129
Bowen disease
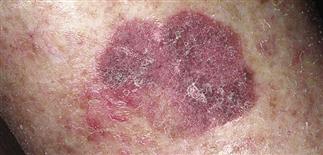
Bowen disease is a slowly growing lesion with in situ or intraepithelial atypical squamous cells. This plaque looks like psoriasis.

The diagnosis of Bowen disease is often not made until after biopsy. This plaque looks like actinic keratosis.

Bowen disease of the penis showing a mild pink to red inflammatory patch on the glans; may be confused with psoriasis or lichen planus. If diagnostic doubt exists, confirm with biopsy.

Bowen disease may arise in sun-exposed and sun-protected areas. It may be patch or plaque-like and resemble eczema or psoriasis.
DESCRIPTION
An intraepidermal (in situ), primary cutaneous malignancy arising from keratinocytes of the skin. Considered an early variant of squamous cell carcinoma. Arises in both sun-exposed and sun-protected areas. Etiologies include ultraviolet light (actinic), chemicals such as arsenic, and human papillomavirus.
HISTORY
• Lesions are persistent and slowly enlarge over months to years. Slow progression ultimately leads to invasion. • They are minimally symptomatic, and patients often delay seeking care. • Unlike actinic keratoses (partial thickness), Bowen disease represents full-thickness replacement of the epidermis with tumor cells. Bowen disease is less common and a potentially more aggressive lesion.
PHYSICAL FINDINGS
• Solitary, barely raised, red plaque with adherent dry scale or irregularly fissured, adherent scale. Border is slightly elevated and very well demarcated. Little if any inflammation is present. • May resemble a single plaque of psoriasis or eczema. • Focal areas of pigmentation may resemble pigmented basal cell carcinoma and lentigo maligna. • Over many years, the plaque extends laterally, becoming an invasive squamous cell carcinoma. • Erythroplasia of Queyrat is also squamous cell carcinoma in situ occurring on the glans penis. These lesions are red, sharply defined, and have a moist, glistening surface. Analogous in situ lesions occur on the vulva. These lesions can progress into squamous cell carcinoma. Erythroplasia of Queyrat has a greater tendency toward invasion and metastases, estimated at 10–30%.
TREATMENT
• Bowen disease should be treated as invasive squamous cell carcinoma until proven to be in situ squamous cell carcinoma by biopsy. • Destruction or excision of Bowen disease is optimal. Other treatment modalities include curettage, cryosurgery, topical 5-fluorouracil, and imiquimod cream. • Close follow-up after any treatment is mandatory. Any areas suspicious for recurrence should be biopsied or excised without delay.






