[level-membership-for-radiology-category] Usually from left side of distal thoracic esophagus
• Chest film
Left side pleural effusion or hydropneumothorax
Radiolucent streaks of gas along aorta or in neck
• Esophagography with nonionic, water-soluble contrast agent
Shows extravasation of ingested or injected (through nasogastric tube) contrast medium
From left side of esophagus, just above gastroesophageal (GE) junction
If initial study with water-soluble contrast medium fails to show leak, examination must be repeated immediately with barium to detect subtle leaks
• CT
Extraluminal gas &/or oral contrast medium in lower mediastinum &/or upper abdomen
TOP DIFFERENTIAL DIAGNOSES
• Mallory-Weiss syndrome
• Pulsion diverticulum (epiphrenic)
• Iatrogenic (postinstrumentation) injury
CLINICAL ISSUES
• Accounts for 15% of total esophageal perforation cases
• Prognosis for large perforation
After 24 hours without treatment: Mortality = 70%
After immediate surgical drainage: Good
• Treatment
Drains in esophagus, mediastinum, pleural space, &/or abdomen
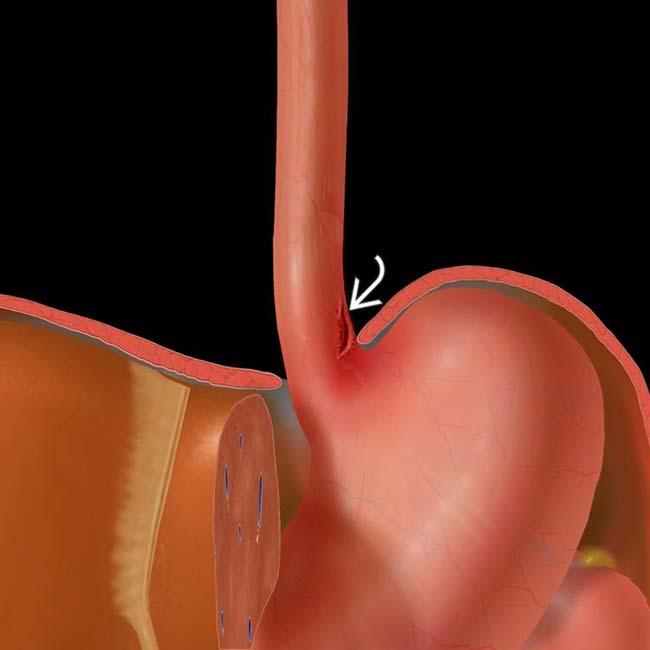
(Left) Graphic shows a vertically oriented laceration of the distal esophagus, just above the hiatus and gastroesophageal (GE) junction.
(Right) Film from an esophagram following injection of a water-soluble contrast medium through a nasogastric tube demonstrates a leak of contrast medium from a tear in the left anterior wall of the distal esophagus , a classic appearance for Boerhaave syndrome.
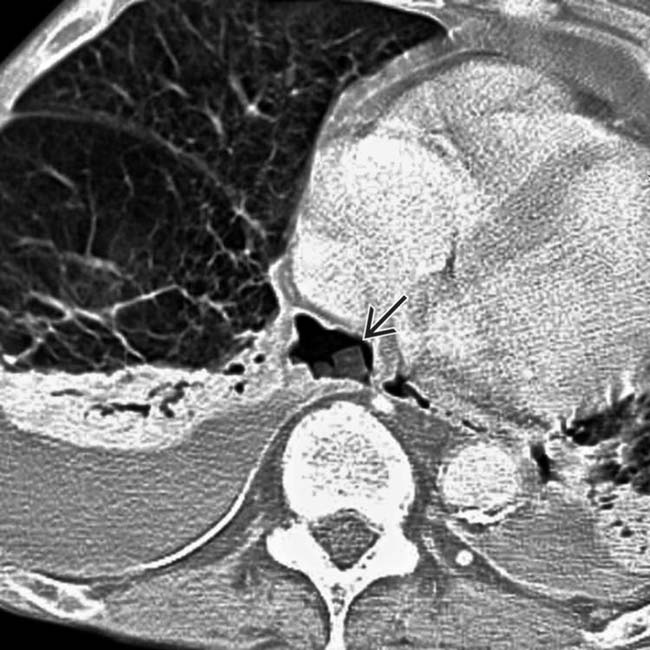
(Left) Axial CECT in a middle-aged man with severe chest pain after repeated retching shows extraluminal gas and contrast material surrounding the esophagus in the lower mediastinum and upper abdomen.
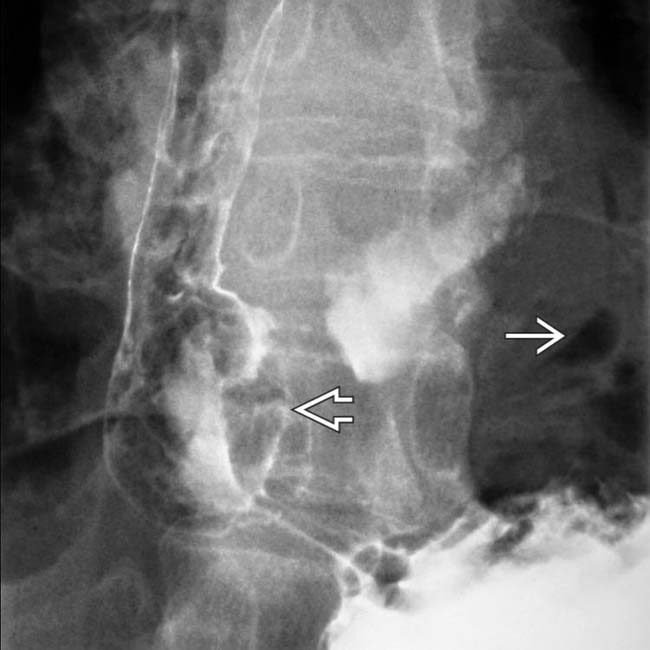
(Right) Film from a fluoroscopic exam in the same patient during injection of water-soluble contrast through a nasogastric tube shows extraluminal contrast in the mediastinum and upper abdomen . The site of the tear is the left anterior wall of the distal esophagus.
TERMINOLOGY
Definitions
• Spontaneous distal esophageal perforation following vomiting or other violent straining
IMAGING
General Features
• Best diagnostic clue
Extraluminal gas and contrast material in lower mediastinum surrounding esophagus
• Other general features
Sudden increase in intraluminal pressure leads to full-thickness esophageal perforation
Left side of distal thoracic esophagus
– Most vulnerable (due to lack of supporting mediastinal structures)
– Vertical, full-thickness tear, 1-4 cm long
Rarely from cervical or upper thoracic esophagus
– Mortality rate < 15% if treated promptly
Radiographic Findings
• Radiography
Chest radiograph
– Mediastinal widening, pneumomediastinum
– Left-side pleural effusion or hydropneumothorax
– Radiolucent streaks of gas along aorta or in neck
Abdominal radiograph
– Gas in retroperitoneum or intraperitoneal (rare)
Esophagography
– Shows extravasation of ingested or injected (through nasogastric [NG] tube) contrast medium
– From left side of esophagus, just above gastroesophageal (GE) junction
CT Findings
• Extraluminal gas &/or oral contrast medium in lower mediastinum &/or upper abdomen
• Plain chest radiograph; helical CECT with oral contrast
• Esophagography with nonionic water-soluble contrast agent
If initial study with water-soluble contrast medium fails to show leak, examination must be repeated immediately with barium to detect subtle leaks
DIFFERENTIAL DIAGNOSIS
Mallory-Weiss Syndrome
• Irregular linear mucosal tear or laceration in long axis of esophagus
Distal esophagus near GE junction or gastric cardia
Rarely detected on imaging studies
Pulsion Diverticulum (Epiphrenic)
• Mucosa-lined pouch from distal esophagus
• No free mediastinal gas or inflammation
Iatrogenic (Postinstrumentation) Injury
• Endoscopic procedures account for 75% of cases
Feeding or NG tubes can also perforate esophagus or esophageal diverticulum
• Location: Cervical (common), thoracic esophagus
• Indistinguishable from Boerhaave syndrome if distal esophagus is involved
PATHOLOGY
General Features
• Etiology
Rare causes
– Coughing, weightlifting, childbirth, defecation
– Seizures, status asthmaticus, blunt trauma
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
Classic triad
– Vomiting, severe substernal chest pain
– Subcutaneous emphysema of chest wall and neck
Rapid onset of overwhelming sepsis
– Fever, tachycardia, ↓ in blood pressure, shock
• Clinical profile
Patient with history of chronic alcoholism, severe vomiting, sudden severe substernal chest pain, and ↓ in blood pressure
Demographics
• Age
Usually adults
Natural History & Prognosis
• Prognosis
Large perforation
– After 24 hours without treatment: Mortality = 70%
– After immediate surgical drainage: Good
Treatment
• Large perforation
Immediate thoracotomy or thoracoscopy
Drains in esophagus, mediastinum, pleural space, &/or abdomen
• Small, self-contained perforation
Managed nonoperatively with broad spectrum antibiotics and parenteral alimentation
DIAGNOSTIC CHECKLIST
Consider
• Check for history of violent retching or vomiting
Esophagram shows irregular extraluminal contrast and gas dissecting through the mediastinum. Note the perforation of the distal esophagus . Immediate drainage was required.
Axial CECT shows bilateral pleural effusions containing high density that may be extravasated oral contrast medium or pleural calcification .
Axial CECT (lung window) shows food particles and gas in the mediastinum.
Esophagram shows an irregular collection of contrast material in the mediastinum and the source of perforation in the distal left side of the esophagus.
Esophagram shows a mediastinal collection of gas but no apparent leak of contrast material.
Axial CECT shows localized perforation of the distal left side of the esophagus with relatively mild periesophageal inflammatory changes.
Esophagram shows localized perforation of the distal left side of the esophagus.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Usually from left side of distal thoracic esophagus
• Chest film
Left side pleural effusion or hydropneumothorax
Radiolucent streaks of gas along aorta or in neck
• Esophagography with nonionic, water-soluble contrast agent
Shows extravasation of ingested or injected (through nasogastric tube) contrast medium
From left side of esophagus, just above gastroesophageal (GE) junction
If initial study with water-soluble contrast medium fails to show leak, examination must be repeated immediately with barium to detect subtle leaks
• CT
Extraluminal gas &/or oral contrast medium in lower mediastinum &/or upper abdomen
TOP DIFFERENTIAL DIAGNOSES
• Mallory-Weiss syndrome
• Pulsion diverticulum (epiphrenic)
• Iatrogenic (postinstrumentation) injury
CLINICAL ISSUES
• Accounts for 15% of total esophageal perforation cases
• Prognosis for large perforation
After 24 hours without treatment: Mortality = 70%
After immediate surgical drainage: Good
• Treatment
Drains in esophagus, mediastinum, pleural space, &/or abdomen
(Left) Graphic shows a vertically oriented laceration of the distal esophagus, just above the hiatus and gastroesophageal (GE) junction.
(Right) Film from an esophagram following injection of a water-soluble contrast medium through a nasogastric tube demonstrates a leak of contrast medium from a tear in the left anterior wall of the distal esophagus , a classic appearance for Boerhaave syndrome.
(Left) Axial CECT in a middle-aged man with severe chest pain after repeated retching shows extraluminal gas and contrast material surrounding the esophagus in the lower mediastinum and upper abdomen.
(Right) Film from a fluoroscopic exam in the same patient during injection of water-soluble contrast through a nasogastric tube shows extraluminal contrast in the mediastinum and upper abdomen . The site of the tear is the left anterior wall of the distal esophagus.
TERMINOLOGY
Definitions
• Spontaneous distal esophageal perforation following vomiting or other violent straining
IMAGING
General Features
• Best diagnostic clue
Extraluminal gas and contrast material in lower mediastinum surrounding esophagus
• Other general features
Sudden increase in intraluminal pressure leads to full-thickness esophageal perforation
Left side of distal thoracic esophagus
– Most vulnerable (due to lack of supporting mediastinal structures)
– Vertical, full-thickness tear, 1-4 cm long
Buy Membership for Radiology Category to continue reading. Learn more here









 of the distal esophagus, just above the hiatus and gastroesophageal (GE) junction.
of the distal esophagus, just above the hiatus and gastroesophageal (GE) junction.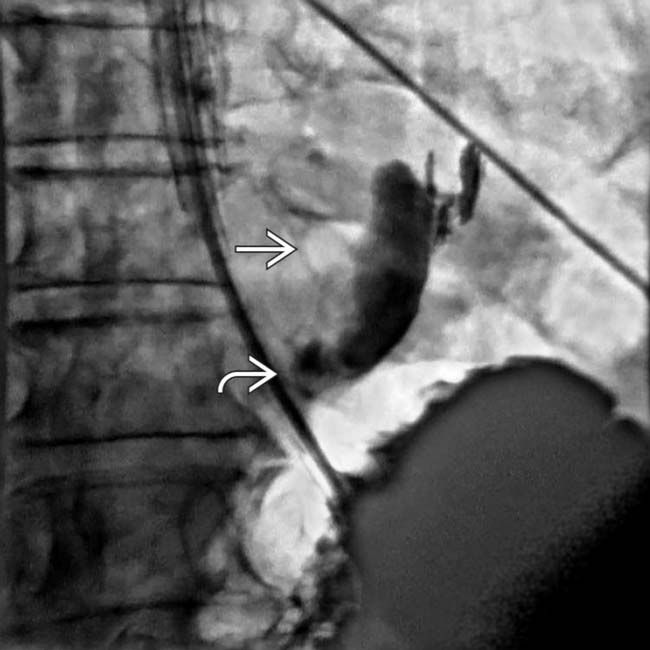
 from a tear in the left anterior wall of the distal esophagus
from a tear in the left anterior wall of the distal esophagus  , a classic appearance for Boerhaave syndrome.
, a classic appearance for Boerhaave syndrome.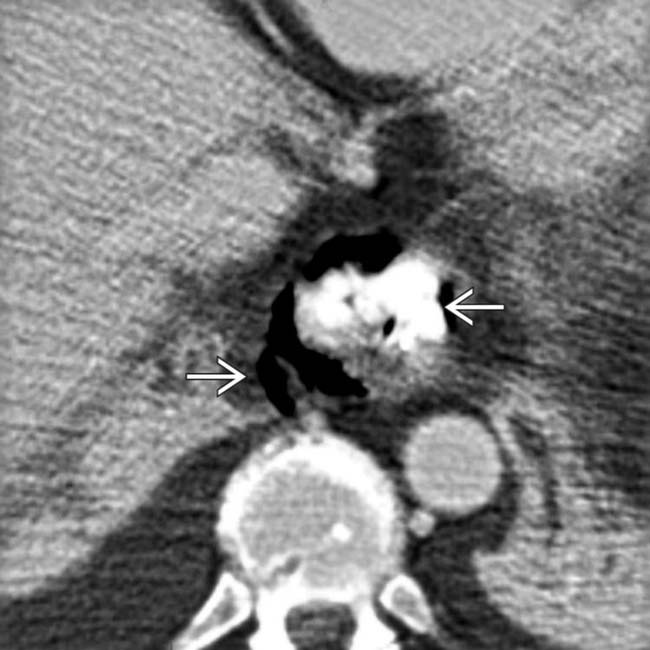
 surrounding the esophagus in the lower mediastinum and upper abdomen.
surrounding the esophagus in the lower mediastinum and upper abdomen.
 . The site of the tear is the left anterior wall
. The site of the tear is the left anterior wall  of the distal esophagus.
of the distal esophagus.



















 dissecting through the mediastinum. Note the perforation of the distal esophagus
dissecting through the mediastinum. Note the perforation of the distal esophagus  . Immediate drainage was required.
. Immediate drainage was required.
 .
.
 in the mediastinum.
in the mediastinum.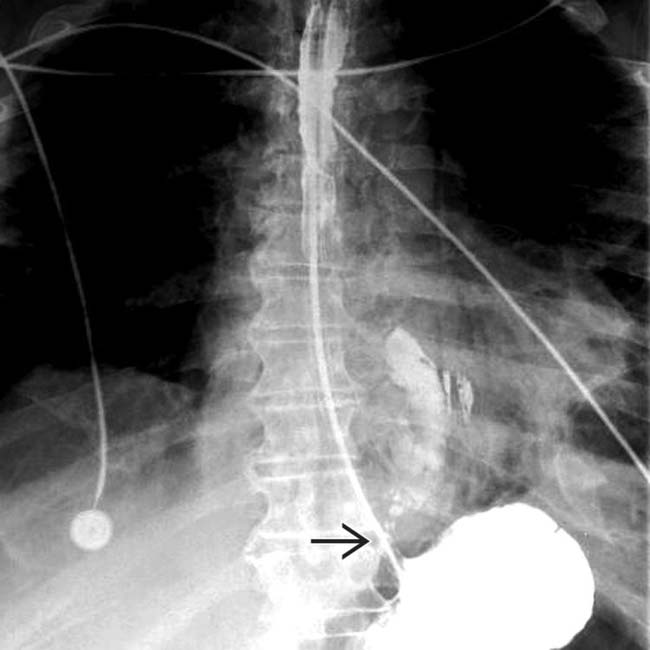
 in the distal left side of the esophagus.
in the distal left side of the esophagus.
 but no apparent leak of contrast material.
but no apparent leak of contrast material.
 with relatively mild periesophageal inflammatory changes.
with relatively mild periesophageal inflammatory changes.
