Blistering disorders
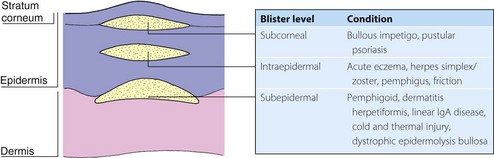
Blistering is often seen with skin disease. It is found with common dermatoses such as acute contact dermatitis, pompholyx, herpes simplex, herpes zoster and bullous impetigo, and it also occurs after insect bites, burns and friction or cold injury. The type of blister depends on the level of cleavage: subcorneal or intraepidermal blisters rupture easily, but subepidermal ones are not so fragile (Fig. 1). The primary acquired autoimmune bullous disorders, dealt with here, are rare but important.
Pemphigus
Aetiopathogenesis
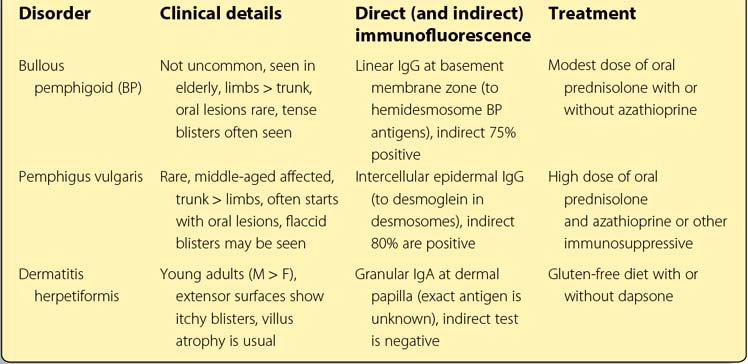
Over 80% of patients have circulating immunoglobulin (Ig) G autoantibodies detectable in the serum by indirect immunofluorescence (p. 127), which bind with desmoglein, a desmosomal cadherin involved in epidermal intercellular adhesion. The antibodies, possibly with complement activation and protease release, result in loss of adhesion and an intraepidermal split. Direct immunofluorescence shows the intercellular deposition of IgG in the suprabasal epidermis. Pemphigus is associated with other organ-specific autoimmune disorders such as myasthenia gravis.
Clinical presentation
Less common variants include pemphigus foliaceus, in which shallow erosions appear on the scalp, face and chest (Fig. 2), and pemphigus vegetans, in which pustular and vegetating lesions affect the axillae and groins. In Brazil, an endemic form of pemphigus foliaceus, fogo selvagem, seems to be induced by an infective agent. Paraneoplastic pemphigus describes a variant associated with underlying malignancy.

Pemphigoid
Pemphigoid is a chronic and not uncommon blistering eruption of the elderly.
Aetiopathogenesis
IgG autoantibodies to bullous pemphigoid antigens BP230 and BP180 in the hemidesmosomes at the basement membrane zone bind complement, which induces inflammation and protease release, leading to subepidermal bulla formation. The IgG and C3 are detected by direct immunofluorescence (p. 127). Indirect methods demonstrate circulating autoantibodies in 75% of cases.
Clinical presentation
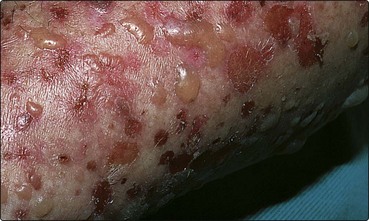
Bullous pemphigoid usually affects the elderly. Tense large blisters arise on red or normal-looking skin, often of the limbs, trunk and flexures (Fig. 3). Oral lesions occur in only 10% of cases. A pruritic urticarial eruption may precede the onset of blistering. Pemphigoid is sometimes localized to one site, often the lower leg. The differential diagnosis of pemphigoid may include dermatitis herpetiformis, linear IgA disease or pemphigus. Immunofluorescence and histology reveal the diagnosis.
Management
Pemphigoid responds to a lower dose of steroids than pemphigus: 0.5 mg/kg daily of oral prednisolone is usually sufficient, and this can normally be reduced to below 15 mg within weeks. Azathioprine is sometimes also prescribed. The disease is self-limiting in many cases, and steroids can often be stopped after 2–3 years. Cicatricial pemphigoid does not respond so well, but pemphigoid gestationis is controlled by standard doses. Steroid-induced side-effects may be a problem, especially in the elderly.
Dermatitis herpetiformis
Clinical presentation
DH usually presents in the third or fourth decade and is twice as common in males as in females. The classical onset is with groups of small, intensely itchy vesicles on the elbows, knees, buttocks and scalp (Fig. 4). The blisters are often broken by scratching to leave excoriations. Although most patients have small bowel villus atrophy, symptoms of gastrointestinal disturbance and malabsorption are uncommon.

Differential diagnosis
Distinction from scabies, eczema and linear IgA disease is important. Biopsy shows a subepidermal bulla, and direct immunofluorescence of normal-looking skin demonstrates granular IgA at the dermal papilla (p. 127). The small bowel can be investigated by jejunal biopsy. Serum folate, vitamin B12 and ferritin estimates detect any biochemical malabsorption. Antiendomysial antibodies are present.
Linear IgA disease
Linear IgA disease is a rare heterogeneous condition of blisters and urticarial lesions on the back or extensor surfaces (Fig. 5). The disorder responds to dapsone and may resemble DH or pemphigoid. Direct immunofluorescence reveals linear IgA at the basement membrane. In the childhood variant, blisters occur around the genitalia. Linear IgA disease induced by medication (commonly vancomycin) is well recognized.