[level-membership-for-orthopaedics-category]16
Biomechanical Basis for Movement
Mitchell A. Collins and Michael Hales
1. Define and apply biomechanical concepts in the description of rudimentary movement patterns.
2. Discuss the difference between the kinematics and kinetics of movement.
3. Identify and discuss the kinematic principles as related to movement in a rehabilitation setting.
4. Discuss both the linear and angular kinematics and kinetics of movement, and explain how angular motion translates to linear movements.
5. Describe the differences among the different levers, and explain the concept of mechanical advantage as related to levers.
6. Describe Newton’s laws of motion.
7. Identify and discuss the different forces that act on objects and how the forces affect movement.
8. Discuss the concepts of mechanical loading, and describe how loading is associated with different types of injuries.
9. Discuss the principles of mechanical energy.
10. Describe the concept of equilibrium and identify the factors that contribute to stability.
Biomechanics is the study of the internal and external forces acting on the body and the effects these forces produce. The data obtained from biomechanical research provide a great deal of insight into human movement interactions in fields such as physical and occupational therapy, sports medicine, human factors, prosthetics, orthotics, and ergonomics.12,31 Clinical biomechanics, a subdiscipline, provides direct measures of human motion which influence our knowledge of injury mechanics, rehabilitation, treatment, and prevention. This information can directly affect how a physical therapist assistant (PTA) rehabilitates a patient, an orthopedist repairs a broken limb or ruptured ligament, an athletic trainer implements modalities for treatment, or a clinician evaluates an individual’s gait.19,21,24
Biomechanics can provide the health professional with a better understanding and a broadened knowledge of the causes and degrees of severity associated with an injury. In order to improve upon a current rehabilitative technique, repair procedure or treatment process, the mechanics associated with the causation of the injury must be fully understood. To help the health professional accomplish this task, several factors need consideration when determining the cause and severity of an injury36:
 How much force was applied? (magnitude)
How much force was applied? (magnitude)
 Where on the body was the force applied? (location)
Where on the body was the force applied? (location)
 Where was the force directed? (direction)
Where was the force directed? (direction)
 How long was the force applied? (duration)
How long was the force applied? (duration)
 How often was the force applied? (frequency)
How often was the force applied? (frequency)


The major role of a PTA revolves around both the causes and effects of human motion and therefore it is imperative to have a fundamental understanding of the mechanical basis for whole body or segmental movement. Since biomechanics is concerned with the effects of forces on the human body, biomechanical principles are involved when a force is present. The following chapter will offer an overview of the science of biomechanics with practical applications for the PTA.
REFERENCE TERMINOLOGY
To facilitate the process of describing human movement, standardized terminology has been adopted to identify body positions and directions of motion (Box 16-1). Movements are defined based on a reference or starting position often referred to as the anatomic position (Fig. 16-1, A), which is a standing position with arms at one’s side and palms facing forward. From the anatomic position, three imaginary cardinal planes bisect the body along three dimensions (Fig. 16-1, B). The transverse or horizontal plane segments the body into upper and lower parts; the frontal or coronal plane separates the body into front and back parts; and the sagittal or anteroposterior plane divides the body into right and left parts. It is important to note that the planes do not necessarily divide the body into equal parts. However, when the segments are equal, the mid-intersection point of the transverse, frontal, and sagittal planes is referred to as the center of mass (COM) or center of gravity (COG). Although human movement is not restricted to a single plane, most named movements (e.g., flexion and abduction) are described based on the three cardinal planes.
BOX 16-1 Basic Directional Terms Used to Describe Body Parts or Other Objects in Relation to the Body










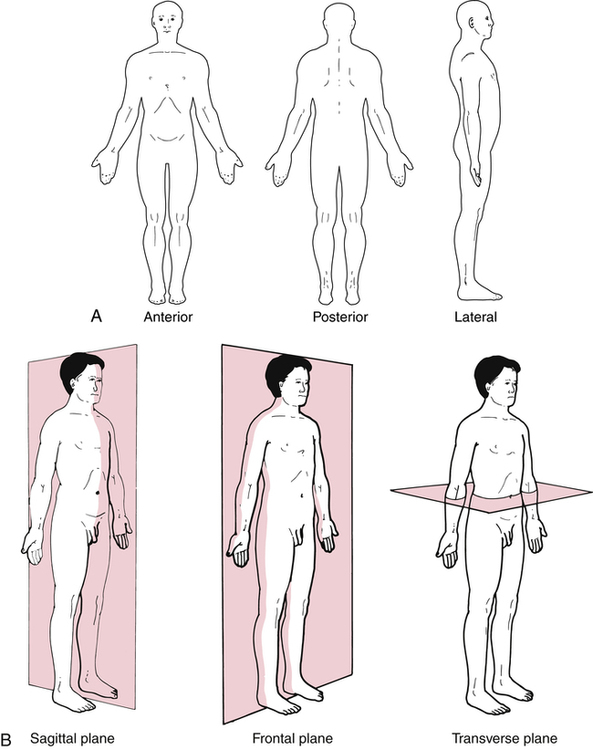
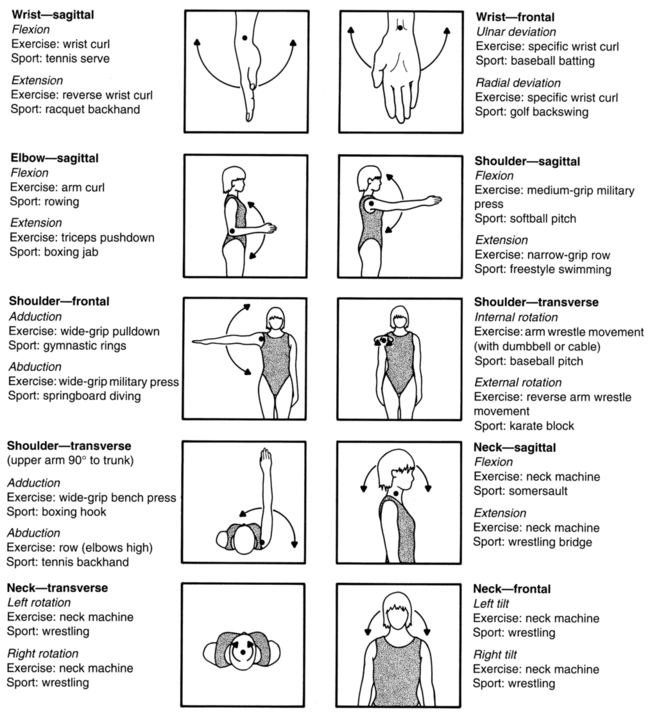
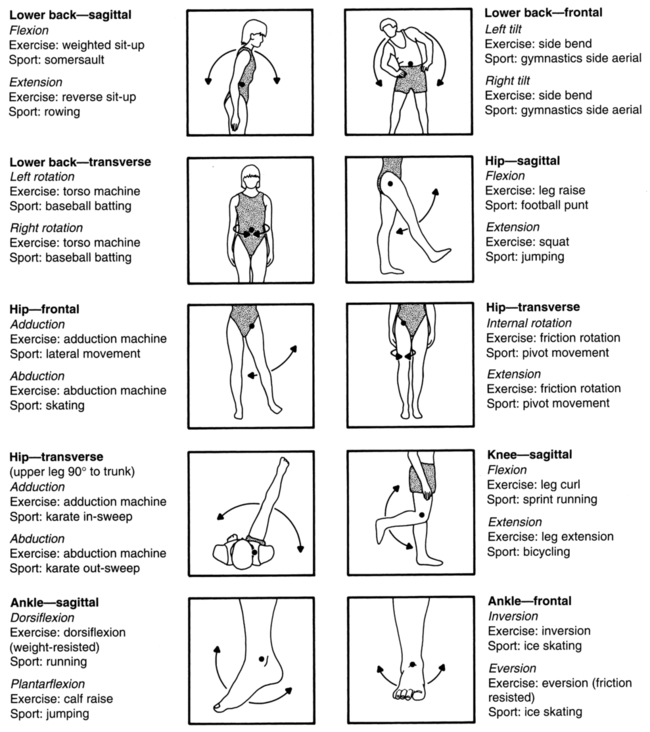
Movements in the transverse plane occur around the longitudinal axis, which runs superiorly–inferiorly while perpendicularly intersecting the transverse plane. These movements include medial and lateral rotation of the leg, thigh, and shoulder; supination and pronation of the forearm; and horizontal abduction and adduction of the shoulder. Movements in the frontal plane occur around the sagittal axis, which runs anteriorly–posteriorly while perpendicularly intersecting the frontal plane. These movements include abduction and adduction of the shoulder and hip, lateral flexion of the neck and trunk, elevation and depression of the shoulder girdle, and inversion and eversion of the foot. Movements in the sagittal plane occur around the frontal axis, which runs from left to right while perpendicularly intersecting the sagittal plane. These movements include flexion and extension of the knee, hip, trunk, elbow, shoulder, and neck; and dorsiflexion and plantar flexion of the foot as well as hyperextension movements. A key role of the PTA is to facilitate patient rehabilitation through the incorporation of various exercises using basic movement patterns. Therefore it is important to be familiar with the appropriate terminology for these movements (Fig. 16-2).
BASIC CONCEPTS
Pressure (p) is a measure of the distribution of a force over a given area (force/area), and it is expressed in newtons per meter2 (N/m2). An example of the concept of pressure in a rehabilitation setting is the development of decubitus ulcers that commonly occur among diabetics.3,32,38 Innovations in shoe design help dissipate the forces applied to the foot over a larger area (e.g., reduced pressure) during locomotion, thus minimizing soft-tissue damage and the incidence of ulceration.6,10,35
BIOMECHANICAL PRINCIPLES
Statics and Dynamics
Linear and Angular Motion
Angular motion is the measurement of rotation about an axis of a rigid lever and is quantified through the use of a polar coordinate system. This is generally represented in the human body by body segments; an example is the upper arm rotating about a joint (axis of rotation) such as the shoulder. By tracking over time how the lever, as established by its endpoints (for the upper arm these would be represented by a line connecting the shoulder and elbow), rotates around its proximal joint (the shoulder), one can determine angular positional changes of the lever, rotational velocities of the lever about the joint, and increases/decreases in rotational velocity. These angular measures describe the quality of motion generated angularly by an individual performing an activity of daily living (ADL), occupational activity, or exercise. This is important because there is a direct link between the quality of angular motion of body segments or levers and the potential for overuse injuries to the subsequent joints. For example, the faster the forearm/racket combination is rotating or extending about the elbow at the instant before impact in a tennis serve, the faster the racket is moving linearly at the moment of impact with the ball. The faster the racket head is moving linearly at impact, the greater the momentum or force imparted to the tennis ball by the athlete. Conversely, because of the high action force and moment, the greater the reaction force and moment imposed on the joints, which could lead to inflammation of the lateral epicondyle (tennis elbow) if poor service mechanics are demonstrated.22 The rotation of the forearm about the elbow is due in part to the contraction of the muscles (triceps group), which causes acceleration in the direction of elbow extension. The linear force of the triceps tendon pulling on the ulna generates a torque or rotational force. The greater the torque produced by the muscles, the greater the angular acceleration generated, leading to changes in angular velocity that lead to changes in angular position.
Kinematics and Kinetics
An understanding of kinematic principles is extremely important to PTAs. Analysis of motion can facilitate the determination of the etiology of injury, extent of damage, and assessment of the effectiveness of treatment. Historically, researchers have studied injuries in sport settings, but the same applications are pertinent to nonathletic settings, such as gait analysis of individuals with lower extremity joint injury or joint replacement.7,9,11,16,27,28 Thus it is imperative for PTAs to be knowledgeable about normal movement patterns from a kinematic perspective to facilitate the recognition of abnormal movements of rehabilitating patients.
Newton’s Laws of Motion
Newton’s first law of motion is commonly referred to as the law of inertia, which states:
“A body remains in a state of rest, or of uniform motion in a straight line, unless it is compelled to change that state by forces impressed on it.”5
Inertia of an object is used to describe the reluctance of an object to change its movement pattern; that is, to stay motionless or to move in a linear path unless a force is applied. The amount of inertia an object possesses is related to the mass of the object. As a result, the larger the mass or inertia of an object, the more difficult it is to alter its motion. We can observe the concept of inertia by examining events that occur during car accidents. If an automobile is struck in the rear by another vehicle, the head of the passenger tends to remain at rest momentarily as the body is thrust forward. Whiplash is the term used to describe the injury mechanism of the anterior longitudinal ligament.37 Conversely, when a car strikes an object and is suddenly forced to stop, the passenger continues to move forward because of the person’s inertia. This forward motion continues to occur until a force is applied (hopefully seat belts and air bags) to counteract the inertia. However, if the passenger is wearing a seat belt but an air bag is either not present or fails to deploy, the head tends to continue moving forward as the body stops. Basilar skull fractures are a common cause of death among race car drivers when their vehicle collides head-on with the race track concrete barrier at extremely high speeds.24
Newton’s second law of motion is commonly referred to as the law of acceleration, which states that the change of motion is proportional to the force impressed and is made in the direction of the straight line in which that force is impressed.5
This law can be expressed algebraically with force (F), mass (m), and acceleration (a):
< ?xml:namespace prefix = "mml" />

When the equation is rearranged, it yields a useful expression:

which mathematically illustrates that the acceleration of an object is directly proportional to the force applied and inversely related to mass of the object. Newton’s second law is relatively simple, but it has many applications to physical therapy. Because acceleration (motion) is inversely related to mass, it is clear that basic weight-bearing movements tend to be more challenging for larger patients. In addition, a greater force application is needed for these patients to accomplish said movement. The difficulty in locomotion is compounded if larger mass of a patient results from too much fat, because fat does not contribute to force production.
Newton’s third law of motion is commonly referred to as the law of reaction, which states that to every action there is always opposed an equal reaction; or, the mutual action of two bodies upon each other are always equal and directed to contrary parts.5
The concept of reaction can be more difficult to visualize than inertia and acceleration, but when a force is applied to an object such as a wall, there is a force opposite in direction and equal in magnitude to the force applied. As the applied force increases, the reaction force likewise increases. From a clinical perspective, reaction forces are of interest during gait analysis. When a patient walks or runs, clinicians may analyze the differences in gait patterns among individuals with varying levels of disability and the subsequent ground reaction forces that occur when the foot strikes the floor. These forces can achieve three times one’s body weight during running, and patterns vary based on running style. Physicians and therapists use devices such as orthotics to alter ground reaction force patterns to help minimize foot injuries.33
ADVANCED BIOMECHANICAL CONCEPTS
Reaction Forces
Reaction forces are forces applied on a person by a surface with which the person’s body is in contact. These forces are applied as an equal and opposite reaction force to the force applied to the surface by the person. The more force generated by the person onto the contact surface, as a result of their body weight and musculoskeletal activity, the more force the surface returns to the performer. When analyzing gait abnormalities, ground reaction forces (GRFs) should be measured in relation to a fixed three-dimensional coordinate system oriented at the surface of the platform.30 The GRF planes of motion are termed anteroposterior, which describes forces imposed horizontally directed forward or backward; mediolateral, which describes forces generated horizontally side to side; and vertical, which describes forces directed upward or downward. In other words, if the person pushes downward on the surface the surface reacts by pushing upward with equal force. If the person pushes backward on the surface the surface pushes forward with an equal force. If the person pushes rightward on the surface the surface pushes leftward with equal force. Other sources for force application are wheelchair pushrims, which are referred to as pushrim reaction forces. These multidirectional forces are applied to the hand when in contact with the wheelchair pushrim in an equal and opposite manner. The forces specific to a pushrim are termed tangential, which describes forces applied tangent to the pushrim (causes motion); radial, which describes the forces directed toward the axis of rotation (frictional force); and mediolateral, which describes forces directed parallel to the axis of rotation. The forces imposed at the pushrim are transferred to the hand and used to determine subsequent upper extremity joint forces and moments during wheelchair ambulation. Chronic and acute shoulder pain of manual wheelchair users is one of the foremost issues facing PTAs.2,4,8
Levers and Resistive Torque

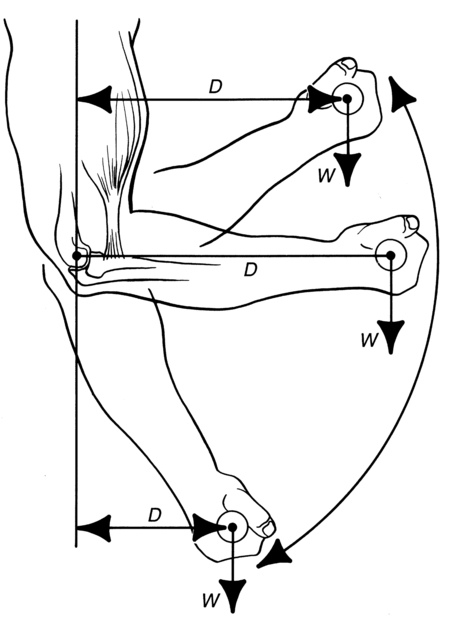
In a first-class lever, when the fulcrum is located halfway between the point of force and point of resistance on the lever, the MA is equal to 1 (e.g., MF = MR). If the fulcrum is closer to the point of the resistance than the point of force (e.g., MF > MR), the MA becomes greater than 1; thus a smaller force is necessary to overcome a constant resistance. In the opposite scenario where the MF is less than the MR, the MA is less than 1 and a larger force is necessary to move a given resistance. The head tilting backward, initiated by a concentric contraction of the extensor neck muscles (splenius capitis, semispinalis capitis, suboccipitals, trapezius) to overcome the resistive force imposed by the weight of the cranium where the fulcrum is the atlanto-occipital joint, is an example of a first-class lever system (Fig. 16-3, A).
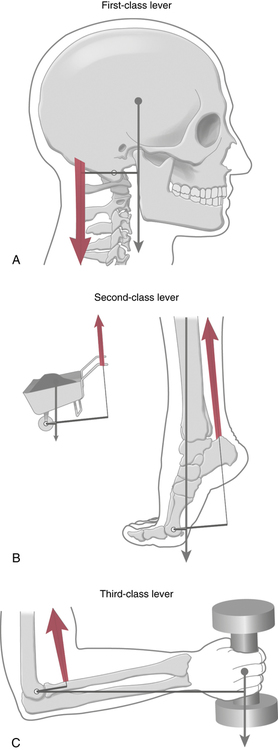
In a second-class lever, the point of resistance is located between the fulcrum and the point of force. The MF is always greater than the MR, yielding a MA greater than 1. Hence this arrangement favors the effort of force, because less force is necessary to cause movement of a given resistance. Performing a toe raise exercise demonstrates a second-class lever. The plantar and dorsiflexion movement can be employed by the PTA to regain ankle ROM due to injury or surgery. Resistance can be added to create an exercise designed to strengthen the calf muscles (soleus and gastrocnemius), which represents a second-class lever system (Fig. 16-3, B).
In a third-class lever, the point of force is located between the fulcrum and the resistance. The MF always is less than the MR, yielding a MA less than 1. Therefore this arrangement favors the effort of resistance, because more force is necessary to cause movement of a given resistance. This is the more common type of lever found within the human body (Fig. 16-3, C). Therefore muscles within the body tend to work under a mechanical disadvantage, resulting in larger internal muscular forces than the mass of the external object (resistance) being moved. It is also important to realize that within some joints of the skeletal system, the actual fulcrum point changes through the ROM. Consequently, mechanical advantage and muscle force vary as the length of the moment arm changes. A person performing elbow flexion during a bicep curl exercise depicts a third-class lever system. The olecranon represents the axis of rotation where the biceps muscle group (biceps brachii, brachioradialis, brachialis) exerts a force to overcome the mass of the forearm or any additional resistance held in the hand.
The resistive force, or more specifically the resistive torque, encountered during movements varies based on the length of the resistance arm (moment arm of the resistance). During the performance of a bicep curl exercise, length of the resistance arm is maximized when the elbow is at a 90-degree angle (Fig. 16-4). As the angle increases or decreases, the length of the resistance arm shortens, thus reducing the magnitude of the resistive torque.26 Therefore it is important to realize that less force is necessary to lift a given resistance when the resistance is closer to the fulcrum (e.g., the resistance arm is reduced). This basic biomechanical principle has numerous applications, including the mechanical function of exercise equipment. Various manufacturers use a pulley system consisting of cam-based pulleys. The unique advantage of a cam compared with a traditional round pulley is the variation in the length of the resistance and force arms during rotation of the pulley. By simply increasing the length of the resistance arm or reducing the length of the force arm, the resistive torque can be increased to provide a variable resistance through the ROM. This relatively simple alteration in design has enhanced the effectiveness of exercise equipment to provide proper loading on muscles throughout the full ROM.
Kinetic Link Principle
Body segments are connected in more ways than most individuals realize. When there is a perpetual orthopedic problem in one area of the body, chances are the problem is related to another area of the body in some form or fashion. For example, if patients complain their ankles or knees hurt when they walk, it could be linked to an orthopedic issue with their feet. The foot pain could be directly associated with a problem in the calf region. A taut gastrocnemius–soleus muscle group can often lead to problems in the knees, hips, and lower back area. If this is ignored, the problem can migrate to the upper back, shoulders, and neck. In a sense, everything in the body is connected, in other words, it is a kinetic chain. When a part of this chain is weak or damaged, it will affect other parts of the kinetic chain (Box 16-2).
BOX 16-2 Sequential Kinetic Chain




Squat lifting is an example of movement requiring force generation by several muscle groups simultaneously. These types of movements generally need high force magnitudes to overcome relatively high inertial conditions.25
Balance and Stability
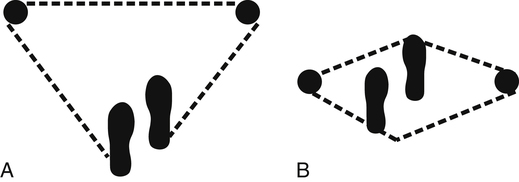
Realize that biomechanically, stability and mobility are inversely related. A health professional can apply the principle of balance to provide a patient with an appropriate mix of stability and mobility for a particular activity or skill. Three biomechanical factors directly affect an individual’s balance for improving stability: body mass, COG reference height, and base of support area.1,17 The stability of the human body with respect to the base of support depends on the overall size of the base of support and the height of the body’s COG above the base of support. For example, a person recovering from a lower extremity injury may use crutches or a walking cane in order to relieve the load on the injured limb. The use of crutches also increases the area of the base of support and makes it easier for the user to maintain stability (Fig. 16-5).29,34 Postural sway is normally under the control of automatic neuromuscular mechanisms that dictate the adequate base of support area. However, those mechanisms are diminished in patients with a muscle atrophy disease or neurological disorder. The use of crutches would greatly increase the stability of these individuals.29,34
BASIC BIOMECHANICAL ANALYSES OF INJURY MECHANISMS
Mechanical Loading
There are three types of stresses: compression, tension, and shear (Fig. 16-6). Compression occurs when two forces or loads are applied toward each other. A common example is the compression stress on the vertebral column during standing while supporting an object (e.g., dumbbell). Excessive compression stress can lead to contusions, fractures, or herniations.23,25 Tension occurs when two forces or loads are applied in opposite directions. This type of loading is commonly applied to muscles and tendons during stretching activities to improve flexibility.
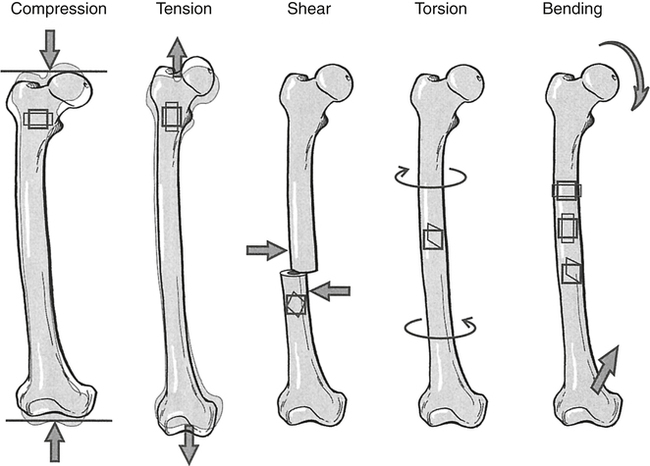
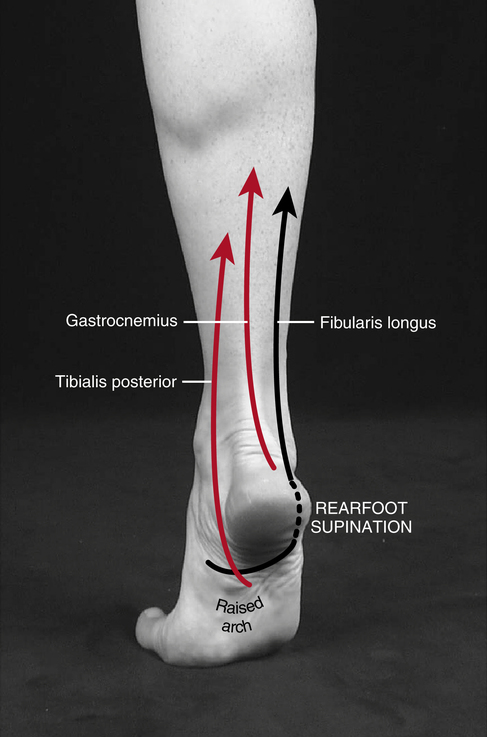
When the loading exceeds the ability of the object to resist the stress, injuries such as strains, sprains, and avulsion fractures commonly occur.20 Figure 16-7 illustrates the tension stresses acting on the Achilles tendon during movements of the foot. Injuries associated with tension are more common during activities that utilize the stretch-shortening cycle most often observed during actions that require fast, quick, change in direction movements. Shear occurs when there are two parallel forces or loads in opposite directions, causing adjacent points on the surface to slide past each other. Injuries such as vertebral disk problems, femoral condyle fractures, and epiphyseal fractures of the distal femur in children occur as a result of shear stress acting on the body.
The resulting action of compression, tension, and shear forces is dependent on how these forces are distributed, a concept called mechanical stress. Force applied over a smaller surface area results in a greater mechanical stress than force applied over a larger surface area. Given that the lumbar vertebrae typically are more load bearing than the vertebrae in the upper back, one notices that the load-bearing surface area in the lumbar vertebrae is greater than that found in the upper vertebrae.18 Accordingly, the greater surface area for the thoracic vertebrae translates into a lower mechanical stress for a given load.
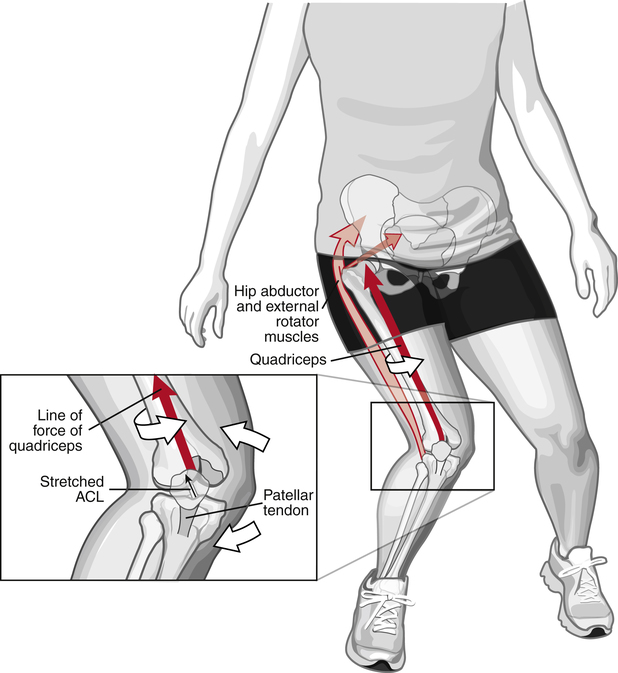
Another type of loading on an object, called bending, occurs when nonaxial forces are applied, resulting in compressive stress on one side and a tension stress on the other. When an object is forced to twist along the longitudinal axis, a load called torsion is produced. Injuries commonly occur because of torsion in activities such as skiing, when a foot is planted and the body begins to twist.11,16 Another example is an anterior cruciate ligament (ACL) injury, which commonly occurs during a running activity when one suddenly stops and then turns, thereby causing a deceleration of the lower limb, a forced hyperextension of the knee, or a forced tibial rotation (Fig. 16-8). Other injury mechanisms include an internal rotary force applied to a femur on a fixed weight-bearing tibia, an external rotation force with a valgus (outward) force, or a straight anterior force applied to the back of the leg, forcing the tibia forward relative to the femur.
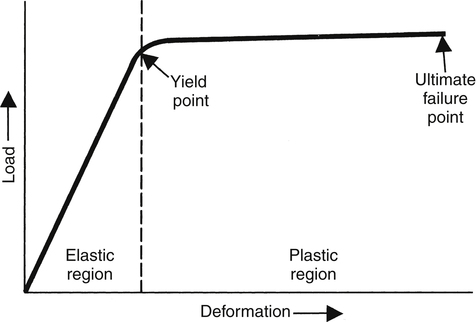
Deformation or a change in shape can occur when an object is loaded. The load–deformation curve describes the relationship between the loading and corresponding degree of deformation (Fig. 16-9). Within the elastic region, the object deforms in direct relation to the force, and returns to the beginning shape once the force is removed. However, at the elastic limit point, the response becomes plastic, resulting in some degree of permanent deformation, even when the force is removed. Also within the plastic region, excessive loading can result in a point of failure. For a bone, this is the point where a fracture occurs. Although excessive acute loading as described can result in damage to the object, the effect of chronic or repetitive loading that commonly occurs in occupational settings is equally problematic.31 Repetitive loading can result in microtrauma to the point of stress. If this persists long enough, a chronic wound, termed a stress-related injury, may occur.26
Common Musculoskeletal Injuries
Soft Tissue Strains and Sprains
Strain and sprain injuries are usually caused by trauma (slip, fall, collision). Strain refers to an injury to a muscle, occurring when a muscle–tendon unit is stretched or overloaded. Sports that incorporate a running component have a relatively high incidence of soft tissue strains, which are quite common injuries treated by PTAs. The injury mechanism begins just before ground impact of the foot; the hamstring muscles contract forcefully to halt the knee extension, which occurs at the end of the recovery phase.20 The action of the hamstrings causes knee flexion to occur and this continues through the early portions of the ground phase. In combination with the hip extension, this knee flexion serves to reduce the braking force (decelerating force), which occurs when the foot strikes the ground. The braking force is a result of a forward moving foot at initial ground impact, analogous to kicking the ground. Hamstring (semitendinosus, semimembranosus, biceps femoris) muscle group injuries are quite common in running activities.20 Hamstring injuries, such as strains or ruptures to soft tissues, result when the muscle concentrically contracts while the muscle continues to undergo stretching during heel contact. A non-sport related soft tissue strain often occurs during slips on surfaces with low coefficient fiction.
Sprain is an injury to a ligament when it is overstretched. The most commonly injured ligaments are located at the ankle, knee, wrist, and low back region. The purpose of ligaments is to hold the adjacent bones together in a normal alignment and prevent abnormal movements by the bones. However, when too much force is applied to a ligament, such as in a fall, the ligaments can be stretched or torn, leading to an injury. Back pain or injury is a leading cause of disability among warehouse and construction workers. The diagnosis of back sprain (whether lumbar or cervical) implies that the ligamentous and capsular structures connecting the facet joints and vertebrae have been damaged.18,31
Rotator Cuff Injury/Shoulder Separation
The primary biomechanical goal of the baseball overhand fastball pitch is to throw a ball at near maximum horizontal velocity with accuracy. Though there are numerous styles of pitching windups, the delivery phase of the overhand pitch (when the ball is accelerated to the release point) tends to have great similarity.14 This complex series of body movements is characterized by the sequential nature in which the body segments contribute to the velocity of the ball. Basically, the lower body begins its contribution with the ground contact of the lead foot at the completion of the stride toward home plate. The forces created by the ground contact, when combined with the forward moving body, cause a rapid rotation of the lower trunk and pelvic area. This rotation is closely followed by the sequential movements of the upper trunk, the upper arm, forearm, and hand. When the hand reaches its maximum velocity the ball is released. The velocity of each successive segment exceeds that of its preceding segment. In other words, these successive segment rotations accept the momentum passed on by the preceding segments and add their momentum before passing it on to the next segment. As momentum builds with each successive segmental contribution, the kinetic energy of the ball increases and reaches a peak at the release point.13
One must consider the biomechanical issues associated with shoulder injuries in overhand baseball pitching. As a result of the very high shoulder rotational velocities attained during the acceleration of the ball toward the catcher, the pitcher must create tremendously large deceleration forces to stop this fast shoulder internal rotation. Relatively speaking, the pitcher spends much time building up shoulder internal rotation to throw the ball with high velocity to the batter, but must stop this motion in a very short time period in order to be ready to field his position. This very short time period for deceleration means the torques around the shoulder joint will be quite high.13,14
The rotator cuff muscles (supraspinatus, infraspinatus, teres major, and subscapularis) are a group of relatively small muscles that are challenged to maintain shoulder integrity and, particularly, to stop shoulder internal rotation and anterolateral distraction. Because the momentum for the shoulder with regard to both the internal rotation and the anterolateral distraction are high, this muscle group is challenged to the extreme with every ball thrown. With the onset of fatigue and the wear and tear of the forces associated with throwing a large number of pitches, injury to this muscle group occurs fairly frequently.14 If the injury is severe, it may very well end a pitcher’s career prematurely, much like an athlete suffering an ACL injury of the knee. Another common shoulder injury involves a disruption of the acromioclavicular (AC) joint. This joint is composed of the collar bone, or clavicle, and the highest portion of the shoulder blade, the acromion of the scapula. These two bones meet on top of the shoulder and form the AC joint, as mentioned earlier.13,17 The most common cause of shoulder separation, or AC joint disruption, is a direct fall onto the shoulder. This fall injures the ligaments that provide stability to the joint. The laxity that results allows a degree of separation between the acromion and the clavicle. The degree of separation can range from mild to severe with a noticeable deformity depending on the momentum–impulse relationship. Treatment of this condition can vary from conservative management with a period of immobility followed by gentle shoulder strengthening, to surgery.
Low Back Injury
The two most serious leg or squat lifting errors are descending too rapidly and allowing the trunk to flex too far forward during the descent phase. Rapid descent should be avoided because it allows an excessive amount of momentum or kinetic energy to be generated, which the muscles may not be able to overcome when challenged to halt and then reverse this motion. The faster an individual descends, the more muscle force required to reverse this direction. If the person is lifting at a resistance close to his or her maximum or is fatigued, it is likely at best that the ascent phase will not be successfully completed, or at worst an injury will occur.15
When the individual allows the trunk to flex too far forward, the forces occurring in the low back are greatly increased over those associated with a more upright posture. The reason for this is rather simple. The trunk can be considered a lever with a fulcrum or rotational axis formed in the lumbar area of the vertebral column. When this lever is rotated forward into flexion from a more vertical trunk posture, the line of action of the resistive force of the patient, not to mention the trunk weight itself, is moved from an orientation directly through the vertebral bodies to one very far forward of them.15
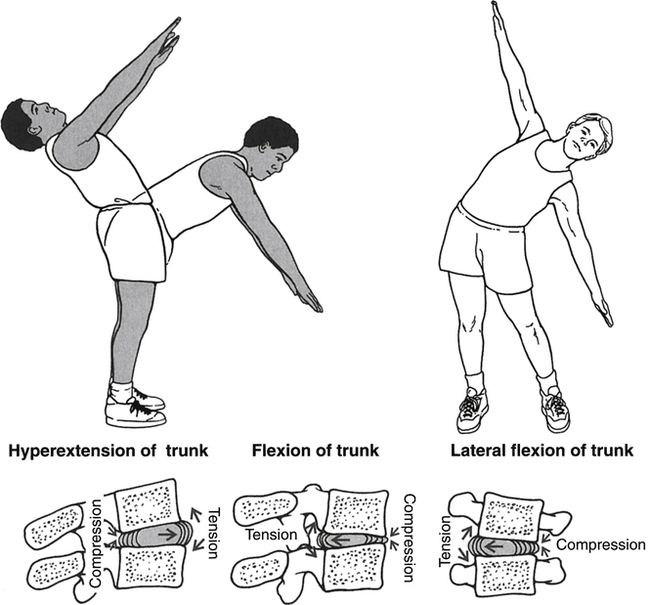
The shifting of the line of action of the resistive forces to this extreme position causes the torque (force of the weight of the barbell and trunk and head segment multiplied times the distance from this line to the lumbar vertebrae) to increase to very high levels. With the increased torque, the type and magnitudes of forces applied to the cartilaginous vertebral discs, which separate the bony vertebral bodies, are radically different from those applied while standing erect. Generally, the anterior portion of two adjacent vertebral bodies (i.e., L4-L5) are forced together, a compressive force, while the posterior aspect of these same bones are forced apart by a tensile force (Fig. 16-10).
ADVANCES IN BIOMECHANICS
Prosthesis design has made incredible advances in functionality. Today, an amputee who is physically active and participates in recreational sports may possess a variety of prostheses designed for a specific activity or sport. Today, prostheses are being fitted with microprocessors that produce a limb classified as artificial intelligence. The prosthesis has the ability to alter position based on feedback from the terrain. Springs and cables are being replaced with pneumatics and hydraulics. The combination of microprocessors and hydraulics produces a more efficient gait and improved balance characteristics compared with traditional prosthetic joints (Fig. 16-11).

Another area that has changed considerably is wheelchair design and wheelchair propulsion mechanics. Patented measuring devices are beginning to emerge in the field as a tool for physical therapy clinics to use for measuring upper extremity joint forces and muscle moments—tools that have been elusive in the past. With today’s biomechanical instrumentation, a manual wheelchair user can visit a rehabilitation professional who has the ability to analyze the individual’s propulsion technique and make adjustments to the user’s mechanics to reduce the force that contributes to acute and chronic shoulder pain or injury. Minor changes to wheelchair setup can impact the ease with which the user can propel the chair, ultimately resulting in improvements to well-being and possibly injury avoidance. During the wheelchair setup process, new instrumentation technology enables the clinician to measure and detect impact. Finally, the force sensor is used to teach a patient how to propel a wheelchair in the most efficient manner. Propulsion training is used to optimize pushing style by reducing the force and frequency of pushes.8,22
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]16
Biomechanical Basis for Movement
Mitchell A. Collins and Michael Hales
1. Define and apply biomechanical concepts in the description of rudimentary movement patterns.
2. Discuss the difference between the kinematics and kinetics of movement.
3. Identify and discuss the kinematic principles as related to movement in a rehabilitation setting.
4. Discuss both the linear and angular kinematics and kinetics of movement, and explain how angular motion translates to linear movements.
5. Describe the differences among the different levers, and explain the concept of mechanical advantage as related to levers.
6. Describe Newton’s laws of motion.
7. Identify and discuss the different forces that act on objects and how the forces affect movement.
8. Discuss the concepts of mechanical loading, and describe how loading is associated with different types of injuries.
9. Discuss the principles of mechanical energy.
10. Describe the concept of equilibrium and identify the factors that contribute to stability.
Biomechanics is the study of the internal and external forces acting on the body and the effects these forces produce. The data obtained from biomechanical research provide a great deal of insight into human movement interactions in fields such as physical and occupational therapy, sports medicine, human factors, prosthetics, orthotics, and ergonomics.12,31 Clinical biomechanics, a subdiscipline, provides direct measures of human motion which influence our knowledge of injury mechanics, rehabilitation, treatment, and prevention. This information can directly affect how a physical therapist assistant (PTA) rehabilitates a patient, an orthopedist repairs a broken limb or ruptured ligament, an athletic trainer implements modalities for treatment, or a clinician evaluates an individual’s gait.19,21,24
Biomechanics can provide the health professional with a better understanding and a broadened knowledge of the causes and degrees of severity associated with an injury. In order to improve upon a current rehabilitative technique, repair procedure or treatment process, the mechanics associated with the causation of the injury must be fully understood. To help the health professional accomplish this task, several factors need consideration when determining the cause and severity of an injury36:
How much force was applied? (magnitude)
Where on the body was the force applied? (location)
Where was the force directed? (direction)
How long was the force applied? (duration)
How often was the force applied? (frequency)
The major role of a PTA revolves around both the causes and effects of human motion and therefore it is imperative to have a fundamental understanding of the mechanical basis for whole body or segmental movement. Since biomechanics is concerned with the effects of forces on the human body, biomechanical principles are involved when a force is present. The following chapter will offer an overview of the science of biomechanics with practical applications for the PTA.
REFERENCE TERMINOLOGY
To facilitate the process of describing human movement, standardized terminology has been adopted to identify body positions and directions of motion (Box 16-1). Movements are defined based on a reference or starting position often referred to as the anatomic position (Fig. 16-1, A), which is a standing position with arms at one’s side and palms facing forward. From the anatomic position, three imaginary cardinal planes bisect the body along three dimensions (Fig. 16-1, B). The transverse or horizontal plane segments the body into upper and lower parts; the frontal or coronal plane separates the body into front and back parts; and the sagittal or anteroposterior plane divides the body into right and left parts. It is important to note that the planes do not necessarily divide the body into equal parts. However, when the segments are equal, the mid-intersection point of the transverse, frontal, and sagittal planes is referred to as the center of mass (COM) or center of gravity (COG). Although human movement is not restricted to a single plane, most named movements (e.g., flexion and abduction) are described based on the three cardinal planes.
BOX 16-1 Basic Directional Terms Used to Describe Body Parts or Other Objects in Relation to the Body
Movements in the transverse plane occur around the longitudinal axis, which runs superiorly–inferiorly while perpendicularly intersecting the transverse plane. These movements include medial and lateral rotation of the leg, thigh, and shoulder; supination and pronation of the forearm; and horizontal abduction and adduction of the shoulder. Movements in the frontal plane occur around the sagittal axis, which runs anteriorly–posteriorly while perpendicularly intersecting the frontal plane. These movements include abduction and adduction of the shoulder and hip, lateral flexion of the neck and trunk, elevation and depression of the shoulder girdle, and inversion and eversion of the foot. Movements in the sagittal plane occur around the frontal axis, which runs from left to right while perpendicularly intersecting the sagittal plane. These movements include flexion and extension of the knee, hip, trunk, elbow, shoulder, and neck; and dorsiflexion and plantar flexion of the foot as well as hyperextension movements. A key role of the PTA is to facilitate patient rehabilitation through the incorporation of various exercises using basic movement patterns. Therefore it is important to be familiar with the appropriate terminology for these movements (Fig. 16-2).
BASIC CONCEPTS
Pressure (p) is a measure of the distribution of a force over a given area (force/area), and it is expressed in newtons per meter2 (N/m2). An example of the concept of pressure in a rehabilitation setting is the development of decubitus ulcers that commonly occur among diabetics.3,32,38 Innovations in shoe design help dissipate the forces applied to the foot over a larger area (e.g., reduced pressure) during locomotion, thus minimizing soft-tissue damage and the incidence of ulceration.6,10,35
BIOMECHANICAL PRINCIPLES
Statics and Dynamics
Linear and Angular Motion
Angular motion is the measurement of rotation about an axis of a rigid lever and is quantified through the use of a polar coordinate system. This is generally represented in the human body by body segments; an example is the upper arm rotating about a joint (axis of rotation) such as the shoulder. By tracking over time how the lever, as established by its endpoints (for the upper arm these would be represented by a line connecting the shoulder and elbow), rotates around its proximal joint (the shoulder), one can determine angular positional changes of the lever, rotational velocities of the lever about the joint, and increases/decreases in rotational velocity. These angular measures describe the quality of motion generated angularly by an individual performing an activity of daily living (ADL), occupational activity, or exercise. This is important because there is a direct link between the quality of angular motion of body segments or levers and the potential for overuse injuries to the subsequent joints. For example, the faster the forearm/racket combination is rotating or extending about the elbow at the instant before impact in a tennis serve, the faster the racket is moving linearly at the moment of impact with the ball. The faster the racket head is moving linearly at impact, the greater the momentum or force imparted to the tennis ball by the athlete. Conversely, because of the high action force and moment, the greater the reaction force and moment imposed on the joints, which could lead to inflammation of the lateral epicondyle (tennis elbow) if poor service mechanics are demonstrated.22 The rotation of the forearm about the elbow is due in part to the contraction of the muscles (triceps group), which causes acceleration in the direction of elbow extension. The linear force of the triceps tendon pulling on the ulna generates a torque or rotational force. The greater the torque produced by the muscles, the greater the angular acceleration generated, leading to changes in angular velocity that lead to changes in angular position.
Kinematics and Kinetics
An understanding of kinematic principles is extremely important to PTAs. Analysis of motion can facilitate the determination of the etiology of injury, extent of damage, and assessment of the effectiveness of treatment. Historically, researchers have studied injuries in sport settings, but the same applications are pertinent to nonathletic settings, such as gait analysis of individuals with lower extremity joint injury or joint replacement.7,9,11,16,27,28 Thus it is imperative for PTAs to be knowledgeable about normal movement patterns from a kinematic perspective to facilitate the recognition of abnormal movements of rehabilitating patients.
Newton’s Laws of Motion
Newton’s first law of motion is commonly referred to as the law of inertia, which states:
“A body remains in a state of rest, or of uniform motion in a straight line, unless it is compelled to change that state by forces impressed on it.”5
[/not-level-membership-for-orthopaedics-category]
