[level-membership-for-opthalmology-category]52
Boston Keratoprosthesis Outcomes
Introduction
The Boston Keratoprosthesis™ (Boston KPro) was developed at the Massachusetts Eye and Ear Infirmary for the treatment of corneal blindness in patients who otherwise have a poor prognosis for a standard penetrating keratoplasty (PKP). Since its approval by the FDA in 1992, the Boston KPro has become the most commonly used keratoprosthesis device in the United States. Over 3500 Boston keratoprosthesis devices have been implanted worldwide, with the vast majority having been implanted since 2006.1
Advances in the Boston Keratoprosthesis to Improve Outcomes
Several advances in both the design of the Boston type I keratoprosthesis and in our understanding of the postoperative management of these patients have led to improved outcomes and contributed to the popularity of the surgery.1 Major postoperative complications, such as corneal melting, keratoprosthesis extrusion, and endophthalmitis can lead to removal of the keratoprosthesis and significant vision loss. However, even retroprosthetic membranes, which are the most common postoperative complications after keratoprosthesis surgery, may lead to vision decline.
Current design features of the Boston keratoprosthesis that have helped to improve retention of the KPro include holes in the back plate of the KPro, a threadless design, and a titanium locking ring.2–4 The holes in the back plate of the KPro allow nutrients, such as glucose to pass from the aqueous to the corneal carrier tissue.2 An early study showed a statistically significant decrease in tissue necrosis or melt around a keratoprosthesis from 51% of eyes with a solid PMMA back plate to 10% of eyes of eyes with a back plate with holes.2 The threadless design of the stem of the KPro prevents misthreading or inadequate threading of the back plate, a design that previously led to gaps between the front plate and the cornea carrier tissue and resulting anterior protrusion of the front.3 Anterior protrusion of the KPro was associated with tissue melting around the stem.3 The titanium locking ring helps prevent intraocular loosening of the KPro postoperatively.4
Postoperatively, the use of a bandage contact lens and long-term vancomycin drops has been instrumental to reducing vision-threatening complications of keratoprosthesis surgery. Bandage contact lenses improve outcomes by decreasing the risk of corneal melting from desiccation of the ocular surface.5
Long-term topical vancomycin eye drops (14 mg/mL) help decrease the risk of bacterial endophthalmitis.6 Bacterial endophthalmitis is a devastating complication associated with a very poor visual outcome.6 In their retrospective review of bacterial endophthalmitis in KPro eyes between 1990 and 2006, Durand and Dohlman. found that only two of 18 eyes regained useful vision.6 Eight of 18 eyes in their review lost light perception vision entirely, with five eyes retaining only hand motions or light reception vision.6 Fortunately, they also found a statistically significant lower incidence of bacterial endophthalmitis in patients on topical vancomycin prophylaxis, compared with those on a single commercially available antibiotic agent alone (0.35% versus 4.13% per patient-year, p = 0.001).6 Keratoprosthesis surgeons now routinely use topical vancomycin in combination with another commercially available broad-spectrum antibiotic agent, although the precise regimen varies among surgeons.1
Finally, decreasing the frequency of retroprosthetic membrane formation may also help improve long-term visual outcomes after KPro surgery. Although visually significant retroprosthetic membranes can typically be treated with a simple YAG membranotomy, some membranes may be refractory to laser treatment, causing a decline in vision and necessitating more aggressive surgical removal.7–9 In some instances, the retroprosthetic membrane may be recalcitrant even to surgical removal.9 A titanium back plate for the Boston keratoprosthesis is currently being evaluated at the Massachusetts Eye and Ear Infirmary. The preliminary findings are encouraging, with a trend towards decreased postoperative inflammation and less frequent formation of retroprosthetic membranes in patients with a titanium back plate.10
Early Postoperative Outcomes of the Boston Type 1 Keratoprosthesis
Early postoperative outcomes for the Boston type 1 keratoprosthesis are generally excellent. Table 52.1 highlights studies looking at shorter-term outcomes (average follow-up period < 12 months). Within the first few months after surgery, visual improvement is often drastic. Dunlap et al. reported short-term visual outcomes of the Boston type I keratoprosthesis and found that in their series of 126 eyes, 82.5% (104 eyes) had improved visual acuity within the first 6 months.11 Of those 104 eyes, 31 eyes (30%) achieved best-corrected vision within 1 week of surgery.11 By postoperative month 1, 59 eyes (54%) had achieved their best-corrected visual acuity.11 The 22 eyes which did not have an improvement in visual acuity postoperatively had co-morbid conditions limiting visual potential.11
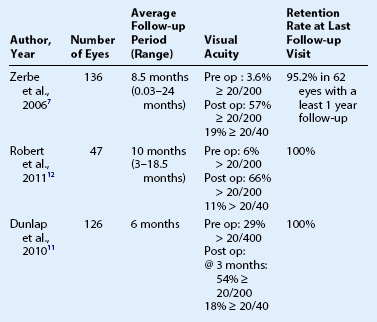
Robert and Harissi-Dagher reported similar outcomes in their patients.12 In a group of 47 eyes, they observed that 84% had an improvement of best-corrected visual acuity, with the median visual acuity improving from hand motions preoperatively to 20/150 by postoperative month 3.12 There was 100% anatomic retention of the keratoprosthesis in these patients.12
Zerbe et al. also reported positive outcomes in the United States multicenter study.7 Postoperatively, 57% of eyes had a best-corrected vision of 20/200 or better, compared to just 3.6% preoperatively.7 There was a 95% rate of KPro retention in this study.7
Interestingly, even in their relatively short follow-up period (average, 10 months; range, 3–18.5 months), Robert and Harissi-Dagher had four patients (8%) who had progressively worsening vision.12 One patient lost vision from phthisis; three patients lost vision from progression of glaucoma.12 Similarly, Zerbe et al. reported that in 62 eyes with at least 1 year follow-up (average, 14.5 months; range, 12–27 months), 12.9% (eight eyes) had decreased vision at the final follow-up visit, compared to 1 month postoperatively.7 The reasons cited for vision loss included end-stage glaucoma, retinal detachment, and age-related macular degeneration.7
Long-Term Outcomes of the Boston Type 1 Keratoprosthesis
An analysis of the long-term outcomes of the Boston KPro suggests the need for continued research and development in this field of keratoprosthesis surgery. Table 52.2 summarizes the KPro outcomes from the published literature.
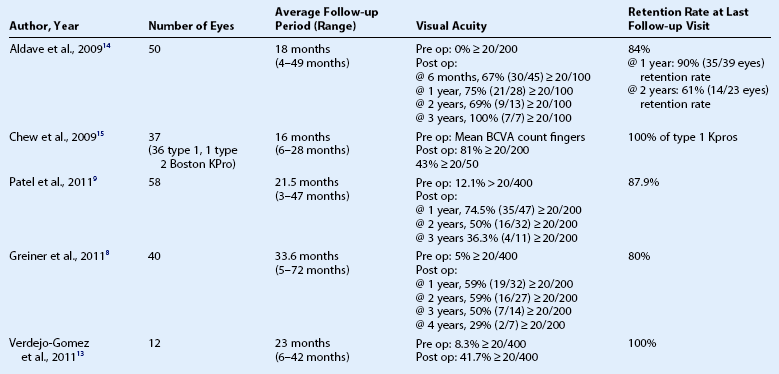
For the most part, outcomes remain positive for the first 2 to 3 years after keratoprosthesis surgery.13–15 Aldave et al. reviewed a series of 57 keratoprosthesis surgeries that were performed in 50 eyes. Seventy-nine percent (38/48 eyes) had improved vision at the final postoperative visit, compared with preoperative vision.14 They found it encouraging that the percentage of eyes with a visual acuity of 20/200 or better increased over time.14 Of the eight eyes with at least 3 year follow-up data, all eight eyes (100%) had a visual acuity of 20/200 or better.14 The authors speculate that many of the complications of keratoprosthesis surgery which affect vision, such as retroprosthetic membrane formation, cystoid macular edema and posterior capsular opacification, appear and are managed in the first postoperative year, allowing for better vision later in the postoperative course.14 These are by far the best results reported in the literature to date. However, despite these encouraging results, long-term retention of the keratoprosthesis shows a downward trend with a 90% retention rate (35/39) at 1 year decreasing to 61% (14/23) at 2 years.14
Chew et al. also demonstrated an overall improvement of visual acuity in their patients with an improvement from a preoperative mean best-corrected visual acuity (BCVA) of count fingers to a mean best BCVA at any point postoperatively of 20/50.15 However, even during the follow-up period ranging from 6 to 28 months, 25% patients did not maintain their best postoperative visual acuity, and the mean BCVA at the final follow-up visit for these patients was 20/90.15 The most common causes of vision loss after keratoprosthesis surgery in this series were progression of glaucoma and endophthalmitis.15
Concerns regarding long-term visual acuity loss and late complications are echoed in studies of KPro patients from the New York Eye and Ear Infirmary and the University of California, Davis.8,9 Patel et al. observed a trend of worsening visual acuity over time.9 At the last follow-up, 43.1% of eyes had attained a BCVA ≥ 20/200 and 55.2% of eyes had improved vision, compared to preoperative vision.9 This is comparable to the study by Zerbe et al. but worse than what Aldave et al. had reported.7,14 However, over time, the percentage of eyes with BCVA ≥ 20/200 visual acuity decreased from 74.5% (35/47) at 1 year, 50.0% (16/32)at 2 years and 36.3% (4/11) at 3 years.9 Additionally, the incidence of complications increased with time; 19.0% of eyes had at least one adverse event by 1 month, 65.5% by 6 months, and 75.9% by 1 year.
Greiner et al. reported very similar results with visual acuity worsening over time.8 Although 89% of eyes achieved a BCVA ≥ 20/200 at some point during the postoperative period, only 59% retained this level of vision at 1 year and 2 years postoperatively, 50% at 3 years, and only 29% at 4 years postoperatively.8 They found that the most common cause for progressive vision loss was progression of glaucoma.8 Other causes for vision loss included retroprosthetic membranes, endophthalmitis, and recurrent corneal melts with KPro extrusion.8
Preoperative diagnosis may provide prognostic indications of ultimate postoperative outcomes.16 In the next section, we will review outcomes for individual indications for Boston keratoprosthesis placement.
Aniridia and Keratoprosthesis Surgery
Congenital aniridia is a bilateral, panocular disease which may affect cornea, iris, lens, macula and optic nerve. These patients develop a limbal stem cell deficiency which may lead to conjunctivalization, vascularization and opacification of the cornea, requiring limbal stem cell transplantation and corneal transplantation.17,18
In the study by Akpek et al., 16 eyes in 15 patients with aniridia underwent Boston type I keratoprosthesis surgery.19 Visual acuity improved in 15 patients and was maintained in 14 patients at their last follow-up visit.19 Postoperative visual acuity ranged from 20/60 to hand motions (median 20/200), compared to preoperative visual acuities which ranged from 20/300 to light perception (median count fingers).19 Postoperative visual acuity was limited by factors related to the underlying congenital aniridia, such as foveal hypoplasia, optic nerve hypoplasia, nystagmus and glaucomatous optic nerve damage.19 Postoperative complications did occur in several patients, including three patients with choroidal detachments of which one progressed to retinal detachment, hypotony and vision loss.19 All devices were retained at the last follow-up visit for the study (range 2–85 months, median 17 months), but there was one case of a tissue melt requiring a scleral patch graft.19
Bakhtiari et al. describe nine cases of Boston type I keratoprosthesis surgery in eyes with aniridic fibrosis syndrome, a condition in which progressive anterior chamber fibrosis occurs in a patient with congenital aniridia who had had multiple intraocular surgeries.20 After keratoprosthesis surgery, vision improved in all eyes, ranging from hand motions to count fingers preoperatively to 20/200 to 20/500 postoperatively.20 Successful outcomes in these challenging cases were achieved with intraocular lens explantation, removal of the fibrotic membrane and placement of a Boston KPro.20
Autoimmune Disease, Corneal Limbal Stem Cell Deficiency and Keratoprosthesis Surgery
Autoimmune diseases affecting the ocular surface and leading to corneal opacification present a significant challenge for the corneal surgeon. Patients with diseases, such as Stevens–Johnson syndrome (SJS), toxic epidermal necrolysis syndrome (TENS), and mucous membrane pemphigoid (MMP) frequently have corneal limbal stem cell deficiency or tear dysfunction resulting in failure with traditional corneal transplantation. Similarly, corneal limbal stem cell deficiency in the setting of chemical injuries may render traditional penetrating keratoplasty ineffective. The Boston keratoprosthesis has been used as an alternative in these difficult cases.21–23
Unfortunately, in these patients, the prognosis for keratoprosthesis surgery is extremely guarded.16 In an early study from Massachusetts Eye and Ear Infirmary, keratoprosthesis surgery in SJS patients had the worst visual outcome with no eyes retaining 20/200 vision or better at 5 years.16 Postoperative complications requiring operative repair was also far higher in the SJS group of patients with 71% requiring some type of postoperative surgical intervention.16 Non-cicatricial diseases had the most favorable prognosis with MMP and chemical burns, falling into a middle prognostic category.16 Sixty-four percent of eyes of chemical burns and 43% of eyes with MMP had 20/200 vision or better at 5 years.16
Subsequent retrospective case reviews have supported these initial observations by Yaghouti et al.16 Despite improvements in design and management of the Boston keratoprosthesis with use of vancomycin prophylaxis, chronic soft contact lens use and holes in the back plate of the keratoprosthesis,2–6 SJS continues to have a less favorable outcome with the device than in patients with non-autoimmune diseases. In 15 patients with SJS who underwent KPro surgery (both type I and type II KPro) between 2000 and 2005, seven eyes (44%) retained 20/70 vision or better postoperatively.21 Five eyes that had initial improvement of vision postoperatively had subsequent deterioration of vision long term, with four of these five eyes ultimately losing light perception.21 In this series of patients, however, there were no cases of KPro extrusion.21 Four eyes (25%) did develop tissue melt and aqueous leakage.21
Sejpal et al. reviewed 23 eyes in 22 patients with limbal stem cell deficiency, including seven eyes (30.4%) with chemical injury, six eyes (26.1%) with SJS, and one eye (4.3%) with OCP.23 Seven keratoprostheses were removed over the duration of the postoperative follow-up period.23 Five of seven were removed in patients with SJS, one was removed in a patient with OCP and one from a patient with a chemical injury.23 Visual acuity results in this case series were more favorable than in other series with similar patient populations, with improvement of corrected distance visual acuity in 19 of 21 (90.5%) eyes with a retained keratoprosthesis at the final follow-up visit.23 The most common postoperative complication in these patients was persistent epithelial defect, which was a risk factor for infectious keratitis.23 Persistent epithelial defects were found to be significantly more common in these eyes with limbal stem cell deficiency than in those without (56.5% versus 23.2%, p = 0.008).23
Finally, in a sobering reminder of the challenges of managing patients with autoimmune disease affecting the cornea, Ciralsky et al described two patients, one with TEN and the other with MMP, who both required multiple repeat Boston keratoprosthesis implantations, due to recurrent corneal melts.22
The outcomes for keratoprosthesis surgery in patients with autoimmune disease and, in particular, Stevens–Johnson syndrome and toxic epidermal necrolysis, is extremely guarded. An improved understanding of the pathogenesis of these diseases and the immune response after keratoprosthesis implantation may ultimately help to target appropriate immunomodulating therapies to better the outcomes in these patients.22
Pediatric Keratoprosthesis
Pediatric corneal opacities are a particularly challenging situation for the corneal surgeon. Penetrating keratoplasty surgery in the pediatric population is associated with a higher rate of graft rejection, complications and failure.24,25 A review of the literature on keratoprosthesis surgery in children is relatively sparse with only a few scattered case reports and one retrospective review.26,27 In their retrospective review of 21 cases of Boston keratoprosthesis placement in children ranging from 1.5 months of age to 136 months of age, Aquavella et al. had no intraoperative complications.27 All keratoprostheses were retained for the duration of their follow-up period (range 1–30 months).27 Postoperative complications included five cases of retroprosthetic membrane formation requiring intervention and two cases of hypotony with glaucoma drainage device and subsequent retinal detachment in each case.27 In the seven eyes in which visual acuity could be measured, visual acuity ranged from 20/30 to light perception.27 The remaining eyes in pre-verbal children demonstrated fix and follow vision.27
There are theoretical advantages of keratoprosthesis surgery in children, including rapid postoperative recovery with a stable refraction and a clear visual axis. These conditions allow for more rapid visual rehabilitation and amblyopia management without the risk of allograft rejection.28 It has also been observed that placement of a Boston KPro in children causes less photophobia, epiphora, and blepharospasm than traditional penetrating keratoplasty.28 Similar postoperative complications can be expected in children undergoing keratoprosthesis surgery as in adults and will likely affect the long-term outcomes in these children.
Graft Failures and Keratoprosthesis Surgery
Surgical outcomes in patients with non-cicatrizing ocular surface conditions carry the best prognosis after keratoprosthesis surgery.16 These are patients who have failed traditional penetrating keratoplasty and have underlying diseases ranging from corneal dystrophies or degenerations to bacterial and viral keratitis. They tend to have a better visual outcome at 5 years and are less likely to lose best-corrected visual acuity of 20/200 or better after surgery.16
Patients who are at particularly high risk of corneal allograft failure are those with underlying herpes simplex keratitis.29,30 In a series of 17 failed traditional penetrating keratoplasties in 14 patients with underlying herpetic keratitis, the outcomes were quite favorable after placement of a Boston keratoprosthesis.31 The authors found that 15 eyes (88%) achieved a best-corrected visual acuity between 20/25 and 20/70 during the postoperative period, and 11 eyes (73%) were able to maintain that level of visual acuity at the last follow-up visit (median, 17 months; range 6–72 months).31 There were no device extrusions observed during the follow-up period.31
The Boston keratoprosthesis may be a very viable option for patients who have failed prior penetrating keratoplasty for these non-cicatrizing corneal diseases. Given the increased risk of graft failure with each subsequent regraft and the decreased time of survival of each subsequent regraft, the Boston keratoprosthesis should be considered in patients motivated to obtain visual rehabilitation.32
Other Indications for Boston Keratoprosthesis Surgery and Outcomes
The Boston type I keratoprosthesis has been used successfully for a wide variety of indications, including herpes zoster neurotrophic keratopathy,33 severe vernal keratoconjuncitvitis,34 Mooren’s ulcer,34 and ocular trauma.35 These case reports demonstrate both successful anatomic outcomes and improved visual function after keratoprosthesis surgery in patients with an otherwise poor prognosis for standard penetrating keratoplasty.
References
1. Klufas, MA, Colby, KA. The Boston keratoprosthesis. Int Ophthalmol Clin. 2010;50:161–175.
2. Harissi-Dagher, M, Khan, BF, Schaumberg, DA, et al. Importance of nutrition to corneal grafts when used as a carrier of the Boston keratoprosthesis. Cornea. 2007;26:564–568.
3. Dohlman, C, Harissi-Dagher, M. The Boston keratoprosthesis: a new threadless design. Digital J Ophthalmol. 13, 2007.
4. Khan, BF, Harissi-Dagher, M, Khan, DM, et al. Advances in Boston keratoprosthesis: enhancing retention and prevention of infection and inflammation. Int Ophthalmol Clin. 2007;47:61–71.
5. Dohlman, CH, Dudenhoefer, EJ, Khan, BF, et al. Protection of the ocular surface after keratoprosthesis surgery: the role of soft contact lenses. CLAO J. 2002;28:72–74.
6. Durand, ML, Dohlman, CH. Successful prevention of bacterial endophthalmitis in eyes with the Boston keratoprosthesis. Cornea. 2009;28:896–901.
7. Zerbe, BL, Belin, MW, Ciolino, JB, et al. Results from the multicenter Boston type 1 keratoprosthesis study. Ophthalmology. 2006;113:1779–1784.
8. Greiner, MA, Li, JY, Mannis, MJ. Longer-term vision outcomes and complications with the Boston type 1 keratoprosthesis at the University of California, Davis. Ophthalmology. 2011;118:1543–1550.
9. Patel, AP, Wu, EI, Ritterband, DC, et al. Boston type 1 keratoprosthesis: the New York Eye and Ear experience. Eye. 2012;26:418–425.
10. Todani, A, Ciolino, JB, Ament, JD, et al. Titanium back plate for a PMMA keratoprosthesis: clinical outcomes. Graefes Arch Clin Exp Ophthalmol. 2011;249:1515–1518.
11. Dunlap, K, Chak, G, Aquavella, JV, et al. Short-term visual outcomes of Boston type 1 keratoprosthesis implantation. Ophthalmology. 2010;117:687–692.
12. Robert, MC, Harissi-Dagher, M. Boston type 1 keratoprosthesis: the CHUM experience. Can J Ophthalmol. 2011;46:164–168.
13. Verdejo-Gónez, L, Peláez, N, Gris, O, et al. The Boston type I keratoprosthesis: an assessment of its efficacy and safety. Ophthalmic Surg Lasers Imaging. 2011;42:446–452.
14. Aldave, AJ, Kamal, KM, Vo, RC, et al. The Boston type I keratoprosthesis: improving outcomes and expanding indications. Ophthalmology. 2009;116:640–651.
15. Chew, HF, Ayres, BD, Hammmersmith, KM, et al. Boston keratoprosthesis outcomes and complications. Cornea. 2009;28:989–996.
16. Yaghouti, F, Nouri, M, Abad, JC, et al. Keratoprosthesis: preoperative prognostic categories. Cornea. 2001;20:19–23.
17. Ramaesh, K, Ramaesh, T, Dutton, GN, et al. Evolving concepts on the pathogenic mechanisms of aniridia related keratopathy. Int J Biochem Cell Biol. 2005;37:547–557.
18. Holland, EJ, Djalilian, AR, Schwartz, GS. Management of aniridic keratopathy with keratolimbal allograft: a limbal stem cell transplantation technique. Ophthalmology. 2003;110:125–130.
19. Akpek, EK, Harissi-Dagher, M, Petrarca, R, et al. Outcomes of Boston keratoprosthesis in aniridia: a retrospective multicenter study. Am J Ophthalmol. 2007;144:227–231.
20. Bahktiari, P, Chan, C, Welder, JD, et al. Surgical and visual outcomes of the type I Boston keratoprosthesis for the management of aniridic fibrosis syndrome in congential aniridia. Am J Ophthalmol. 2009;153:967–971.
21. Sayegh, RR, Ang, LPK, Foster, CS, et al. The Boston keratoprosthesis in Stevens–Johnson syndrome. Am J Ophthalmol. 2008;145:438–444.
22. Ciralsky, J, Papaliodis, GN, Foster, CS, et al. Keratoprosthesis in autoimmune disease. Ocul Immunol Inflamm. 2010;18:275–280.
23. Sejpal, K, Yu, F, Aldave, AJ. The Boston keratoprosthesis in the management of corneal limbal stem cell deficiency. Cornea. 2011;30:1187–1194.
24. Dana, MR, Moyes, AL, Gomes, JA, et al. The indications for and outcome in pediatric keratoplasty. A multicenter study. Ophthalmology. 1995;102:1129–1138.
25. Huang, C, O’Hara, M, Mannis, MJ. Primary pediatric keratoplasty: indications and outcomes. Cornea. 2009;28:1003–1008.
26. Botelho, PJ, Congdon, NG, Handa, JT, et al. Keratoprosthesis in high-risk pediatric corneal transplantation: first 2 cases. Arch Ophthalmol. 2006;124:1356–1357.
27. Aquavella, JV, Gearinger, MD, Akpek, EK, et al. Pediatric keratoprosthesis. Ophthalmology. 2007;114:989–994.
28. Nallasamy, S, Colby, K. Keratoprosthesis: procedure of choice for corneal opacities in children? Semin Ophthalmol. 2010;25:244–248.
29. Epstein, RJ, Seedor, JA, Dreizen, NG, et al. Penetrating keratoplasty for herpes simplex keratitis and keratoconus. Allograft rejection and survival. Ophthalmology. 1987;94:935–944.
30. Ficker, LA, Kirkness, CM, Rice, NS, et al. The changing management and improved prognosis for corneal grafting in herpes simplex keratitis. Ophthalmology. 1989;96:1587–1596.
31. Kahn, BF, Harissi-Dagher, M, Pavan-Langston, D, et al. The Boston keratoprosthesis in herpetic keratitis. Arch Ophthalmol. 2007;125:745–749.
32. Bersudsky, V, Blum-Hareuveni, T, Rehany, U, et al. The profile of repeated corneal transplantation. Ophthalmology. 2001;108:461–469.
33. Pavan-Langston, D, Dohlman, CH. Boston keratoprosthesis treatment of herpes zoster neurotrophic keratopathy. Ophthalmology. 2008;115(Suppl. 2):S21–S23.
34. Basu, S, Taneja, M, Sangwan, VS. Boston type 1 keratoprosthesis for severe blinding vernal keratoconjunctivitis and Mooren’s ulcer. Int Ophthalmol. 2011;31:219–222.
35. Harissi-Dagher, M, Dohlman, CH. The Boston keratoprosthesis in severe ocular trauma. Can J Ophthalmol. 2008;43:165–169.
[/level-membership-for-opthalmology-category][not-level-membership-for-opthalmology-category]52
Boston Keratoprosthesis Outcomes
Introduction
The Boston Keratoprosthesis™ (Boston KPro) was developed at the Massachusetts Eye and Ear Infirmary for the treatment of corneal blindness in patients who otherwise have a poor prognosis for a standard penetrating keratoplasty (PKP). Since its approval by the FDA in 1992, the Boston KPro has become the most commonly used keratoprosthesis device in the United States. Over 3500 Boston keratoprosthesis devices have been implanted worldwide, with the vast majority having been implanted since 2006.1
Advances in the Boston Keratoprosthesis to Improve Outcomes
Several advances in both the design of the Boston type I keratoprosthesis and in our understanding of the postoperative management of these patients have led to improved outcomes and contributed to the popularity of the surgery.1 Major postoperative complications, such as corneal melting, keratoprosthesis extrusion, and endophthalmitis can lead to removal of the keratoprosthesis and significant vision loss. However, even retroprosthetic membranes, which are the most common postoperative complications after keratoprosthesis surgery, may lead to vision decline.
Current design features of the Boston keratoprosthesis that have helped to improve retention of the KPro include holes in the back plate of the KPro, a threadless design, and a titanium locking ring.2–4 The holes in the back plate of the KPro allow nutrients, such as glucose to pass from the aqueous to the corneal carrier tissue.2 An early study showed a statistically significant decrease in tissue necrosis or melt around a keratoprosthesis from 51% of eyes with a solid PMMA back plate to 10% of eyes of eyes with a back plate with holes.2 The threadless design of the stem of the KPro prevents misthreading or inadequate threading of the back plate, a design that previously led to gaps between the front plate and the cornea carrier tissue and resulting anterior protrusion of the front.3 Anterior protrusion of the KPro was associated with tissue melting around the stem.3 The titanium locking ring helps prevent intraocular loosening of the KPro postoperatively.4
Postoperatively, the use of a bandage contact lens and long-term vancomycin drops has been instrumental to reducing vision-threatening complications of keratoprosthesis surgery. Bandage contact lenses improve outcomes by decreasing the risk of corneal melting from desiccation of the ocular surface.5
Long-term topical vancomycin eye drops (14 mg/mL) help decrease the risk of bacterial endophthalmitis.6 Bacterial endophthalmitis is a devastating complication associated with a very poor visual outcome.6 In their retrospective review of bacterial endophthalmitis in KPro eyes between 1990 and 2006, Durand and Dohlman. found that only two of 18 eyes regained useful vision.6 Eight of 18 eyes in their review lost light perception vision entirely, with five eyes retaining only hand motions or light reception vision.6 Fortunately, they also found a statistically significant lower incidence of bacterial endophthalmitis in patients on topical vancomycin prophylaxis, compared with those on a single commercially available antibiotic agent alone (0.35% versus 4.13% per patient-year, p = 0.001).6 Keratoprosthesis surgeons now routinely use topical vancomycin in combination with another commercially available broad-spectrum antibiotic agent, although the precise regimen varies among surgeons.1
Finally, decreasing the frequency of retroprosthetic membrane formation may also help improve long-term visual outcomes after KPro surgery. Although visually significant retroprosthetic membranes can typically be treated with a simple YAG membranotomy, some membranes may be refractory to laser treatment, causing a decline in vision and necessitating more aggressive surgical removal.7–9 In some instances, the retroprosthetic membrane may be recalcitrant even to surgical removal.9 A titanium back plate for the Boston keratoprosthesis is currently being evaluated at the Massachusetts Eye and Ear Infirmary. The preliminary findings are encouraging, with a trend towards decreased postoperative inflammation and less frequent formation of retroprosthetic membranes in patients with a titanium back plate.10
Early Postoperative Outcomes of the Boston Type 1 Keratoprosthesis
Early postoperative outcomes for the Boston type 1 keratoprosthesis are generally excellent. Table 52.1 highlights studies looking at shorter-term outcomes (average follow-up period < 12 months). Within the first few months after surgery, visual improvement is often drastic. Dunlap et al. reported short-term visual outcomes of the Boston type I keratoprosthesis and found that in their series of 126 eyes, 82.5% (104 eyes) had improved visual acuity within the first 6 months.11 Of those 104 eyes, 31 eyes (30%) achieved best-corrected vision within 1 week of surgery.11 By postoperative month 1, 59 eyes (54%) had achieved their best-corrected visual acuity.11 The 22 eyes which did not have an improvement in visual acuity postoperatively had co-morbid conditions limiting visual potential.11
Robert and Harissi-Dagher reported similar outcomes in their patients.12 In a group of 47 eyes, they observed that 84% had an improvement of best-corrected visual acuity, with the median visual acuity improving from hand motions preoperatively to 20/150 by postoperative month 3.12 There was 100% anatomic retention of the keratoprosthesis in these patients.12
Zerbe et al. also reported positive outcomes in the United States multicenter study.7 Postoperatively, 57% of eyes had a best-corrected vision of 20/200 or better, compared to just 3.6% preoperatively.7 There was a 95% rate of KPro retention in this study.7
Interestingly, even in their relatively short follow-up period (average, 10 months; range, 3–18.5 months), Robert and Harissi-Dagher had four patients (8%) who had progressively worsening vision.12 One patient lost vision from phthisis; three patients lost vision from progression of glaucoma.12 Similarly, Zerbe et al. reported that in 62 eyes with at least 1 year follow-up (average, 14.5 months; range, 12–27 months), 12.9% (eight eyes) had decreased vision at the final follow-up visit, compared to 1 month postoperatively.7 The reasons cited for vision loss included end-stage glaucoma, retinal detachment, and age-related macular degeneration.7
Long-Term Outcomes of the Boston Type 1 Keratoprosthesis
An analysis of the long-term outcomes of the Boston KPro suggests the need for continued research and development in this field of keratoprosthesis surgery. Table 52.2 summarizes the KPro outcomes from the published literature.
For the most part, outcomes remain positive for the first 2 to 3 years after keratoprosthesis surgery.13–15 Aldave et al. reviewed a series of 57 keratoprosthesis surgeries that were performed in 50 eyes. Seventy-nine percent (38/48 eyes) had improved vision at the final postoperative visit, compared with preoperative vision.14 They found it encouraging that the percentage of eyes with a visual acuity of 20/200 or better increased over time.14 Of the eight eyes with at least 3 year follow-up data, all eight eyes (100%) had a visual acuity of 20/200 or better.14 The authors speculate that many of the complications of keratoprosthesis surgery which affect vision, such as retroprosthetic membrane formation, cystoid macular edema and posterior capsular opacification, appear and are managed in the first postoperative year, allowing for better vision later in the postoperative course.14 These are by far the best results reported in the literature to date. However, despite these encouraging results, long-term retention of the keratoprosthesis shows a downward trend with a 90% retention rate (35/39) at 1 year decreasing to 61% (14/23) at 2 years.14
[/not-level-membership-for-opthalmology-category]
