Birdshot Chorioretinopathy
Clinical Features:
Decreased vision, photopsias, floaters, nyctalopia, and decreased color vision are frequent symptoms. There is minimal to no anterior uveitis with mild vitritis. Multifocal depigmented cream-colored retinal pigment epithelium lesions less than one disc diameter in size are scattered throughout the fundus, although these may be absent or very subtle in the early stages of the disease (Fig. 17.2.1). Retinal phlebitis, narrowing and sheathing of retinal vasculature, disc edema, optic atrophy, cystoid macular edema, choroidal neovascularization and epiretinal membrane may also develop.
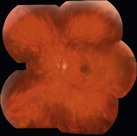
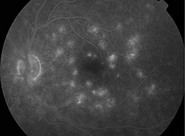
Figure 17.2.1 Characteristic fundus photograph of a patient with birdshot with hypopigmented lesions noted extending into the mid-periphery. Late frames of the fluorescein angiography show hyperfluorescence, and late-frame indocyanine green angiography shows the lesions as hypofluorescent spots with some diffuse hyperfluorescence.
OCT Features:
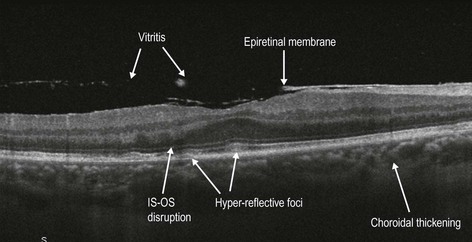
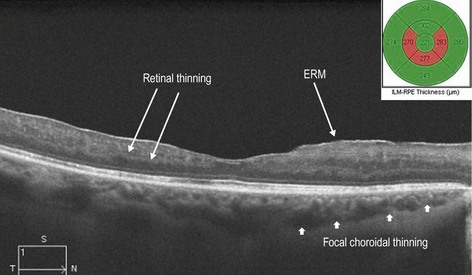
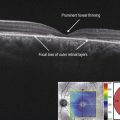
Lines scan of the macula may show the typical features of birdshot: epiretinal membrane formation and macular edema (Fig. 17.2.2). Subretinal fluid may be seen in severe cases of macular edema. In chronic cases, the macula is diffusely thin and disruption of the IS–OS segment/ellipsoid layer with disorganization of the inner retinal layers and retinal pigment epithelium atrophy may be seen (Fig. 17.2.3). Extramacular and enhanced depth OCT images provide greater information than macular scans, because the choroidal lesions themselves can be scanned. Focal and generalized loss of the IS–OS junction/ellipsoid layer, loss of retinal architecture and outer retinal hyper-reflective foci overlying the lesions is typical. Generalized thinning of the choroid and outer retina, and hyporeflective suprachoroidal space are other features.