Benign Lesions of the Groin and the Canal of Nuck
Hidradenitis and Other Groin Lesions
The most common lesions the gynecologist will encounter in the groin are enlarged lymph nodes, usually secondary to drainage from the inferior extremity or the neighboring vulva. These rarely require surgical treatment. However, an enlarging solitary mass in the groin, particularly without any identifiable cause, requires exploration and possible excisional biopsy. Differential diagnoses include enlarging lymph node(s), myoma, and femoral hernia. Here, knowledge of the precise anatomy of the femoral triangle is essential. Draining sinuses involving the vulva or the groin may be associated with a variety of disorders. Excisional biopsy may be required to make a diagnosis (Fig. 77–1A through D). Clearly, venereal causes should be excluded first by blood tests, smears, and punch biopsy. Disorders such as syphilis, lymphopathia venerea, and lymphogranuloma inguinale may be associated with sinus-like purulent drainage from matter and enlarged groin nodes. Treatment of these conditions is medical. Tuberculosis also may be associated with draining vulvar and inguinal sinuses. Again, this disorder may require that a generous excisional biopsy be performed and a portion of the tissue be sent for culture, while the remainder is sent to pathology for routine and acid-fast stains. Finally, infection of the apocrine sweat glands (hidradenitis) leads to persistent and chronic purulent draining sinuses in the vulva and groin (Fig. 77–2A through C). Additionally, this disorder may be seen in the axilla. These modified sweat glands may penetrate deeply into the underling stroma and typically plunge into the fat. Treatments for this disorder consist of antibiotics, retinoids, and/or surgery. Surgical excision is wide, with deep margins to eliminate the infected vulvar and inguinal tissues (Fig. 77–3A, B). The wounds may be left open after excision. In the latter instance, healing, of course, is by secondary intention (Fig. 77–3C through H). The wound site initially should be covered with wet-to-dry dressings. Longer term, the patient should sit in salt water (Instant Ocean) tub baths 3 times daily and should cover the operative site with silver sulfadiazine (Silvadene) cream. Alternatively, excised sites may be closed if the margins can be mobilized without undue tension (Fig. 77–4A through I). The patient should be placed on antibiotics (after the wound is cultured) and in Instant Ocean tub soaks 2 or 3 times daily.
Lesions of the Canal of Nuck
Unilateral swelling of the labium majus may be due to a variety of nonsurgical disorders. The absence of inflammation and early pain selects out many nonsurgical causes. Several common surgical disorders should be borne in mind: cyst of the canal of Nuck, hernia into the canal of Nuck, myoma, and lipoma originating from structures in and around the canal. Transillumination may aid in the differentiation of a cystic from a solid mass preoperatively. Exploration, removal, and, in the case of hernia, correction are performed by making a vertical incision into the labium majus (Fig. 77–5A). The incision should be made above and to the lateral or medial side of the lesion. Once the subcutaneous tissue has been reached, 0 Vicryl traction sutures or Allis clamps are placed at the upper and lower margins of the mass. The anterior and lateral margins of the mass are completely dissected (Fig. 77–5B). Blood vessels are clamped and suture-ligated with 3-0 or 4-0 Vicryl. Next, the medial, posterior, and inferior margins of the mass are freed. The mass is carefully entered to ensure that no underlying intestine is present. If the mass is solid (e.g., a lipoma), it is simply excised (Fig. 77–5C). If the mass is cystic, the final upper margin of the mass is dissected and the upper opening is closed with a 3-0 nylon purse string suture, after which the entire cystic mass is excised. The wound is closed in layers with 3-0 Vicryl sutures (Fig. 77–5D, E). The skin likewise is closed with 3-0 Vicryl sutures. The wound is dressed with a nonadherent dressing covered by a pressure dressing and is taped.
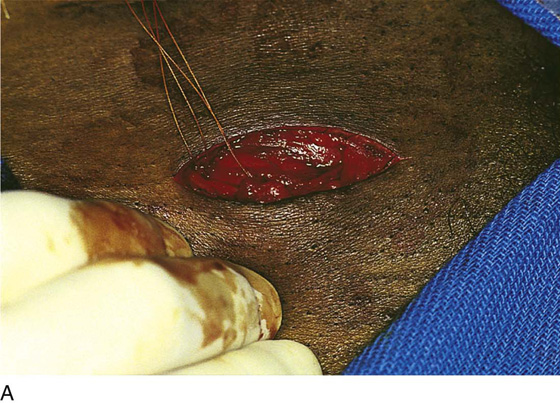

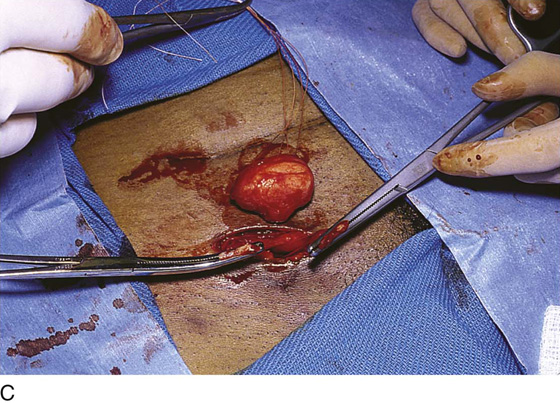
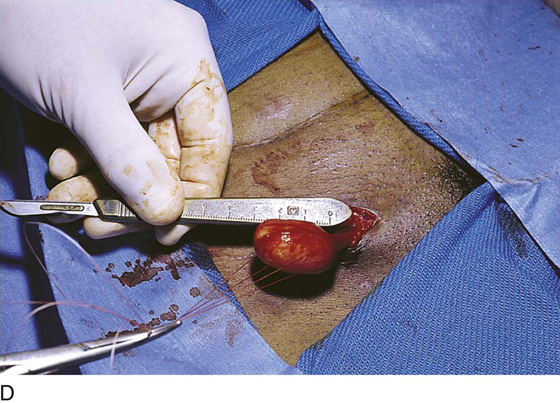
FIGURE 77–1 A. This patient presented with a painful, firm, 3-cm lesion in the left groin. Inspection revealed no vulvar or inferior extremity lesion to account for what was thought to be an enlarged inguinal lymph node. Exploration of the groin was indicated. A 3- to 4-cm incision is made in the groin over the lesion. B. The incision is carried deeply into the fat. Hemostasis is secured with mosquito clamps and 3-0 Vicryl suture-ligatures. Retraction is obtained with the use of vein retractors. C. The mass is isolated and cut out with Metzenbaum scissors. The base is clamped with mosquito clamps. It is obvious that the mass is not a lymph node but instead is a myoma. D. The myoma measures 2½ cm and was proved by histologic evaluation to be benign. The wound is closed in layers with 3-0 or 4-0 Vicryl sutures in interrupted fashion.

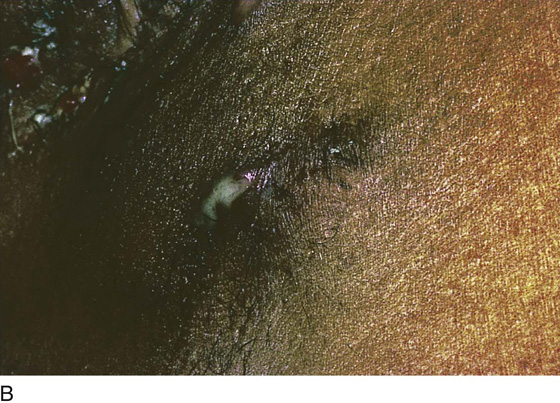
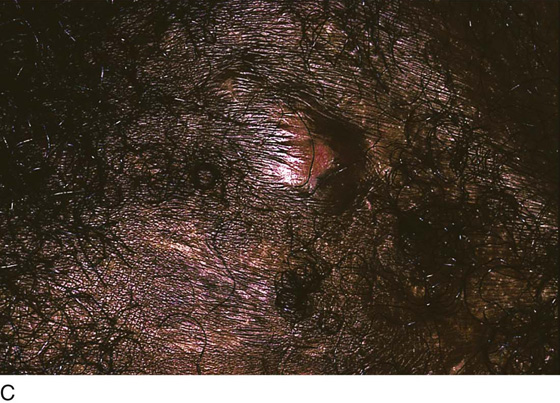
FIGURE 77–2 A. This patient suffered from persistent and recurring abscesses and draining sinuses through the mons and the groin. The appearance, together with the history, is highly suggestive of hidradenitis. A deep-wedge biopsy in the mons confirmed the diagnosis histologically. B. Close-up photo of the groin of another patient with hidradenitis. Note the pus draining from a deeply probed sinus. C. Another area in the groin of the patient shown in part B. The elevated “blister” of skin represents a sinus, which will shortly erupt and drain.
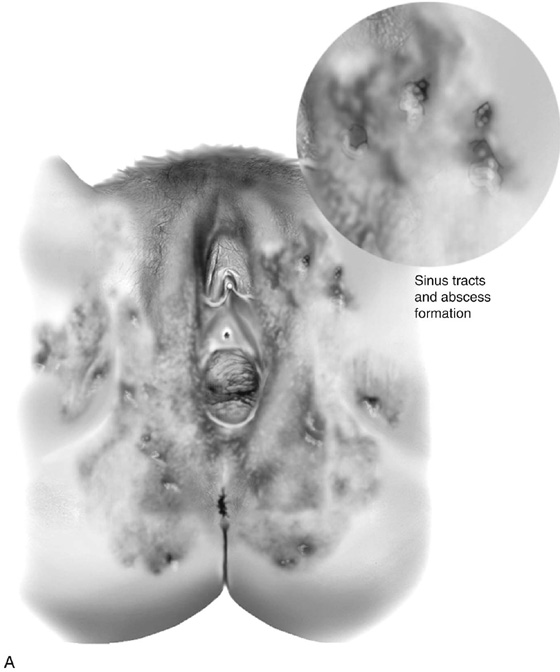
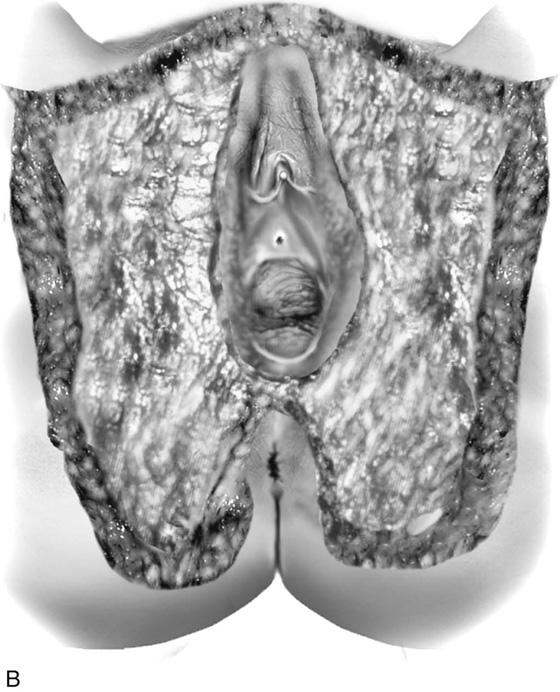
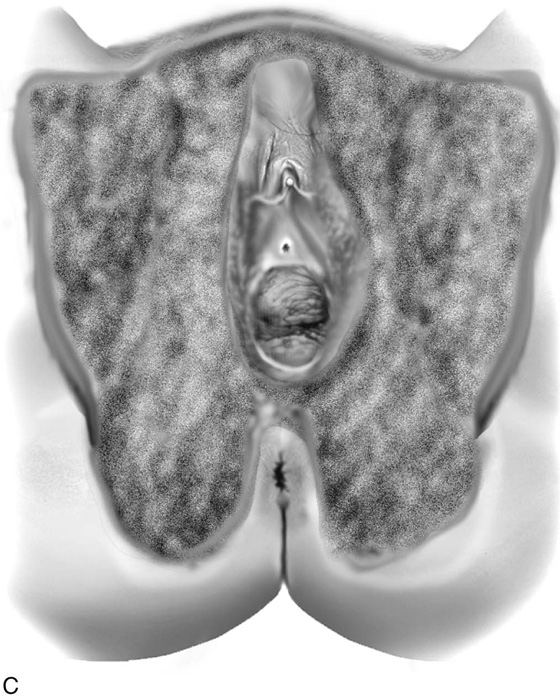




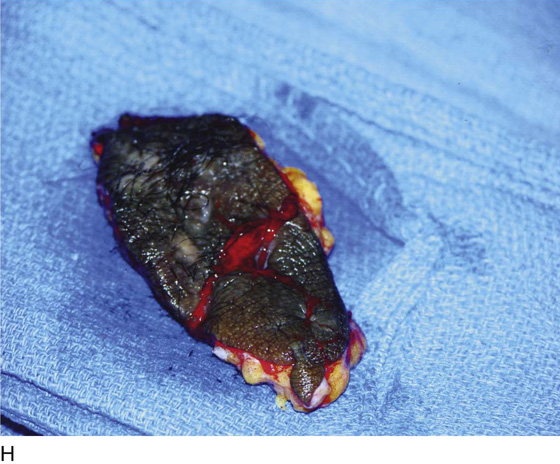
FIGURE 77–3 A. Hidradenitis must be widely and deeply excised. B. The entire affected area, including the mons and the groin, must be dissected, including the upper (ICM) layer of the subcutaneous tissue, and removed en masse. Less radical treatment invariably will result in recurrence. C. The wound must be carefully managed in the postoperative course. Because it cannot be grafted, it should heal from the bottom upward by granulation. All patients are covered with antibiotics administered first 1 hour preoperatively. Oral clindamycin is administered postoperatively for 1 week (300 mg every 6 hours). D. This patient presented with chronic draining sinuses emanating from the labia, mons, and groin. E. Close-up view of blebs, open lesions, and fissures. F. A deep initial incision is made into the right groin and is carried into the lower half of the right labium majus. G. The excision has been completed, thereby removing the sinus tracts and the underlying sweat glands. H. The large excised gross pathology specimen is shown here.

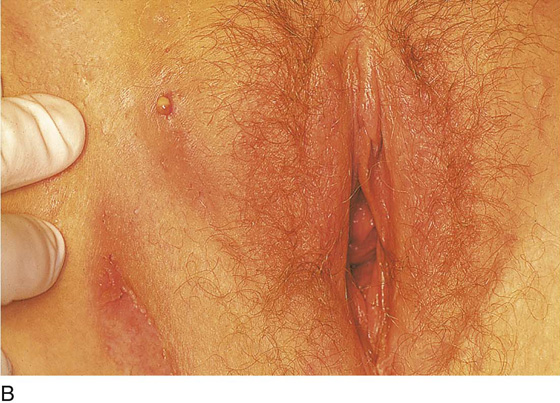


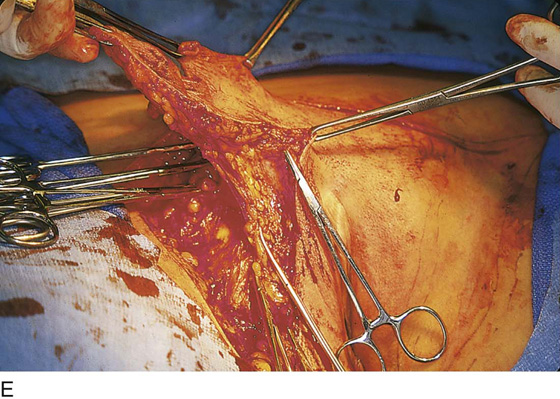

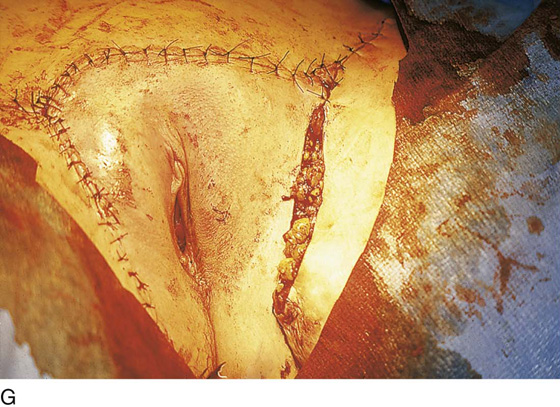

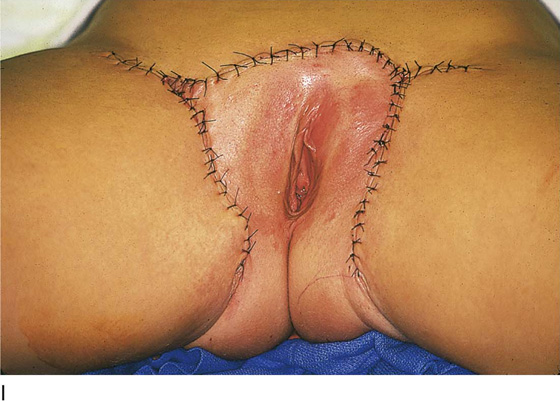
FIGURE 77–4 A. The patient in the lithotomy position shows scarring, sinus formation in the vulva, groin, and mons and buttock. B. Close-up view of a draining vulvar lesion and scar formation in the crural region. The pus tested positive for Staphylococcus aureus.C. A cotton-tipped application stick is placed into a draining sinus tract. D. The treatment plan calls for deep and wide excision of the recurrently infected tissues. The knife-cut outlines the wide margins of the proposed tissue resection. E. The resection begins in the right groin and proceeds from lateral to medial. F. The tissue resection is finished on the right side of the patient. Unaffected areas are spared. G. The wound is partially closed without any skin edge tension. H. The closed wound is covered with Xeroform fine-mesh gauze, which, in turn, is covered with sterile gauze. I. The closure of this extensive excision is complete. All diseased tissue has been deeply cut away and sent to pathology.
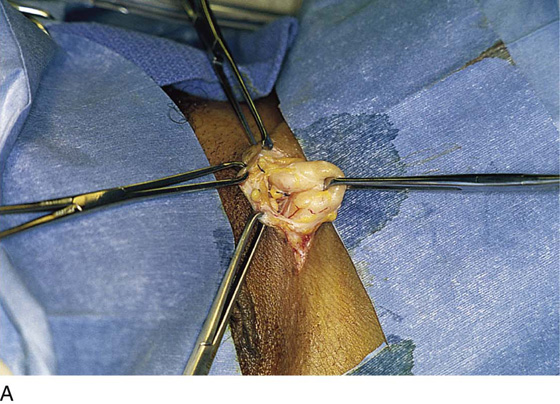
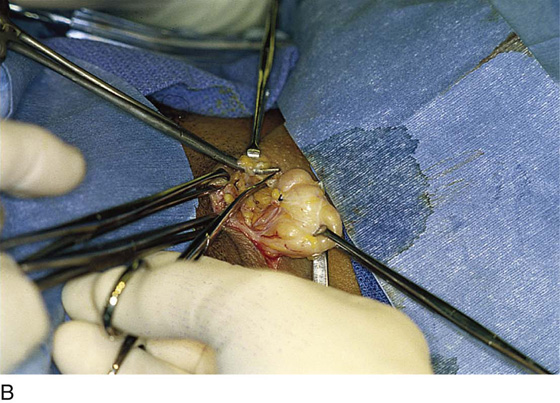

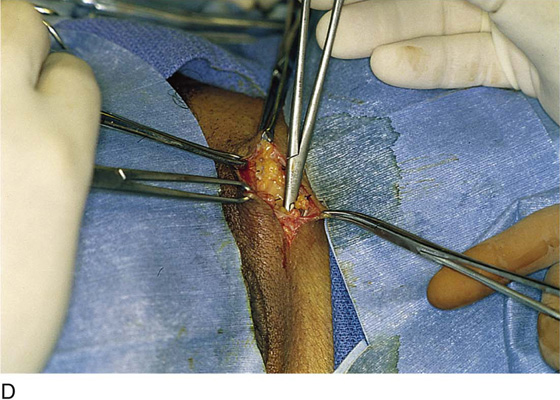

FIGURE 77–5 A. A deep, soft mass was palpated in the upper portion of the labium majus. A vertical incision is made above the mass and is carried deeply into the fat. The margins of the wound are retracted with 0 Vicryl traction sutures or with Allis clamps. An Allis clamp grasps the upper portion of the mass, and traction is placed on the mass. In this case, the lesion was not a cyst but rather a lipoma. B. The tissues surrounding the mass are clamped with tonsil clamps and are suture-ligated. The lesion is freed from the surrounding tissue by sharp dissection with the use of Metzenbaum scissors. C. The mass is delivered from the incision. Careful inspection reveals no herniated intestine. D. The fat is closed with interrupted 3-0 Vicryl sutures. The skin is likewise sutured with interrupted 3-0 Vicryl sutures. E. The lipoma is sent to pathology to ensure that it is benign.






