[level-membership-for-orthopaedics-category]
Chapter 4C Bone Marrow Stimulating Techniques
Autologous Matrix-Induced Chondrogenesis (AMIC)
Introduction
Chondral and osteochondral defects may affect any major joint, but they more often affect the large weight-bearing joints such as the knee and ankle joints. They may be of traumatic or hereditary origin (osteochondrosis dissecans). The original hyaline cartilage may as yet not be restored, so a permanent loss of the original cartilaginous surface is inevitable and responsible for premature arthritis and eventually destruction of the affected joint. However, a stable fibrous cartilage may develop from mesenchymal stem cells invading the defects from the underlying blood vessels, which will yield the patient pain free and slow down the process of joint destruction. Several methods in cartilage reconstruction are available such as ACT/ACI (autologous chondrocyte transplantation/implantation),1 matrix-induced autologous chondrocyte transplantation/implantation (MACT/MACI)2,3,4,5,6 and microfracturing. The membrane-associated chondrogenesis is well documented in vitro. A variety of collagen scaffolds is commercially available and may be applied. Fixation is possible either with fibrin glue (allogenic or partially autologous) or sutures.
An advantage of the autologous matrix-induced chondrogenesis (AMIC) procedure is that it is a one-step process for the patient, allowing the blood clot yielded after microfracturing to stay at the desired location and the chondrocytes to develop on a collagen scaffold in situ. Any collagen matrix will suffice.
Surgical Principles and Objective
Step 2: Miniarthrotomy
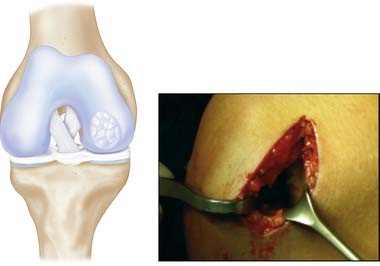
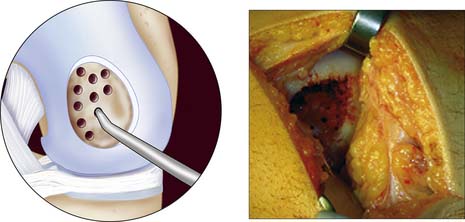
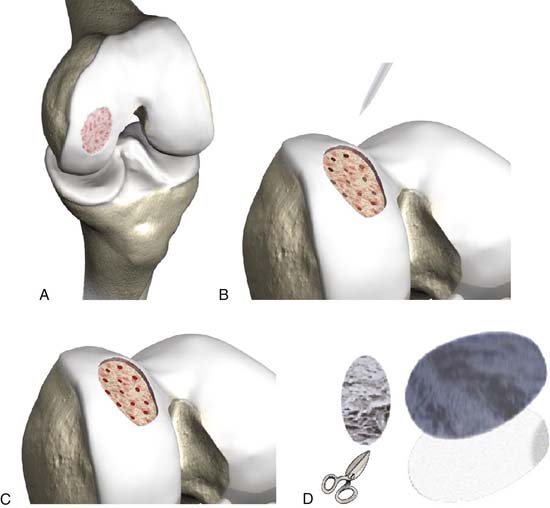
Debridement of lesion: degenerated and detached cartilage is completely removed, microfracturing with a sharp awl or pick, and, if necessary, a mallet to perforate the subchondral bone every 5 mm; a template is made that matches the size of the defect, not overlaying the defect (Figs. 4C-1, 4C-2, and 4C-3).

Step 4
In the meantime, a 10-ml blood sample is taken from the patient; derive the serum by centrifugation (using a hand centrifuge) or allow it to settle, discard 50% of the thrombin of the commercially available fibrin glue (double syringe system: one syringe is thrombin and the other is fibrinogen, for example Tissucol/Tisseel, Baxter Biosciences, Vienna, Austria), replace it with the autologous serum, and mix it so you get the partial autologous fibrin glue (PAF).
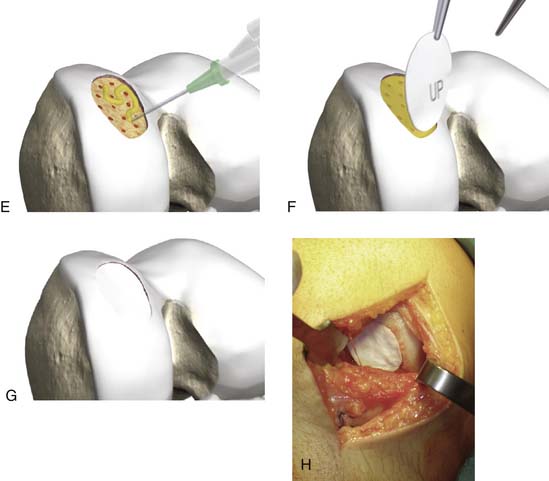
Step 5: Fixation of Matrix with PAF
The matrix is glued directly onto the prepared defect and is adjusted digitally. Finally the knee joint is held in an extended position for 5 minutes (Fig. 4C-4, A-H).
Afterward, flex the knee 10 times to test the stability and correct position.
Step 6
If necessary, add autologous bone graft to build up the defect to the level of the original surrounded bone (e.g., osteochondral defect).
Postoperative Treatment
Surgical Instruments
Postoperative Treatment
1. Brittberg M. Articulate cartilage repair in the knee joint with autologous chondrocytes and periosteal graft. Operat Orthop Traumatol. 2001;13:198-207.
2. Behrens P, Benthien JP. Autologous matrix-induced chondrogenesis (AMIC): a one-step procedure for retropatellar resurfacing. Acta Orthop Belgica 2010 Apr; 76(2):260-3.
3. Behrens P, Benthien JP. Autologous matrix-induced chondrogenesis (AMIC): combining microfracturing and a collagen I/III matrix for articular cartilage resurfacing. Cartilage 2010; I(1)65-68.
4. Behrens P., Bosch U., Bruns J., Erggelet C., Esenwein S.A., Gaissmaier C., Krackhardt T., Löhnert J., Marlovits S., Meenen N.M., Mollenhauer J., Nehrer S., Niethard F.U., Nöth U., Perka C., Richter W., Schäfer D., Schneider U., Steinwaschs M., Weise K. German Society for Traumatology; German Society for Orthopedic Surgery. Indications and implementation of recommendations of the working group “Tissue Regeneration and Tissue Substitutes” for autologous chondrocyte transplantation (ACT). Z Orthop Ihre Grenzgeb. 2004 Sep-Oct;142(5):529-539. Review. German
5. Behrens P., Bitter T., Kurz B., Russlies M. Matrix-associated autologous chondrocyte transplantation/implantation (MACT/MACI)–5-year follow-up. Knee. 2006 Jun;13(3):194-202. Epub 2006 Apr 24
6. Anders S., Schaumburger J., Schubert T., Grifka J., Behrens P. Matrix-associated autologous chondrocyte transplantation (MACT). Minimally invasive technique in the knee. Oper Orthop Traumatol. 2008 Sep;20(3):208-219. German
7. Skodacek D., Brandau S., Deutschle T., Lang S., Rotter N. Growth factors and scaffold composition influence properties of tissue engineered human septal cartilage implants in a murine model. Int J Immunopathol Pharmacol. 2008 Oct-Dec;21(4):807-816.
8. Gille J., Schuseil E., Wimmer J., Gellissen J., Schulz A.P., Behrens P. Mid-term results of autologous matrix-induced chondrogenesis for treatment of focal cartilage defects in the Knee. Knee Surg Sports Traumatol Arthrosc. 2010 Feb 2. Epub
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
Chapter 4C Bone Marrow Stimulating Techniques
Autologous Matrix-Induced Chondrogenesis (AMIC)
Introduction
Chondral and osteochondral defects may affect any major joint, but they more often affect the large weight-bearing joints such as the knee and ankle joints. They may be of traumatic or hereditary origin (osteochondrosis dissecans). The original hyaline cartilage may as yet not be restored, so a permanent loss of the original cartilaginous surface is inevitable and responsible for premature arthritis and eventually destruction of the affected joint. However, a stable fibrous cartilage may develop from mesenchymal stem cells invading the defects from the underlying blood vessels, which will yield the patient pain free and slow down the process of joint destruction. Several methods in cartilage reconstruction are available such as ACT/ACI (autologous chondrocyte transplantation/implantation),1 matrix-induced autologous chondrocyte transplantation/implantation (MACT/MACI)2,3,4,5,6 and microfracturing. The membrane-associated chondrogenesis is well documented in vitro. A variety of collagen scaffolds is commercially available and may be applied. Fixation is possible either with fibrin glue (allogenic or partially autologous) or sutures.
An advantage of the autologous matrix-induced chondrogenesis (AMIC) procedure is that it is a one-step process for the patient, allowing the blood clot yielded after microfracturing to stay at the desired location and the chondrocytes to develop on a collagen scaffold in situ. Any collagen matrix will suffice.
Surgical Principles and Objective
Step 2: Miniarthrotomy
Debridement of lesion: degenerated and detached cartilage is completely removed, microfracturing with a sharp awl or pick, and, if necessary, a mallet to perforate the subchondral bone every 5 mm; a template is made that matches the size of the defect, not overlaying the defect (Figs. 4C-1, 4C-2, and 4C-3).
Step 4
In the meantime, a 10-ml blood sample is taken from the patient; derive the serum by centrifugation (using a hand centrifuge) or allow it to settle, discard 50% of the thrombin of the commercially available fibrin glue (double syringe system: one syringe is thrombin and the other is fibrinogen, for example Tissucol/Tisseel, Baxter Biosciences, Vienna, Austria), replace it with the autologous serum, and mix it so you get the partial autologous fibrin glue (PAF).
Step 5: Fixation of Matrix with PAF
The matrix is glued directly onto the prepared defect and is adjusted digitally. Finally the knee joint is held in an extended position for 5 minutes (Fig. 4C-4, A-H).
[/not-level-membership-for-orthopaedics-category]
