[level-membership-for-emergency-medicine-category]
BLEEDING
For a discussion of wound management (cleaning, closing, and dressing), see page 260.
While it is occasionally visually distressing, bleeding can be one of the easiest problems to manage, because the treatment options are so straightforward. The severity of the injury determines the rate of blood loss and what measures you must take to control the bleeding. Evaluate the following considerations:
1. Where is the bleeding? It is important to consider and identify internal bleeding as well as external bleeding. Considerable blood loss can be associated with blunt (nonpenetrating) abdominal injury (liver, spleen), as well as long bone or pelvic fracture (2 quarts, or liters, of blood can rapidly accumulate in the thigh following a broken femur). Examine the entire victim!
2. Is the bleeding from an artery or from a vein? Because arterial blood is under higher pressure, blood loss tends to be more rapid from a severed artery than from a vein. Arterial bleeding can be recognized by its spurting nature and rapid outflow. All blood exposed to air, in the absence of unusual drug intoxications, turns red fairly quickly, so you cannot rely on color to indicate origin.
TREATMENT FOR BLEEDING
First, remove all clothing covering the wound so that you can see precisely where the bleeding is coming from. Almost all external bleeding stops with firm, direct pressure. This should be applied directly to the wound with the heel of your hand, using the cleanest available thick (four or five thicknesses of a 4 in by 4 in—or 10 cm by 10 cm—sterile gauze pad, for instance) bandage or cloth compress (Figure 31). Maintain pressure for a minimum of 10 minutes, to allow severed vessels to close by spasm (an artery contains small amounts of muscle tissue in its walls) and to allow early blood clot formation. Peeking at the wound under the compress interrupts the process and prolongs active bleeding. The application of cold packs or ice packs over the compress (not under it) may hasten the process by initiating spasm and closure of disrupted blood vessels. It is also useful to have the victim lie down, and to elevate the bleeding part above the level of his heart. A scalp wound tends to bleed freely, and may require prolonged pressure or wound closure for control (see page 65).

If direct pressure to the wound does not stop the bleeding, you must make certain that you are applying the pressure in the correct spot. Check quickly to see that you are pressing precisely over the bleeding point. If you are a fraction of an inch off, you can miss the best compression spot for a torn blood vessel; in this case, simply piling on more bandages may not solve the problem. Once you have repositioned your pressure, wait again for 5 to 10 minutes. If the pressure appears to be working, once the bleeding has substantially subsided you can apply a pressure dressing. Do this by covering the wound with a thick wad of sterile gauze pads or the cleanest dressing available, and wrapping the area firmly with a rolled gauze or elastic bandage. Do not apply the dressing so tightly that circulation beyond it is compromised (as indicated by blue fingertips or toes, or by numbness and tingling). Watch the dressing closely for blood soaking and dripping, which indicate continuous bleeding.
To apply Celox, one pours the granules from a sterilized, sealed packet (15 grams or 35 grams) into the wound and then holds them in place with a gauze bandage for 5 minutes. A compression bandage, such as an elasticized wrap, is then wrapped over the gauze-covered wound and the victim is brought to medical care.
The following are some important things to be aware of with a serious wound:
1. A victim who has lost 25% to 30% of his blood volume may suffer from shock. Treatment is discussed on page 60.
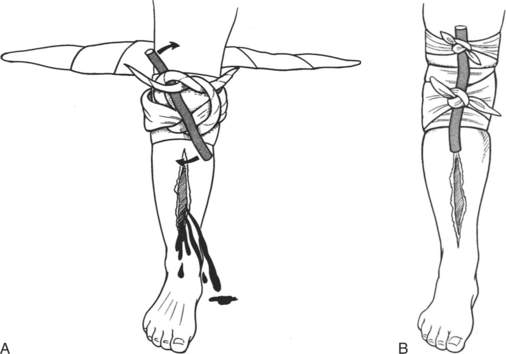
2. Prolonged uncontrollable bleeding is rare unless a major blood vessel or more than one vessel is disrupted, the victim is taking an anticoagulant (blood thinner) medication, or the victim suffers from hemophilia. In such a case, heroic intervention may be lifesaving. The application of extreme compression to “pressure points,” such as the radial, brachial, or femoral arteries, is both difficult and of considerable risk (since the purpose is to cut off all circulation).
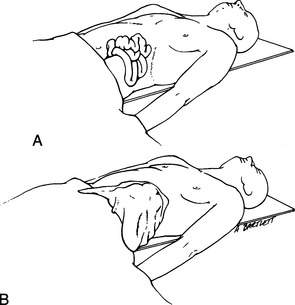
3. If the victim has suffered a large wound through which internal organs (such as loops of bowel) (Figure 33, A) or bones (see page 71) are protruding, do not attempt to push these back inside the body or under the skin unless they slide back in without your assistance. Cover extruded internal organs or bones with continually moistened bandages (pads of gauze or cloth) held in place without excess pressure (Figure 33, B). Seek immediate medical attention.
4. If the victim has suffered a severe cut in his neck, take special care to not disturb the wound, because such disturbance might remove a blood clot that is controlling the bleeding from a large blood vessel. Apply a firm pressure dressing (don’t choke the victim with the bandage) and seek immediate medical attention. Continually assess the airway (see page 22), because an expanding blood clot within the neck can compress the throat and windpipe. If the victim begins to have raspy breathing or a changed voice, evacuation is maximally urgent.
5. Bleeding can be quite brisk from a ruptured or torn varicose (dilated) vein in the leg. This can usually be managed with direct pressure, while elevating the leg. Follow this with a pressure dressing.
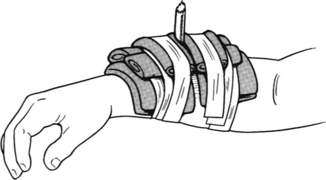
6. If a foreign object (such as a knife, tree limb, or arrow) becomes deeply embedded (impaled) in the body, do not attempt to remove it, because the internal portion may be occluding a blood vessel that will hemorrhage without this “plug.” Any attempt at removal may create more damage than already exists, which includes increasing the bleeding. This is particularly true with a hunting (broadhead) arrow. Instead, pad and bandage the wound around the object, which should be fixed in place with tape if possible (Figure 34). The external portion of the object may be cut to a shorter length (cut off the shaft of the arrow a few inches above the skin, for example), if necessary, to facilitate splinting and transport of the victim.
7. A gunshot wound may cause severe internal damage that is not readily visible from the surface wound. Any victim who has suffered a gunshot wound should be brought to immediate medical attention, no matter how minor the external appearance.
8. There are “blood stopper” products that can be used to assist in controlling bleeding (see page 55). These include QuickClot Sport (Z-Medica), which is a porous sack filled with a highly absorbent mineral derived from lava rocks; QR (Biolife LLC), which is a powder composed of tiny plastic beads and potassium salt that is sprinkled on a wound; and bandage and gauze products (such as BloodStop [LifeScience Plus Inc.]) made from cellulose that transform on contact with blood and accelerate clot formation.
9. After the bleeding has stopped, immobilize the injury. Check all dressings regularly to be certain that swelling has not made them too tight.
[/level-membership-for-emergency-medicine-category][not-level-membership-for-emergency-medicine-category]
BLEEDING
For a discussion of wound management (cleaning, closing, and dressing), see page 260.
While it is occasionally visually distressing, bleeding can be one of the easiest problems to manage, because the treatment options are so straightforward. The severity of the injury determines the rate of blood loss and what measures you must take to control the bleeding. Evaluate the following considerations:
1. Where is the bleeding? It is important to consider and identify internal bleeding as well as external bleeding. Considerable blood loss can be associated with blunt (nonpenetrating) abdominal injury (liver, spleen), as well as long bone or pelvic fracture (2 quarts, or liters, of blood can rapidly accumulate in the thigh following a broken femur). Examine the entire victim!
2. Is the bleeding from an artery or from a vein? Because arterial blood is under higher pressure, blood loss tends to be more rapid from a severed artery than from a vein. Arterial bleeding can be recognized by its spurting nature and rapid outflow. All blood exposed to air, in the absence of unusual drug intoxications, turns red fairly quickly, so you cannot rely on color to indicate origin.
TREATMENT FOR BLEEDING
First, remove all clothing covering the wound so that you can see precisely where the bleeding is coming from. Almost all external bleeding stops with firm, direct pressure. This should be applied directly to the wound with the heel of your hand, using the cleanest available thick (four or five thicknesses of a 4 in by 4 in—or 10 cm by 10 cm—sterile gauze pad, for instance) bandage or cloth compress (Figure 31). Maintain pressure for a minimum of 10 minutes, to allow severed vessels to close by spasm (an artery contains small amounts of muscle tissue in its walls) and to allow early blood clot formation. Peeking at the wound under the compress interrupts the process and prolongs active bleeding. The application of cold packs or ice packs over the compress (not under it) may hasten the process by initiating spasm and closure of disrupted blood vessels. It is also useful to have the victim lie down, and to elevate the bleeding part above the level of his heart. A scalp wound tends to bleed freely, and may require prolonged pressure or wound closure for control (see page 65).
If direct pressure to the wound does not stop the bleeding, you must make certain that you are applying the pressure in the correct spot. Check quickly to see that you are pressing precisely over the bleeding point. If you are a fraction of an inch off, you can miss the best compression spot for a torn blood vessel; in this case, simply piling on more bandages may not solve the problem. Once you have repositioned your pressure, wait again for 5 to 10 minutes. If the pressure appears to be working, once the bleeding has substantially subsided you can apply a pressure dressing. Do this by covering the wound with a thick wad of sterile gauze pads or the cleanest dressing available, and wrapping the area firmly with a rolled gauze or elastic bandage. Do not apply the dressing so tightly that circulation beyond it is compromised (as indicated by blue fingertips or toes, or by numbness and tingling). Watch the dressing closely for blood soaking and dripping, which indicate continuous bleeding.
[/not-level-membership-for-emergency-medicine-category]
