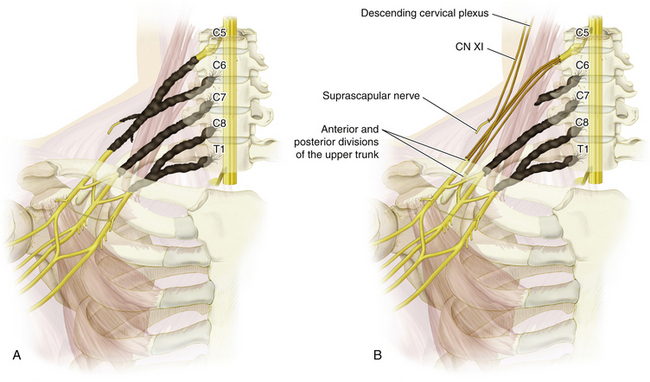
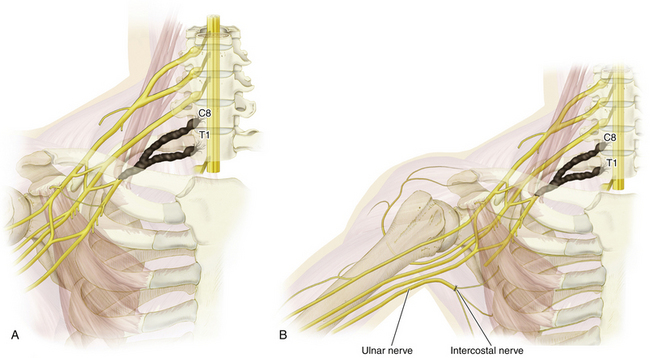
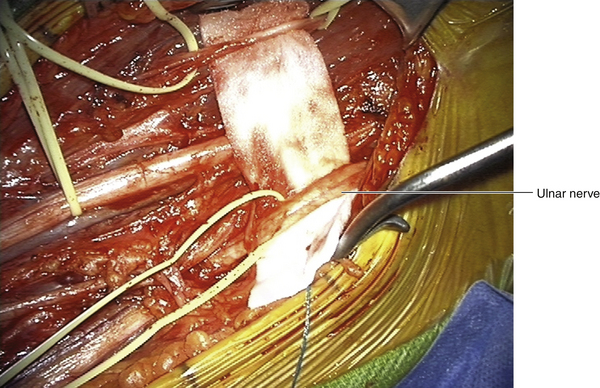
Figure 4-22 A, C8 to T1 preganglionic injury. B, Repair with an intercostal nerve transfer to the ulnar nerve.
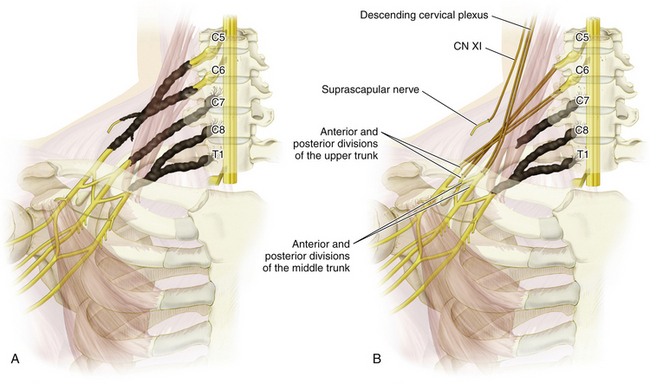
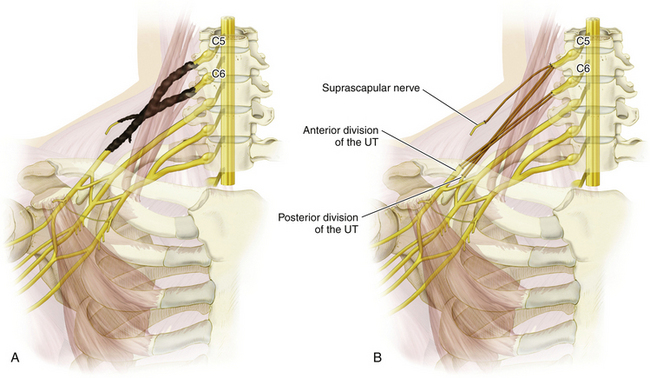
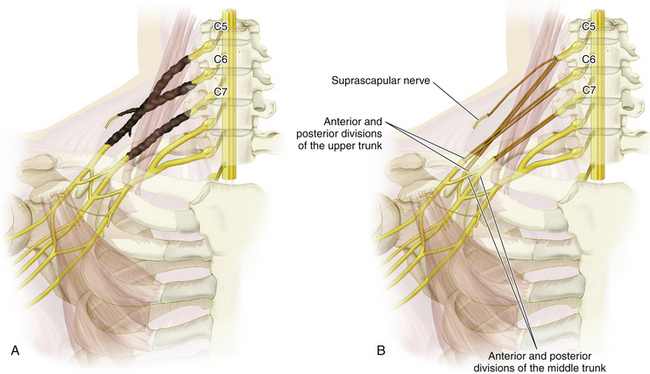
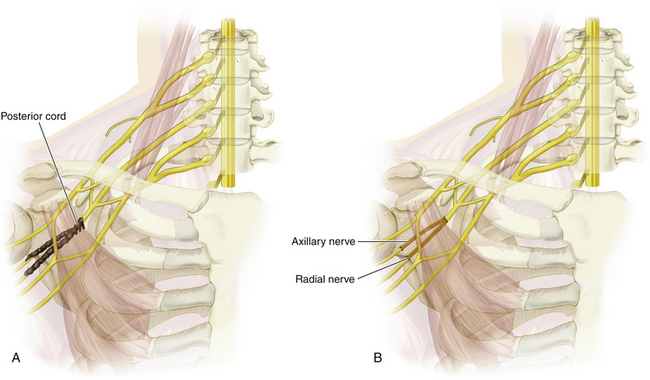
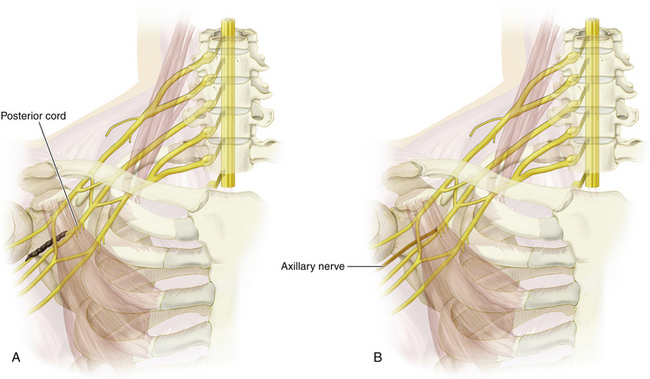
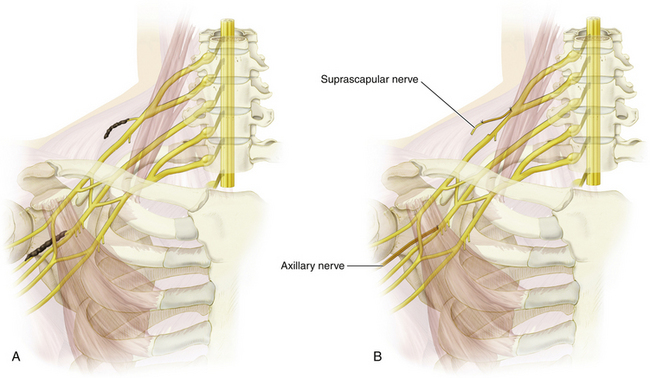
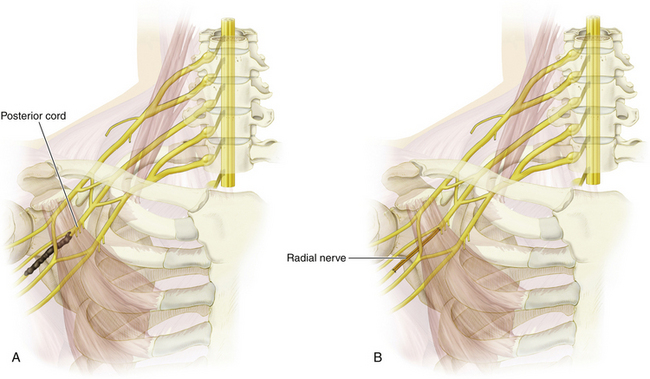
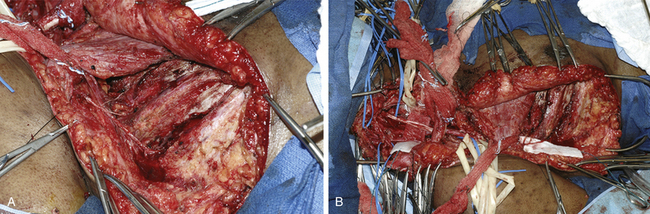
Figure 4-30 A, Posterior cord to radial nerve injury. B, Repair with a posterior cord graft repair to the radial nerve.
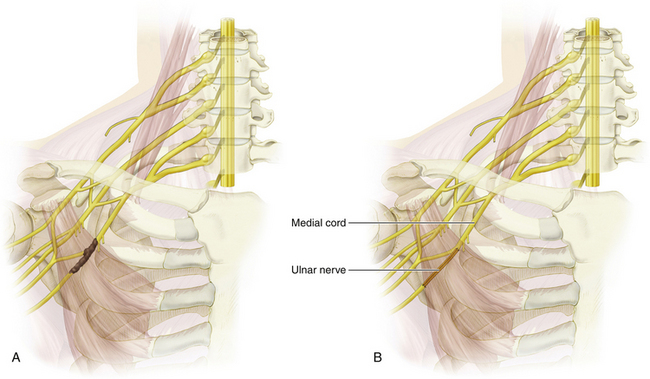
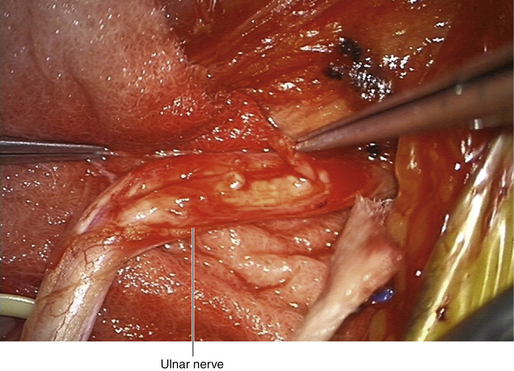
Figure 4-31 A, Medial cord to ulnar nerve injury. B, Repair with a medial cord graft repair to the ulnar nerve.
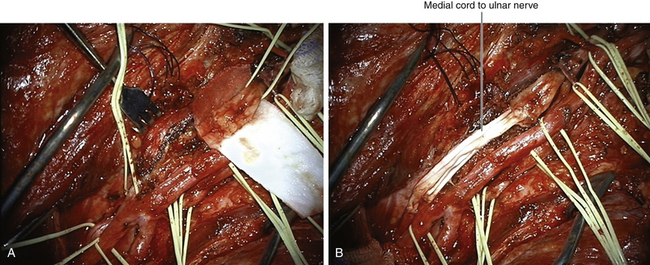
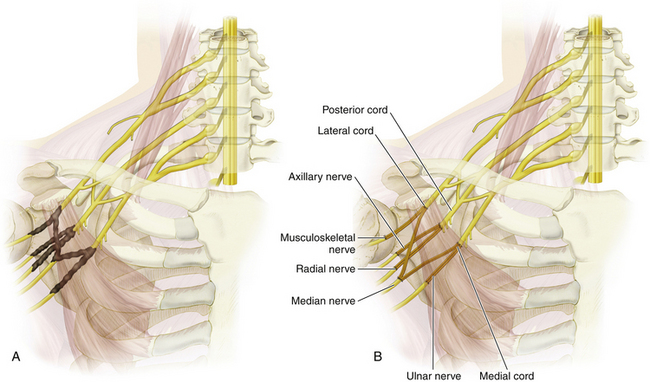
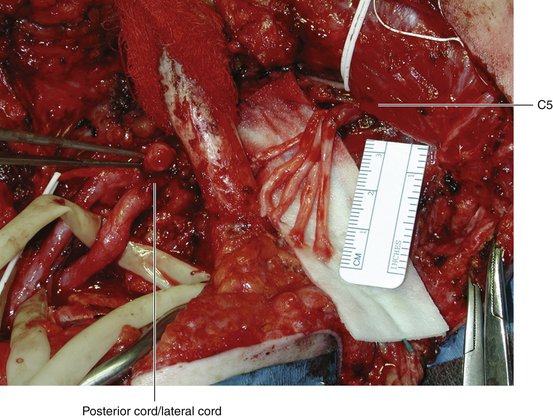

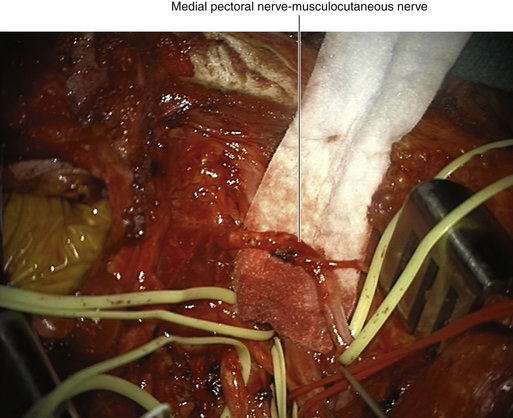

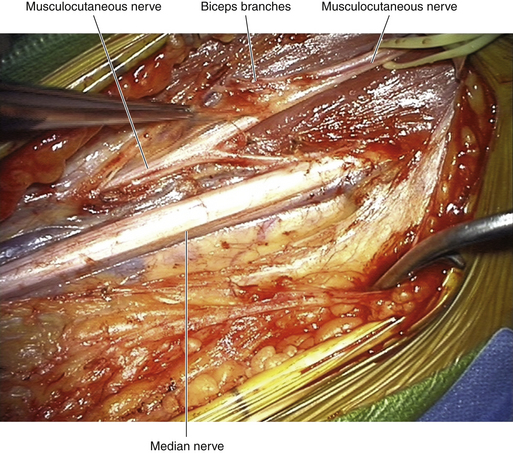
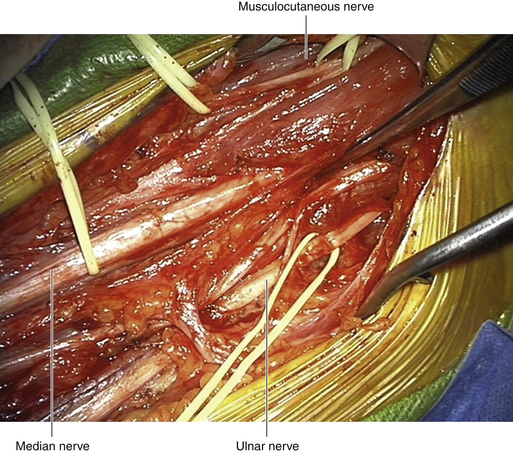
Figure 4-38 Nerve transfer of the medial pectoral nerve to the biceps branches of the musculocutaneous nerve.
[/level-membership-for-neurosurgery-category][not-level-membership-for-neurosurgery-category]
Chapter 4 Brachial Plexus Injury Types
Figure 4-8 Intraoperative photo of nerve transfer of the intercostal nerve to the musculocutaneous nerve.
